

Abstract
To report two cases of bilateral conjunctival granuloma with histopathological features of the Splendore-Hoeppli phenomenon and review of the literature. Two female patients, one with a history of pulmonary eosinophilic infiltration and another with a history of vernal keratoconjunctivitis, presented with bilateral cream to yellow colored nodules in the superior bulbar conjunctiva. Histopathologic examination revealed characteristic features of the Splendore-Hoeppli phenomenon manifesting as zones of amorphous eosinophilic material surrounded by aggregations of epithelioid histiocytes, giant cells, eosinophils and lymphoplasmacytic infiltrates. No evidence of infectious organisms was found. Our report adds to non-infectious cases of conjunctival Splendore-Hoeppli phenomenon. Previous history of allergic disorders may have contributed to the occurrence of this entity.
Keywords: Conjunctival Granuloma, Pulmonary Eosinophilic Infiltration, Splendore-Hoeppli, Vernal Keratoconjunctivitis
INTRODUCTION
Allergic conjunctival granulomas (ACG), described by Ashton and Cook (1979), are benign, noninfectious zonal type granulomatous inflammations exhibiting the Splendore-Hoeppli phenomenon (SHP). This phenomenon is characterized by amorphous eosinophilic material surrounded by epithelioid histiocytes, multinucleated giant cells, lymphocytes, eosinophils and plasma cells. Sometimes Charcot-Leyden crystals are also noted.[1,2,3,4,5,6]
SHP was first described around fungus spores by Splendore in 1908 and then surrounding Schistosoma eggs by Hoeppli in 1932.[7] This phenomenon can be seen in infectious and noninfectious processes. Herein, we report two patients with allergic conjunctival granulomas presenting the SHP.
CASE REPORTS
Case 1
A 27-year-old woman presented with foreign body sensation and itching in both eyes for 3 weeks. She had history of hypereosinophilia and a biopsy-proven pulmonary eosinophilic infiltration, for which she was on a tapering dose of oral prednisolone. She had also received topical steroids with no improvement. Slit lamp examination disclosed multiple non-tender and white-centered cream to yellow colored nodules at the superior bulbar conjunctiva [Figure 1a]. Incisional biopsy of the lesion in the right eye was performed and histopathologic examinations revealed stratified conjunctival squamous epithelium overlying a zonal granulomatous inflammation composed of scattered amorphous eosinophilic materials surrounded by aggregates of epithelioid histiocytes, multinucleated giant cells, lymphocytes, plasma cells and numerous eosinophils [Figure 1b-d]. No microorganisms were found with Brown and Brenn, PAS, and Ziehl-Neelsen stains. The clinical and histopathologic features were consistent with allergic conjunctival granuloma.
Figure 1.
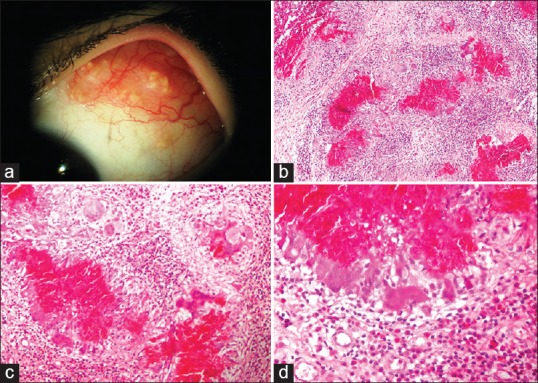
(a) Slit lamp photograph depicts multiple white-centered cream to yellow colored nodules on the superior bulbar conjunctiva. (b) Scattered eosinophilic materials containing nuclear debris which are surrounded with epithelioid histiocytes, giant cells and lymphocytes demonstrating “zonal granulomatous inflammation”. Eosinophils and plasma cells are diffusely infiltrated in the conjunctival stroma (hematoxylin and eosin, magnification × 100). (c and d) Higher magnification images. Note multinucleated giant cells and scattered infiltration of eosinophils in the conjunctival stroma [hematoxylin and eosin, magnification × 200 (c) and × 400 (d)].
