

Abstract
Background
The effectiveness of print-based health promotion materials is dependent on their readability. This study aimed to assess the characteristics of print-based oral health information literature publically available in Tasmania, Australia.
Methods
Oral health education brochures were collected from 11 dental clinics across Tasmania and assessed for structure and format, content and readability. Reading level was calculated using three widely-used measures: Flesch-Kincaid Grade Level (FKGL), Flesch Reading Ease, and Simple Measure of Gobbledygook (SMOG) reading grade level.
Results
The FKGL of the 67 brochures sampled ranged from grade 3 to 13. The grade level for government health department brochures (n = 14) ranged from grade 4 to 11 (5.6 ± 1.8). Reading levels for materials produced by commercial sources (n = 22) ranged from 3 to 13 (8.3 ± 2.1), those from professional associations (n = 22) ranged from grade 7 to 11 (8.9 ± 0.9) and brochures produced by other sources (n = 9) ranged from 5 to 10 (7.6 ± 1.5). The SMOG test was positively correlated with the FKGL (rs = 0.92, p < 0.001) though consistently rated materials 2-3 grades higher. The reading level required to comprehend brochures published by government sources were, on average, lower than those from commercial, professional and other sources. Government materials were also more likely to contain fewer words and professional jargon terms than brochures from the other sources.
Conclusion
A range of oral health information brochures were publically available for patients in both public and private dental clinics. However, their readability characteristics differed. Many brochures required a reading skill level higher than that suited to a large proportion of the Tasmanian population. Readability and other characteristics of oral health education materials should be assessed to ensure their suitability for use with patients, especially those suspected of having low literacy skills.
Keywords: Oral health, Health education and promotion materials, Dental, Health literacy, Readability
Background
Information about oral health is provided in a variety of forms and obtained from a range of sources including the media and more directly from oral health practitioners. Verbal messages from a dentist may be reinforced through a printed handout or brochure provided to a patient regarding ongoing care. Most public and private dental clinics make printed information freely available to patients to promote oral health. It is important that printed educational material should be pitched at an appropriate level for a particular target audience and be “fit for purpose”. Research suggests however, that health educational materials are often designed at a level beyond that which could be readily understood by the average adult or the majority of the population [1].
Wilson [2] assessed the readability of 35 patient education information brochures used in community healthcare centres serving low-income populations. The author found that these were written at a level higher than that for an average patient to understand [2]. Alexander [3] assessed the reading level of 24 general dental educational materials and reported that over 40 % of them were written at a grade level higher than recommended. Hendrickson and colleagues [4] assessed readability as well as thoroughness, textual framework, and the terminology used in 27 paediatric oral health materials and found both conflicting information and variation in readability across publishers [4]. Noticeably, there has been limited research published on the readability of print based oral health information made available in Australia. Our search recovered only three recent studies [5–7] which was limited to information about paediatric oral health.
Systematic reviews [8, 9] have demonstrated a significant association between socioeconomic status (determined by income, education and occupational background) and dental caries. There is a similar association between low oral health literacy and self-reported poor oral health [10–12]. Given that health literacy contributes to oral health literacy, it is of concern that the Australian adult literacy survey found that nearly 60 % of Australian and 63 % of Tasmanian 15-74 year olds were not able to demonstrate the minimum level of health literacy “to meet the complex demands of everyday life” [13]. Compared to other states, Tasmania’s population of around half a million persons is one of the least advantaged in term of socio-economic status. It is widely disbursed and ageing rapidly; factors that all contribute to poorer oral health outcomes [14]. Within this context, the aim of this study was to assess the readability characteristics of print-based oral health information literature available to the Tasmanian public. The results may assist the future development and use of these materials to better tailor them to the literacy level of a particular target audience.
Methods
Sampling
Oral health brochures readily available to patients were collected from a convenient sampling of public and private general dental clinics located in large and small towns in Tasmania. A member of the research team initially visited 7 clinics and collected all the materials that were made readily available to the public free of charge. A verbal request was made to another 4 clinics to mail all available oral health brochures to the research team. Collection ceased when no new brochure was identified in the yield from the last site sampled.
A total of 238 information brochures were collected and the following inclusion criteria were applied to each: written in the English language; aimed at patients and not health professionals/educators; oral health specific rather than general health or disease conditions that may impact oral health; and were in current use.
Figure 1 shows the design of the study. After removing duplicates, 67 (28 %) brochures remained and were grouped according to type of publisher: commercial (22), professional associations (22), government departments (14), and other (9) (eg. in-house) sources. The materials were assessed on 20 features across three major attributes: structure and format, content, and readability. Sampled brochures were scanned and converted to plain text Microsoft Word 2010 documents [15] for calculation of word counts and readability analyses.
Fig. 1.
