

A woman aged 51 years was referred to our endocrinology outpatient clinic because of excessive hair growth for seven years. The Ferriman–Gallwey hirsutism score was 36. No abdominal palpable masses were found. Mild clitoromegaly was observed in the pelvic examination. Her hormonal evaluation revealed total testosterone (T) of 761.15 ng/dL (14.2–73.1 ng/dL), dehydroepiandrosterone sulfate (DHEA-SO4) of 160 μg/dL (35–430 μg/dL), 17-hydroxiprogesteron of 3.49 ng/mL, follicle-stimulating hormone of 1.1 IU/L (23.9–119.1 IU/L), luteinizing hormone of 0.2 IU/L (16.3–54.8 IU/L), and estradiol of 56 pg/mL (14.4–44.5 pg/mL). After a 1 mg dose of dexamethasone at night, plasma cortisol levels returned to a normal level of 0.7 mg/dL. A transvaginal ultrasound (US) examination showed uterine fibroid with normal ovaries. Magnetic resonance imaging (MRI) of the abdomen and pelvis revealed that all other organs including the adrenal gland and ovaries were normal (Figure 1, 2).
Figure 1.
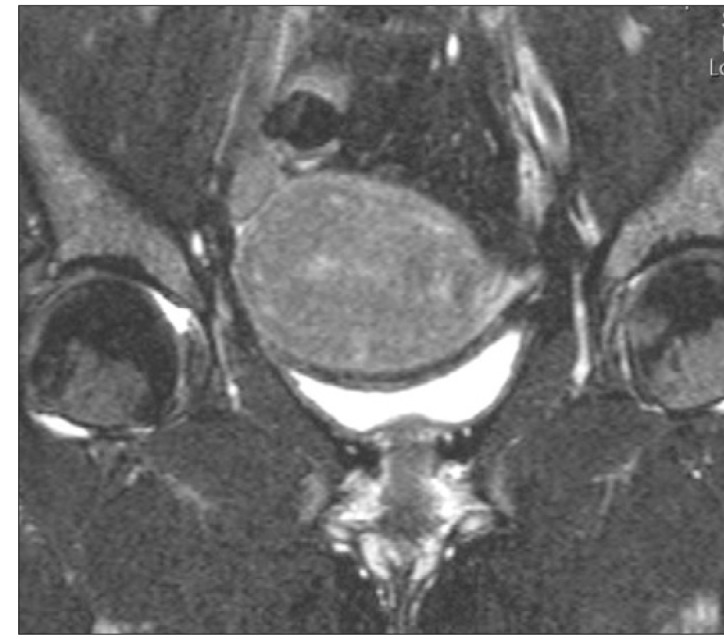
Fat-suppressed T2-weighted coronal pelvic magnetic resonance image shows normal uterus and adnexal structures
Figure 2.

T2-weighted coronal pelvic magnetic resonance image shows normal adrenal gland
Answer
Clinical findings of severe virilization in women with markedly increased serum androgens are indicative of androgen-secreting tumors, which may arise from the ovaries or adrenals (1). Leydig cell tumors are functioning testosterone-producing benign ovarian tumors that lead to hyperandrogenism and virilization (2). Diagnosis is often very challenging because Leydig cell tumors are small and are frequently missed with conventional imaging techniques owing to their size (3).
Our patient’s DHEA-SO4 levels were within the normal range, whereas the testosterone and estrogen levels were significantly elevated, which was suggestive of a tumor of ovarian origin. No lesion was observed in the transvaginal US and pelvic MRI. Selective ovarian venous hormonal catheterization (SOVHS) was used to assist diagnosis and localization of androgen-secreting tumors. SOVHS is recommended when tumor identification remains unclear (4). When small androgen-producing tumors are suspected clinically and biochemically in postmenopausal patients, laparoscopic or open bilateral adnexectomy is recommended in the literature because conventional imaging is often unable to detect this variety of tumor (5, 6). Localization of the tumor was provided according to the hormonal findings obtained with SOVHS. An alternative method that can assist the localization of androgen-producing tumors is preoperative measurement of T levels in the ovarian vein (7).
Hyperandrogenism is frequently observed in polycystic ovary syndrome (PCOS). Speed of virilization onset (<2 years) or late onset in life is a better predictor of neoplasm than androgen levels (8). Our patient was diagnosed with PCOS and received treatment accordingly. However, she developed hyperandrogenism associated with serious atherosclerotic vascular disease. Six months later she underwent surgery after being diagnosed with an ovarian tumor (Figure 3, 4). The differential diagnosis of PCOS and ovarian or adrenal tumors must be successfully evaluated and SOVHS should be remembered in challenging tumor localization.
Figure 3.
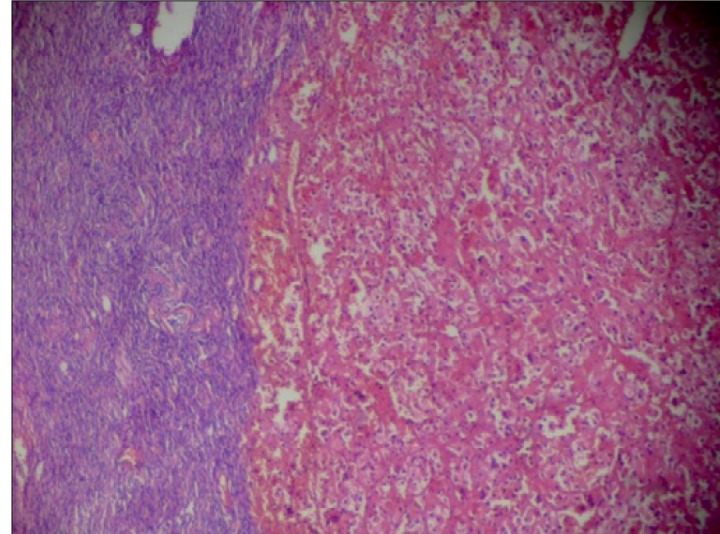
Normal ovarian tissue observed on the left side. Eosinophilic and vacuolated cytoplasm of tumor cells was seen on the right side (10X, H.E.)