Case 2
This patient was a 31-year-old female and a known case of vernal keratoconjunctivitis (VKC) who presented with chronic redness and itching in both eyes. Slit lamp biomicroscopy, similar to the first case, disclosed multiple lesions on the upper bulbar conjunctiva. Incisional biopsy of the right-sided lesion revealed a subepithelial fibrovascular tissue displaying a typical Splendore-Hoeppli phenomenon as described in patient 1 and was suggestive of an allergic conjunctival granuloma [Figure 2].
Figure 2.
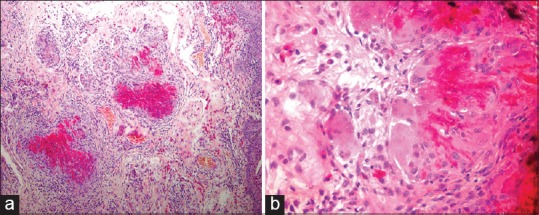
Microphotographs of case 2 demonstrating the same histopathologic findings as in case 1. Note the characteristic scattered foci of granulomatous inflammation around eosinophilic material and intrastromal infiltration of eosinophils [(hematoxylin and eosin, magnification × 100 (a) and × 400 (b)].
DISCUSSION
Splendore-Hoeppli phenomenon (SHP) can be induced by infectious and non-infectious etiologies. Infections such as bacteria, fungi and parasites, and noninfectious conditions such as allergic conjunctival granuloma (ACG) and hypereosinophilic syndromes or foreign bodies can induce SHP.[2,3,5] Out of 22 cases reported by Ashton and Cook, no microorganism was found in 18 cases, and the histopathologic features were in favor of a noninfectious form of SHP known as ACG.[1] Transmission electron microscopy of the amorphous eosinophilic substance suggested the possibility of an antigen-antibody complex and the role of immune mechanisms.[2,5]
The patients reported herein had clinical and histopathological features of ACG, and interestingly both cases had a background of allergic disorders. In a case report by Nigel et al,[2] the past history of severe asthma was remarkable. We speculate that previous history of allergic conditions such as peripheral eosinophilia, asthma, VKC, and pulmonary eosinophilia may have contributed to the pathogenesis of ACG.
Since spontaneous resolution of the lesions occurs frequently,[2,3,5,6] no treatment is usually required; however, in refractory cases in which lesions may persist for several months, excisional biopsy can be curative. No benefit has been reported with topical administration of corticosteroids.[2,5] Moreover, development of ACG has been reported while the patients were already on systemic steroids,[2,3,5] as evident in our first case.
In conclusion, ACG is one of the differential diagnoses in patients with bilateral superior conjunctival nodules, especially when the patients have an allergic or hypersensitivity predisposition.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
REFERENCES
- 1.Ashton N, Cook C. Allergic granulomatous nodules of the eyelid and conjunctiva. The XXXV Edward Jackson memorial lecture. Am J Ophthalmol. 1979;87:1–28. doi: 10.1016/0002-9394(79)90187-9. [DOI] [PubMed] [Google Scholar]
- 2.Pinto N, Hirst L, Whitby M. Conjunctival and episcleral Splendore-Hoeppli phenomenon. Clin Experiment Ophthalmol. 2008;36:865–867. doi: 10.1111/j.1442-9071.2009.01916.x. [DOI] [PubMed] [Google Scholar]
- 3.Raniga A, Weatherhead RG. Recurrence of the Splendore-Hoeppli phenomenon. Clin Experiment Ophthalmol. 2010;38:647–648. doi: 10.1111/j.1442-9071.2010.02317.x. [DOI] [PubMed] [Google Scholar]
- 4.Hussein MR. Mucocutaneous Splendore-Hoeppli phenomenon. J Cutan Pathol. 2008;35:979–988. doi: 10.1111/j.1600-0560.2008.01045.x. [DOI] [PubMed] [Google Scholar]
- 5.Read RW, Zhang J, Albini T, Evans M, Rao NA. Splendore-Hoeppli phenomenon in the conjunctiva: Immunohistochemical analysis. Am J Ophthalmol. 2005;140:262–266. doi: 10.1016/j.ajo.2005.03.023. [DOI] [PubMed] [Google Scholar]
- 6.Cameron ME, Greer H. Allergic conjunctival granulomas. Br J Ophthalmol. 1980;64:494–495. doi: 10.1136/bjo.64.7.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hoeppli R. Histological observations in experimental schistosomiasis. Jpn Chin Med J. 1932;46:1179–1186. [Google Scholar]