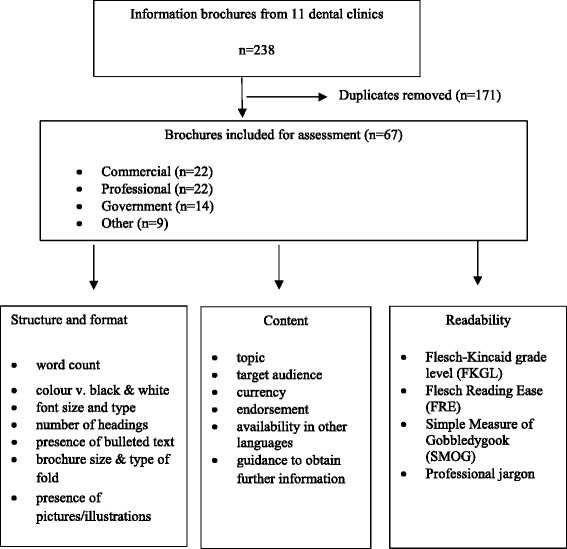
Design of the study
Structure and format
Presentation and layout of brochures can enhance readability and comprehension. Generally, materials that are complex, excessively wordy and or contain extraneous information are less likely to be read and can have less impact than those that are more focussed. Using everyday language, the logical sequencing of information, judicious use of white space, headings, bullets and using devices such as pictures or illustrations can help break up long passages of text, reduce text density and help reinforce key messages and assist understanding [16]. The structure and format of the brochures was evaluated by an assessment of: size of the brochure; type of fold (double fold, tri-fold or gate fold); the presence of bulleted text; number of pictures, use of colour, total word count; font size and type.
Content
This attribute was evaluated using six features that included the broad purpose or content area of the brochure and target audience. Currency of information was assessed by locating the date on which the brochure was last published or reviewed. As a proxy measure for the accuracy and evidence-base of the information presented, we searched for any statement indicating endorsement by an appropriate (non-commercial) dental authority or professional association. Given that our sampling frame included clinics that serviced clients from different cultural backgrounds, we also looked for indicators that the brochure or the information it contained was available in languages other than English. Accepting that most brochures are designed to convey a particular message simply and succinctly rather than provide detailed or extensive coverage of the topic, we also looked for statements that directed the reader to additional sources of information on the topic.
Readability
Readability refers to the degree to which written information can be understood by the reader. The reading level of each brochure was calculated using three widely-used measures. The Flesch-Kincaid Grade Level (FKGL) [17] and the Flesch Reading Ease (FRE) [18] score is calculated by formula based on average sentence length and average number of syllables per word. The Simple Measure of Gobbledygook (SMOG) is a count of polysyllabic words and typically used to analyse short documents [19]. The SMOG score may be calculated manually using a formula or via an on-line calculator [20]. Essentially, the more polysyllabic words, the higher the SMOG score.
Both the FKGL and the SMOG estimate the U.S. primary or secondary school grade level (from 1-12) that a reader would be expected to have completed in order to understand a particular text. These grade levels approximate those in the Australian school system. The FRE test produces a score from a given text that can range from 0 to 100. The higher the score, the easier a text is to read. In general, scores below 30 are “very difficult” and scores above 90 “very easy” to read [18]. The higher the FRE score, the lower the FKGL and SMOG grade level.
Professional jargon refers to words that would be uncommon to an average adult who had not received a health sciences education. Words that were explained in a brochure were not considered as jargon [4]. For this study, we drew upon lists of professional jargon identified by others [3-5] and extracted additional acronyms, dental or medical terms used in the sampled brochures that the research team thought could be difficult to understand. This list of 171 words was sorted alphabetically and five university qualified adults who were not health care professionals were asked to independently identify those words on the list that they found difficult to understand. Any word that more than one person rated as difficult was retained on the final list of 132 “professional jargon” words applied in our analysis.
Statistical analysis
Data for each brochure were recorded in a spreadsheet then analysed using descriptive and inferential statistics available in SPSS 20. Descriptive statistics included, frequency tallies, range, mean, median and standard deviation were used to summarise characteristics related to the structure and format of each brochure as well as readability. A Spearman correlation coefficient was computed to determine the strength of the association between readability measures (Flesch-Kincaid, SMOG, and FRE).
Approval for the study from a research ethical review board was not required as our procedures did not involve the collection of data from humans or any experimental intervention. The study was restricted to a desk-top analysis of publicly available, print-based literature.
Results
Structure and format
Most brochures used standard paper sizes A3 (9), A4 (38) and A5 (2), though 18 were customised. A majority (60 %) of brochures were folded: 11 used a double fold, 21 tri-fold, 5 quad-fold and 3 utilised a gate-fold. The remainder (27) were single page hand-outs.
All except 4 brochures used colour and most (95 %) contained pictures or illustrations. The number of pictures used ranged from 0 to 17 (median: 5 pictures). A majority of brochures (79 %) distributed text under sub-headings (range: 13 (1-14), median: 4) and all but 1 made use of bulleted text. Brochures produced “in-house” were less likely to use pictures and more likely to be produced in black and white.
Word length ranged from 84 to 3856 (median 854 words). The smallest font size was 7 and largest 14. The most frequent font size used was 11 (used in 32 brochures). Ten different font types were used. The most frequently used was Calibri (22) followed by Gillsans MT (13) and DaxOT-light (10). Publishers tended to use one font type for their brochures. For example, Calibri was the preferred font type for all of the brochures sampled from the Australian Dental Association (Table 1).
Table 1.