Figure 4.
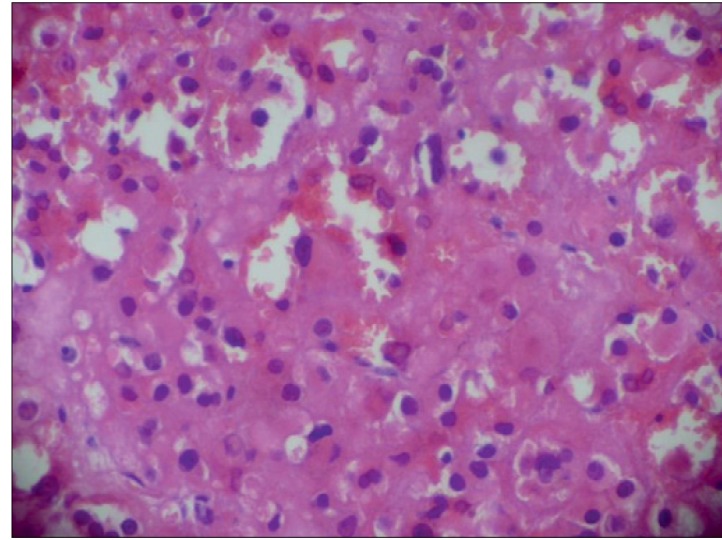
Eosinophilic cytoplasm of tumor cells and Reinke crystals in the cytoplasm were observed (20×, H.E.)
This report demonstrates effective preoperative use of SOVHS in localization of an androgen-secreting ovarian tumor that could not be identified using conventional imaging. Early diagnosis of this tumor is very important to decrease the risk of cardiovascular and cerebrovascular events.
References
- 1.Surrey ES, de Ziegler D, Gambone JC, Judd HL. Preoperative localization of androgen-secreting tumors: clinical, endocrinologic, and radiologic evaluation of ten patients. Am J Obstet Gynecol. 1988;158:1313–22. doi: 10.1016/0002-9378(88)90362-6. http://dx.doi.org/10.1016/0002-9378(88)90362-6. [DOI] [PubMed] [Google Scholar]
- 2.Takeuchi S, Ishihara N, Ohbayashi C, Itoh H, Maruo T. Stromal Leydig cell tumor of the ovary. Case report and literature review. Int J Gynecol Pathol. 1999;18:178–82. doi: 10.1097/00004347-199904000-00014. http://dx.doi.org/10.1097/00004347-199904000-00014. [DOI] [PubMed] [Google Scholar]
- 3.Pugeat M, Mirakian P, Dutrieux-Berger N. Androgen secreting ovarian neoplasm. In: Azziz R, Nestler JE, Dewailly D, editors. Androgen excess disorders in women. New York: Lippincott-Raven; 1997. pp. 555–68. [Google Scholar]
- 4.Dickerson RD, Putman MJ, Black ME, Pinto KR, Diamond NG, Marynick S, et al. Selective ovarian vein sampling to localize a Leydig cell tumor. Fertil Steril. 2005;84:218. doi: 10.1016/j.fertnstert.2004.12.055. http://dx.doi.org/10.1016/j.fertnstert.2004.12.055. [DOI] [PubMed] [Google Scholar]
- 5.Sanz OA, Martinez PR, Guarch RT, Go-i MJ, Alcazar JL. Bilateral Leydig cell tumour of the ovary: a rare cause of virilization in postmenopausal patient. Maturitas. 2007;57:214–6. doi: 10.1016/j.maturitas.2006.11.013. http://dx.doi.org/10.1016/j.maturitas.2006.11.013. [DOI] [PubMed] [Google Scholar]
- 6.Sanyal D, Taylor WG, Otter MI. Bilateral thecomata in ovaries with normal ultrasonographic and radiological appearances, presenting with postmenopausal hirsutism and virilism. J Obstet Gynaecol. 2003;23:457–8. doi: 10.1080/0144361031000122796. http://dx.doi.org/10.1080/0144361031000122796. [DOI] [PubMed] [Google Scholar]
- 7.Judd HL, Spore WW, Talner LB, Rigg LA, Yen SS, Benirschke K, et al. Preoperative localization of a testosterone-secreting ovarian tumor by retrograde venous catheterization and selective sampling. Am J Obstet Gynecol. 1974;120:91–6. doi: 10.1016/0002-9378(74)90184-7. http://dx.doi.org/10.1016/0002-9378(74)90184-7. [DOI] [PubMed] [Google Scholar]
- 8.Derksen J, Nagesser SK, Meinders AE, Haak HR, van de Velde CJ. Identification of virilizing adrenal tumors in hirsute women. N Engl J Med. 1994;331:968–73. doi: 10.1056/NEJM199410133311502. http://dx.doi.org/10.1056/NEJM199410133311502. [DOI] [PubMed] [Google Scholar]