Structure, format and readability analyses of the brochures
| Number | Publishera | Typeb | Title | Structure and format analyses | Readability analyses | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Target audience | Word count | Font/size | Paper size | Fold | Number of pictures | Professional jargon (instances) | Flesh-Kincaid grade level | Flesh reading ease | SMOG reading level | ||||
| 1 | Colgate | C | Oral health through everyday care | All patients | 193 | DaxOT-Light/10 | A5 | No fold | 6 | 1 | 3.1 | 98.1 | 6 |
| 2 | Colgate | C | Patient information: dental erosion | All patients | 642 | DaxOT-Light/10 | A4 | Trifold | 5 | 1 | 9.1 | 54.3 | 11 |
| 3 | Colgate | C | Oral health for teens and 20s | Teens and 20s | 1759 | DaxOT-Light/12 | Customised | Closed gate | 17 | 1 | 8.8 | 58.3 | 11 |
| 4 | Colgate | C | Patient information: caries free teeth for a healthy smile | All patients | 1032 | DaxOT-Light/10 | A4 | Trifold | 5 | 2 | 7.8 | 63.8 | 11 |
| 5 | Colgate | C | Patient information: oral health for children 3-12 | Parents | 1471 | DaxOT-Light/10 | Customised | Closed gate | 15 | 2 | 7.1 | 69.3 | 10 |
| 6 | Colgate | C | Oral health and diabetes | Diabetic patients | 934 | DaxOT-Light/10 | A4 | Trifold | 2 | 4 | 6.2 | 58.4 | 9 |
| 7 | Colgate | C | Helpful tips to keep your gums healthy | All patients | 787 | DaxOT-Light/11 | A4 | Trifold | 7 | 13 | 8.6 | 55.4 | 10 |
| 8 | Colgate | C | 12 h antibacterial protection against plaque | All patients | 429 | Calibri/7 | Customised | Doublefold | 7 | 6 | 8.8 | 53 | 11 |
| 9 | Colgate | C | Sensitive teeth | Adult patients | 728 | DaxOT-Light/11 | A4 | Trifold | 7 | 10 | 10.7 | 44.9 | 12 |
| 10 | Colgate | C | Patient information: oral care during orthodontic treatment | Parents | 1088 | DaxOT-Light/10 | Customised | Quadfold | 15 | 5 | 6.7 | 70.4 | 9 |
| 11 | Colgate | C | Patient information: oral health for infants and toddlers | Parents | 1449 | DaxOT-Light/10 | Customised | Quadfold | 10 | 0 | 7.8 | 67.1 | 10 |
| 12 | 3M ESPE | C | Winning formula helps prevent tooth decay: clinpro tooth crème | All patients | 528 | HelveticaNeue-Condensed + FZKMUV/11 | A5 | Doublefold | 4 | 8 | 8.4 | 59.8 | 9 |
| 13 | Polident | C | Denture care information booklet | Denture holders | 1039 | StoneSans/10 | Customised | Quadfold | 9 | 0 | 5.3 | 74.9 | 7 |
| 14 | GSK Pronamel | C | Protect teeth against acid wear | Adults | 359 | StoneSans/8 | Customised | Quadfold | 6 | 3 | 7.6 | 58.9 | 10 |
| 15 | GSK biotene | C | Do you suffer from dry mouth | Adults | 1108 | StoneSans/11 | Customised | Closed Gate | 2 | 2 | 7.3 | 65.4 | 9 |
| 16 | GC | C | Tooth Mousse | All patients | 734 | Avenir 35 Light/9 | A4 | Trifold | 5 | 1 | 8 | 63 | 11 |
| 17 | GC | C | GC tooth mousse FAQS | All patients | 744 | Avenir 35 Light/8.5 | A4 | Trifold | 4 | 3 | 7.7 | 64.5 | 10 |
| 18 | GC | C | GC tooth mousse for seniors | Seniors | 815 | Avenir 35 Light/9 | a4 | Trifold | 9 | 4 | 11 | 46.7 | 12 |
| 19 | GC | C | GC tooth mousse for adults | Adults | 731 | Avenir 35 Light/9 | A4 | Trifold | 9 | 2 | 10.9 | 45.8 | 13 |
| 20 | GC | C | GC tooth mousse for children | Parents | 612 | Avenir 35 Light/9 | A4 | Trifold | 9 | 13 | 12.6 | 43.5 | 13 |
| 21 | GC | C | GC tooth mousse plus | All patients | 826 | Avenir 35 Light/9 | A4 | Trifold | 4 | 5 | 10.2 | 51.9 | 12 |
| 22 | Align Technology | C | Straight Talk about cooked teeth: how to reduce your risk of periodontal disease | Teens and Adults | 739 | Avenir-Book/10 | Customised | Quadfold | 6 | 10 | 10.7 | 49.2 | 12 |
| 23 | ANZAOMS | P | TMJ disorders | Adults | 2701 | Times New Roman/12 | A3 | Doublefold | 2 | 18 | 9.9 | 51.8 | 12 |
| 24 | ANZAOMS | P | Wisdom teeth | Adults | 3155 | Calibri/11 | A3 | Doublefold | 4 | 15 | 7.5 | 65.6 | 10 |
| 25 | ANZAOMS | P | Orthognathic surgery | Adults | 3169 | Calibri/11 | A3 | Doublefold | 2 | 15 | 9.5 | 55.2 | 11 |
| 26 | ADA | P | Root canal treatment | Adults | 1834 | Calibri/11 | A4 | No fold | 4 | 15 | 9.8 | 56.4 | 11 |
| 27 | ADA | P | Fissure sealants | All patients | 1367 | Calibri/11 | A4 | No fold | 2 | 9 | 9.4 | 54.8 | 11 |
| 28 | ADA | P | Treatment of gum infections | Adults | 1520 | Calibri/11 | A4 | No fold | 2 | 7 | 9.7 | 54.9 | 11 |
| 29 | ADA | P | Crowns and bridges | Adults | 1474 | Calibri/11 | A4 | No fold | 2 | 7 | 8.7 | 60.9 | 10 |
| 30 | ADA | P | Dental care for babies and young children | Parents | 3447 | Calibri/11 | A3 | Doublefold | 6 | 18 | 7.6 | 66.8 | 10 |
| 31 | ADA | P | Bisphosphonate treatment and oral health | Adults | 1412 | Calibri/11 | A4 | No fold | 2 | 5 | 9.8 | 52.2 | 11 |
| 32 | ADA | P | Disorders of the jaw joint | Adults | 1181 | Calibri/11 | A4 | No fold | 1 | 9 | 9.9 | 53.4 | 11 |
| 33 | ADA | P | Bruxism | Adults | 1315 | Calibri/11 | A4 | No fold | 5 | 13 | 9 | 56.2 | 11 |
| 34 | ADA | P | 7 tips for healthy baby teeth | Parents | 280 | Calibri/7 | Customised | No fold | 1 | 4 | 8.7 | 62.1 | 10 |
| 35 | ADA | P | Cracked tooth syndrome | Adults | 1445 | Calibri/11 | A4 | No fold | 1 | 8 | 7.7 | 67.1 | 10 |
| 36 | ADA | P | Orthodontics | All patients | 1762 | Calibri/11 | A3 | Doublefold | 2 | 12 | 9.1 | 54.3 | 11 |
| 37 | ADA | P | Dental implants | Adults | 3459 | Calibri/11 | A3 | Doublefold | 6 | 4 | 9.3 | 55.6 | 11 |
| 38 | ADA | P | Wisdom teeth | Late Teens and Adults | 2925 | Calibri/11 | A3 | Doublefold | 4 | 10 | 6.9 | 68.8 | 9 |
| 39 | ADA | P | Your oral health and smoking | Late Teens and adults | 1416 | Calibri/11 | A4 | No fold | 5 | 9 | 9.1 | 57.6 | 11 |
| 40 | ADA | P | Home dental care | All patients | 3856 | Calibri/11 | A3 | Doublefold | 7 | 7 | 8 | 66.4 | 9 |
| 41 | ADA | P | Veneers, bonding, bleaching and composite fillings | Adults | 2785 | Calibri/11 | A3 | Doublefold | 9 | 7 | 8.6 | 60.4 | 12 |
| 42 | ADA | P | Dental extractions | Adults | 1833 | Calibri/11 | A4 | No fold | 1 | 9 | 8.6 | 60.9 | 11 |
| 43 | ADA | P | Orofacial pain | Adults | 1714 | Calibri/11 | A4 | No fold | 2 | 10 | 10.9 | 50.5 | 11 |
| 44 | ADA | P | Amalgam fillings for teeth | Adults | 1326 | Calibri/11 | A4 | No fold | 1 | 5 | 9.9 | 52.9 | 10 |
| 45 | OHST | G | Tips for the first dental visit | Parents | 145 | Gillsans MT/11 | Customised | No fold | 3 | 0 | 5.8 | 74.8 | 8 |
| 46 | OHST | G | Give your child’s teeth a healthy start | Parents | 162 | Gillsans MT/11.5 | A4 | Trifold | 12 | 0 | 4.4 | 82.2 | 7 |
| 47 | OHST | G | Free dental care for children and teens | Parents | 168 | Gillsans MT/11 | Customised | No fold | 2 | 0 | 4.5 | 80.3 | 8 |
| 48 | OHST | G | Dental services for adults | Adults | 339 | Gillsans MT/11 | Customised | No fold | 1 | 0 | 6.8 | 66.3 | 9 |
| 49 | OHST | G | Psst give my teeth a healthy start magnetic | Parents | 114 | Gillsans MT/10.5 | Customised | No fold | 10 | 1 | 5.1 | 73.4 | 7 |
| 50 | OHST | G | Smoking and your oral health | Adults and Late teens | 383 | Gillsans MT/12 | A4 | Trifold | 9 | 2 | 4.3 | 74.5 | 7 |
| 51 | OHST | G | Caring for and cleaning your denture | Denture holders | 436 | Gillsans MT/11.5 | A4 | Trifold | 7 | 1 | 5.7 | 70.4 | 9 |
| 52 | OHST | G | Smoking? What’s happening in your mouth? | Late teens and young adults | 150 | Gillsans MT/12 | Customised | No fold | 7 | 1 | 4.6 | 81.6 | 6 |
| 53 | OHST | G | Give your child’s teeth a healthy start: a guide for children 2–5 years | Parents | 168 | Gillsans MT/11 | Customised | No fold | 10 | 1 | 4.9 | 85.7 | 7 |
| 54 | OHST | G | Give your child’s teeth a healthy start: a guide for children 12–24 months | Parents | 204 | Gillsans MT/10 | Customised | No fold | 13 | 1 | 4.4 | 78.1 | 6 |
| 55 | OHST | G | Your child had fluoride varnish painted on their teeth today | Parents | 81 | Gillsans MT/14 | Customised | No fold | 2 | 0 | 4.3 | 82.6 | 7 |
| 56 | OHST | G | Post op instructions | All patients | 188 | Gillsans MT/12 | A4 | No fold | 1 | 0 | 5.2 | 76.8 | 8 |
| 57 | Medicare | G | Child dental benefits schedule | Parents | 618 | Veranda/11 | A4 | Trifold | 4 | 3 | 11.1 | 46.3 | 13 |
| 58 | South Australia Dental Service | G | Sugar | All patients | 660 | Gillsans MT/11 | A4 | Trifold | 5 | 2 | 7.5 | 66.4 | 9 |
| 59 | Oral Health Promotion Clearing House | O | 11 things you must know about protecting your teeth, gums and mouth | All patients | 327 | FranklinGothic-Book/10 | A4 | Trifold | 5 | 1 | 9.8 | 56.7 | 11 |
| 60 | University of Adelaide | O | Patient information pamphlet no. 9: early childhood decay | Parents | 1105 | FranklinGothic-Book/9 | A4 | Trifold | 4 | 2 | 7.8 | 65.3 | 9 |
| 61 | University of Adelaide | O | Patient information pamphlet no. 6: beating rampant decay | Parents | 854 | FranklinGothic-Book/9 | A4 | Trifold | 3 | 2 | 7.4 | 65.4 | 9 |
| 62 | University of Adelaide | O | Patient information pamphlet no. 2: tooth erosion | All patients | 718 | FranklinGothic-Book/9 | A4 | Trifold | 3 | 1 | 8.1 | 63.3 | 10 |
| 63 | University of Adelaide | O | Patient information Pamphlet no 5.: dental sealants | All patients | 666 | Arial/9 | A4 | Trifold | 3 | 4 | 6.6 | 68.7 | 9 |
| 64 | Private family dental practice | O | Information for patients interested in orthodontic treatment at Riverside family dental | All patients | 508 | Times New Roman/12 | A4 | No fold | 0 | 1 | 9.1 | 57 | 11 |
| 65 | Private family dental practice | O | Information for parents of children having a dental treatment under general anaesthetic | Parents | 989 | Times New Roman/12 | A4 | No fold | 3 | 8.7 | 63.1 | 11 | |
| 66 | Private dental surgery | O | Home treatment after surgical dental extractions | All patients | 231 | Veranda/11 | A4 | No fold | 0 | 0 | 6 | 71.8 | 9 |
| 67 | Private dental surgery | O | Home treatment after simple dental extractions | All patients | 193 | Veranda/11 | A4 | No fold | 0 | 0 | 5.1 | 74.7 | 8 |
a ADA Australian Dental Association, ANZAOMS Australian and New Zealand Association of Oral and Maxillofacial Surgeons, OHST Oral Health Services Tasmania
b C Commercial, G Government, O Other, P Professional
Content
Table 1 shows that out of the 67 oral health brochures reviewed, 20 targeted adult patients, 21 all patients and 16 contained information about child oral health though this latter group targeted parents rather than children as the reading audience. Materials were also written for late teens and adults (6), denture holders (2), diabetic patients (1), and seniors (1).
A range of topics were represented in the brochures samples and included: preventative oral health care (9), care in response to a specific oral health condition (15), age group (13) or oral health specific to a general health status/condition (4). Seven were about oral health products and the remaining 19 focussed information on a dental appliances or procedures.
Only thirty one brochures (46 %) listed the year of publication or revision and these ranged from the years 2002 to 2014. Twenty eight brochures reported endorsement by a professional association, 14 by a government department and 20 did not list any endorsement. Thirty four brochures (51 %) provided information on how the reader could access additional information though there were only 6 brochures (5 from industry sources and 1 from a Government source) that were also available in up to 6 other languages.
Readability
The FKGL of the 67 brochures ranged from Grade 3 to 13 (post-secondary). The SMOG test was positively correlated with the FKGL (rs = 0.92, p < 0.001) though consistently rated materials 2–3 grades higher. The FRE scores ranged from 43.5 to 98.1 (the higher the FRE score, the more readable the material) and scores demonstrated a high inverse correlation with grades computed for the FKGL (rs = -0.96, p < 0.001) and the SMOG (rs = -0.90, p < 0.001).
The brochure produced by Colgate entitled “Oral Health through everyday care” had the lowest reading-grade level with a FKGL level of 3.1 and contained only1 professional jargon term (Table 1, #1). The highest reading level (12.6) required was obtained for a well-illustrated brochure “GC Tooth mousse for children” which had 13 professional jargon terms recorded (Table 1, #20).
Brochures produced by government publishers required a lower level of reading ability than those from other sources with median and mean scores for the FKGL and the SMOG being lower than those from commercial, professional and other sources (Table 2). The FKGL for government brochures (n = 14) ranged from grade 4 to 11 (mean = 5.6 ± 1.8). Reading levels for materials produced by commercial sources (n = 22) ranged from 3 to 13 (mean = 8.3 ± 2.1), those from professional colleges (n = 22) ranged from grade 7 to 11 (mean = 8.9 ± 0.9) and brochures produced by “other” sources (n = 9) ranged from 5 to 10 (mean = 7.6 ± 1.5).
Table 2.
Descriptive statistics: selected attributes (N = 67)
| Source | Commercial (n = 22) | Government (n = 14) | Professional (n = 22) | Other (n = 9) |
|---|---|---|---|---|
| Feature | ||||
| Structure and format | ||||
| Word count | ||||
| • Min-Max | 193–1759 | 81–660 | 280–3856 | 193–1105 |
| • Mean (SD) | 852 (371) | 272.5 (186.4) | 2061.4 (949.6) | 621 (329) |
| • Median | 765 | 178 | 1738 | 666 |
| Font size | ||||
| • Min-Max | 7–12 | 10–14 | 7–12 | 9–12 |
| • Mean (SD) | 9.7 (1.1) | 11.4 (0.9) | 10.8 (0.9) | 10.2 (1.3) |
| • Median | 10 | 11 | 11 | 10 |
| Pictures | ||||
| • Min-Max | 2–17 | 1–13 | 1–9 | 0–5 |
| • Mean (SD) | 7.4 (4.0) | 6.1 (4.1) | 3.2 (2.2) | 2.3 (1.8) |
| • Median | 6.5 | 6 | 2 | 3 |
| Readability | ||||
| Flesch-Kincaid Grade Level | ||||
| • Min-Max | 3.1–12.6 | 4.3–11.1 | 6.9–10.9 | 5.1–9.8 |
| • Mean (SD) | 8.3 (2.1) | 5.6 (1.8) | 8.9 (0.9) | 7.6 (1.5) |
| • Median | 8.2 | 5 | 9.1 | 7.8 |
| SMOG | ||||
| • Min-Max | 6–13 | 6–13 | 9–12 | 8–11 |
| • Mean (SD) | 10.3 (1.7) | 7.9 (1.8) | 10.6 (0.8) | 9.6 (1.1) |
| • Median | 10.5 | 7.5 | 11 | 9 |
| Flesch Reading Ease | ||||
| • Min-Max | 43.5–98.1 | 46.3–85.7 | 50.5–68.8 | 56.7–74.7 |
| • Mean (SD) | 59.8 (12.2) | 74.2 (9.9) | 58.4 (5.6) | 65.1 (6.1) |
| • Median | 58.65 | 75.8 | 56.3 | 65.3 |
| Professional jargon words | ||||
| • Range | 0–13 | 0–3 | 4–18 | 0–4 |
| • Mean (SD) | 4.3 (4.0) | 0.9 (0.9) | 9.8 (4.2) | 1.6 (1.5) |
| • Median | 3 | 1 | 9 | 1 |
There were 132 dental jargon terms identified in the 67 brochures sampled (Table 3). The number used in each ranged from 0 to 18. Ten brochures (6 from government sources) contained no professional jargon terms. Government brochures (with the exception of #57 “Child dental benefits schedule”) used fewer professional jargon terms (mean = 0.9 ± 0.9) than those produced by “other” (mean = 1.6 ± 1.5), commercial (mean = 4.3 ± 4.0) or professional associations (mean = 9.8 ± 4.2). Brochures from these latter three sources also used a greater average number of words (Table 2).
Table 3.
Professional jargon words
| Professional jargon words (n = 132) | ||||
|---|---|---|---|---|
| Abrasive | CPPACP | Haemophilia | Microscopic | Pulpotomies |
| Abscess | Craze | Halitosis | MRI | Radiograph |
| Abutment | Crossbite | Herpes simplex | Nerve canal | Recede |
| Amalgam | Cusp | Hyperplasia | Occlusal | Remineralise |
| Anticariogenic | Decalcification | Hypersensitivity | Occlusion | Resin |
| Apicoetomy | Deciduous teeth | Impacted | Onlays | Resorption |
| Arch wire | Demineralise | Incision | Open bite | Retrognathic |
| Arthrocentesis | Denting | Incisors | Ophthalmic | Rheumatoid arthritis |
| Arthroscopy | Dentition | Inferior alveolar nerve | Orofacial | Root planning |
| Arthrotomy | Desensitising | Inlays | Orthodontics | Septicaemia |
| Atherosclerotic cardiovascular disease | Disc | Interdental | Orthodontist | Splints |
| Bio-available | Disclosing tablets | Intravenous fluids | Orthognathic | Strontium chloride |
| Biofeedback | Dissipate | Keloid | Osteoarthritis | Temporalis muscle |
| Bonding | Dormant | Lateral pterygoid muscle | Osteonecrosis | Temporomandibular joint |
| Bone graft | Dry socket | Lavage | Osteoporosis | Tooth crown |
| Bridge | Endocarditis | Leukoplakia | Paget’s disease | Tooth mousse |
| Bruxism | Endodontic | Lingual nerve | Periodontal | Tricalcium |
| Buropion | Erosion | Lustre | Periodontal ligament | Triclosan |
| Calculus | Expectorate | Malocclusion | Periodontitis | Trigeminal nerve |
| Canines | Fissure sealants | Mandible | Pharynx | Tubules |
| Caries | Fissures | Mandibular | Phosphate | Velopharyngeal |
| Cementum | Fluoroapatite | Masseter muscle | Post operative | Velum |
| Composite | Fluorosis | Maxilla | Potassium | Veneers |
| Condyle | Foramen | Maxillofacial | Prognathic | Xerostomia |
| Conjunctional tissue | Fossa | Melanosis | Propagating | |
| Connective tissue | Gingivitis | Mental Foramen | Prosthodontist | |
| Copolymer | Glass ionomer cements | Mental nerve | Pulp | |
Discussion
A number of factors contribute to the readability of health education materials such as content of the message, complexity, the language used, text type and size, visual appearance, layout and understandability [21]. In this study, we focussed upon the structure and format of materials, features related to content as well as readability metrics. The format and presentation of the brochures such as font type and size, use of headings, bullets and pictures as devises to illustrate key concepts and to break up passages of text can influence how readers engage with and comprehend the information presented [4]. In the present study, consideration had clearly been given to these (and other) factors by publishers though brochures from professional and to a slightly lesser extent those produced by commercial publishers tended to use a greater number of words and demonstrated readability characteristics suited to a more literate audience.
The median and most frequent font size used in the brochures reviewed was 11 point. Out of the 67 brochures, only 10 made used of a recommended font size between 12 and 14 points [21]. Noticeably, one brochure written for older people (Table 1, #18) used a font size of 9 points and could present a challenge for those with some visual impairment even with the assistance of glasses.
The reading level of brochures sampled ranged from grade 3 to grade 13. Within the context of the U.S. assessment of grade level, it has been recommended that the reading level of patient education brochures should be no higher than sixth- to eighth-grade [22, 23]. However, about 50 % of the 67 brochures sampled in this study were written at a level above this upper limit. This suggests that the information contained in these materials may be difficult to fully comprehend by sections of the Tasmanian population where it has been estimated that less than 50 % of people are able to demonstrate the minimum level of health literacy required to function adequately in this domain (skill level 3 or above) [13].
Consistent with the previous studies [4, 5], our findings indicated that government brochures were the easiest to read though did contain some jargon words and, as reported in an Australian qualitative study [7], could therefore still be confusing to a reader. Brochures from professional associations and commercial publishers made more frequent use of professional jargon. Such differences may reflect assumptions about differences in the overall literacy level of the populations serviced by each sector with government materials (public dental services) directed to a larger proportion of clients with lower levels of literacy.
Although a wide range of assessment tools is available, no gold standard has been established to assess the readability of print-based patient education information across all settings [24]. Generally, using more than one readability assessment tool is preferred over using a single measure. This can provide some assurance of reliability and also highlight different aspects of the attribute under investigation. In this study, we chose four indictors of readability for reasons of simplicity (ease to use) and their widespread use across health discipline areas: the FKGL, FRE, SMOG and count of professional jargon words [4]. Consistent with the literature, the FKGL, FRE, SMOG were highly correlated though the reading grade results obtained from the SMOG were consistently from two to three grades higher than results obtained from the FKGL. This was because the SMOG formula is based on 100 % comprehension ability i.e. stricter criteria [24]. For example, if a brochure has SMOG readability grade of 5, it indicates that all people with grade 5 reading skills would normally be able to comprehend the brochure.
Whilst strong associations have been demonstrated between literacy level and the health status of a population [25], health education and promotion materials are only one component of a broader public health message. Dental clinics often make use of oral health information materials to inform patients and augment verbal advice provided by the dentist and members of the dental team [26]. To help maximise their effectiveness, at the readability of these materials should suit the skill level and other characteristics of the patient. Identifying attributes important to the readability of materials can help dental practitioners apply the more relevant of these to the selection or even design of materials best suited to their patient’s needs.
Whilst our selection of printed materials was limited to one state of Australia and clearly not exhaustive, we did sample a relatively large number of brochures and, as found elsewhere [4, 5] they did vary in their readability characteristics. The readability attributes we assessed were limited. For example, we did not assess the use of active and passive verbs or directly measure white space, density or “clutter” in each brochure (however, our word, picture and heading counts provide some estimate of this). As acknowledged elsewhere [5] the list of professional jargon terms identified were subjective and, given the procedure we used, is likely to be an underestimate of the number of words someone with a low reading skill level would find difficult to read and understand. A critical observation to be made of this and similar studies is to recognise that reading skill level and the readability of health information is only one component of oral health literacy. The judicious and appropriate use of health education materials can however, contribute to public health and education measures directed to improving oral health outcomes.
Conclusions
Print-based oral health materials provide important information about the maintenance of good oral health and prevention of disease. Oral health brochures are publically available for patients in both public and private dental clinics in Tasmania. However their reading characteristics differed. Government (health department) brochures were easier to read than those produced by commercial, professional and other publishers. Some brochures required a high reading grade level and may not be suitable for a wide range of patients. Readability and other characteristics of oral health education materials should be assessed to ensure their suitability for use with patients, especially those suspected of having low literacy skills. The criteria applied in this study could be used as a checklist when reviewing, selecting or developing oral health brochures.
Ethics statement
This study did not involve human subject or animals. HREC approval was therefore not required.
Acknowledgements
None
Footnotes
Competing interests
The authors declare that they have no competing interests.
Author contribution
TB, HH and AF contributed to the design of the study, the collection and analysis of data and the write up of the report. All authors have read and approved the final manuscript.
Contributor Information
Tony Barnett, Phone: 613 6324 4011, Email: Tony.barnett@utas.edu.au.
Ha Hoang, Email: Thi.Hoang@utas.edu.au.
Ashlea Furlan, Email: ashlea.furlan@ths.tas.gov.au.
References
- 1.Amini H, Casamassimo PS, Lin HL, Hayes JR. Readability of the American Academy of Pediatric Dentistry patient education materials. Pediatr Dent. 2007;29(5):431–5. [PubMed] [Google Scholar]
- 2.Wilson M. Readability and patient education materials used for low-income populations. Clin Nurse Spec. 2009;23(1):33–40. doi: 10.1097/01.NUR.0000343079.50214.31. [DOI] [PubMed] [Google Scholar]
- 3.Alexander R. Readability of published dental educational materials. J Am Dent Assoc. 2000;131:937–42. doi: 10.14219/jada.archive.2000.0312. [DOI] [PubMed] [Google Scholar]
- 4.Hendrickson RL, Huebner CE, Riedy CA. Readability of pediatric health materials for preventive dental care. BMC Oral Health. 2006;6:6–14. doi: 10.1186/1472-6831-6-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Arora A, Lam AS, Karami Z, Do LG, Harris MF. How readable are Australian paediatric oral health education materials? BMC Oral Health. 2014;14(1):111. doi: 10.1186/1472-6831-14-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Arora A, Nguyen D, Do QV, Nguyen B, Hilton G, Do LG, et al. ‘What do these words mean?’: A qualitative approach to explore oral health literacy in Vietnamese immigrant mothers in Australia. Health Educ J. 2014;73(3):303–12. doi: 10.1177/0017896912471051. [DOI] [Google Scholar]
- 7.Arora A, McNAB MA, Lewis MW, Hilton G, Blinkhorn AS, Schwarz E. ‘I can’t relate it to teeth’: a qualitative approach to evaluate oral health education materials for preschool children in New South Wales, Australia. Int J Paediat Dent. 2012;22(4):302–9. doi: 10.1111/j.1365-263X.2011.01195.x. [DOI] [PubMed] [Google Scholar]
- 8.Costa SM, Martins CC, Bonfim MLC, Zina LG, Paiva SM, Pordeus IA, et al. A systematic review of socioeconomic indicators and dental caries in adults. Int J Environ Res Public Health. 2012;9(10):3540–74. doi: 10.3390/ijerph9103540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Schwendicke F, Dörfer C, Schlattmann P, Page LF, Thomson W, Paris S. Socioeconomic inequality and caries a systematic review and meta-analysis. J Dent Res. 2015;94(1):10–8. doi: 10.1177/0022034514557546. [DOI] [PubMed] [Google Scholar]
- 10.Naghibi Sistani MM, Yazdani R, Virtanen J, Pakdaman A, Murtomaa H. Determinants of oral health: does oral health literacy matter? ISRN Dentistry. Hindawi Publishing Corporation. 2013;2013:1-6. http://dx.doi.org/10.1155/2013/249591. [DOI] [PMC free article] [PubMed]
- 11.Jones K, Parker E, Jamieson L. Access, literacy and behavioural correlates of poor self-rated oral health amongst an indigenous South Australian population. Community Dent Health. 2014;31(3):167–71. [PubMed] [Google Scholar]
- 12.Baur C, Comings J, Evans C, Garcia R, Horowitz A, Ismail A, et al. The invisible barrier: literacy and its relationship with oral health. J Public Health Dent. 2005;65(3):174–82. doi: 10.1111/j.1752-7325.2005.tb02808.x. [DOI] [PubMed] [Google Scholar]
- 13.Australian Bureau of Statistics . Adult literacy and life skills survey, Summary results. 422 8.0. 2006 (Re issue) Canberra: Australian Bureau of Statistics; 2008. [Google Scholar]
- 14.National Advisory Council on Dental Health. Report of the National Advisory Council on Dental Health Canberra: National Advisory Council on Dental Health (NACDH); 2012. Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/final-report-of-national-advisory-council-on-dental-health.htm . Accessed 5 May 2014.
- 15.Online OCR. Convert scanned Pdf to Word: Online OCR; 2014. Available from: http://www.onlineocr.net/ . Accessed 15 May 2014.
- 16.Lewis M, Newton J. An evaluation of the quality of commercially produced patient information leaflets. Br Dent J. 2006;201(2):114–7. doi: 10.1038/sj.bdj.4813846. [DOI] [PubMed] [Google Scholar]
- 17.Kincaid JP, Fishburne RP, Jr, Rogers RL, Chissom BS. Derivation of new readability formulas (automated readability index, fog count and flesch reading ease formula) for navy enlisted personnel. Springfield: US Department of Commerce; 1975. [Google Scholar]
- 18.Flesch R. A new readability yardstick. J Appl Psychol. 1948;32(3):221. doi: 10.1037/h0057532. [DOI] [PubMed] [Google Scholar]
- 19.McLaughlin GH. SMOG grading: A new readability formula. J Reading. 1969;12(8):639–46. [Google Scholar]
- 20.The University of Nottingham. How to use the SMOG calculator: The University of Nottingham; no year. Available from: http://www.niace.org.uk/misc/SMOG-calculator/smogcalc.php#userguide . Accessed 15 June 2014.
- 21.Centers For Disease Control Prevention . Simply put: A guide for creating easy-to-understand materials. Atlanta: Georgia Strategic and Proactive Communication Branch; 2009. [Google Scholar]
- 22.Kindig DA, Panzer AM, Nielsen-Bohlman L. Health Literacy: A Prescription to End Confusion. Washington: National Academies Press; 2004. [PubMed] [Google Scholar]
- 23.Weiss BD, Blanchard JS, McGee DL, Hart G, Warren B, Burgoon M, et al. Illiteracy among Medicaid recipients and its relationship to health care costs. J Health Care Poor Underserved. 1994;5(2):99–111. doi: 10.1353/hpu.2010.0272. [DOI] [PubMed] [Google Scholar]
- 24.Badarudeen S, Sabharwal S. Assessing readability of patient education materials: current role in orthopaedics. Clin Orthop Relat Res. 2010;468(10):2572–80. doi: 10.1007/s11999-010-1380-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92(8):1278–83. doi: 10.2105/AJPH.92.8.1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Albright J, de Guzman C, Acebo P, Paiva D, Faulkner M, Swanson J. Readability of patient education materials: implications for clinical practice. Appl Nurs Res. 1996;9(3):139–43. doi: 10.1016/S0897-1897(96)80254-0. [DOI] [PubMed] [Google Scholar]