

Abstract
Sigmoid volvulus (SV) is a rare form of acute intestinal obstruction in which the sigmoid colon wraps around itself. The disease generally presents as a mechanical bowel obstruction with clinical features that are not pathognomonic. Similarly, X-ray films are not diagnostic in most cases. It is difficult to establish the correct preoperative diagnosis when CT and MRI are not used.
The principal strategy in the treatment of SV in uncomplicated patients is emergency endoscopic detorsion followed by elective surgery; emergent surgery is required in patients with bowel gangrene, bowel perforation, peritonitis, or unsuccessful endoscopic treatment.
In this review, we have discussed the role of sigmoidoscopy in the diagnosis and treatment of SV. Additionally, we have retrospectively and prospectively evaluated our 49-year, 987-patient clinical experience, the largest single-center SV series ever reported.
KEY WORDS: Sigmoid colon, Volvulus, Sigmoidoscopy, Diagnosis, Treatment
INTRODUCTION
First described by von Rokitansky in 1836, sigmoid volvulus (SV) refers to the wrapping of the sigmoid colon around its own base.1-3 The incidence of SV is relatively high in South Africa, the Middle East, Northern Europe, Latin America and Australia,1,3-6 but the incidence in the United states is 1.67 per 100 000 person-years.5 SV most commonly occurs in adult men and usually presents in the 4th to 8th decades of life; the male to female ratio ranges from 1.4/1 to 4/1.1,3,7 The presence of an elongated sigmoid colon with a narrow mesentery (dolichosigmoid) is a prerequisite for SV, which is thought to be related to advanced age, male gender, high altitude, dietary or defecation habits, and some pathologies such as megacolon.1,8
SV generally presents as an acute large bowel obstruction. The most common clinical features include abdominal pain, abdominal distention, and obstipation, which are known as the classical SV triad.1,3,4,9 It may be difficult to make an accurate preoperative diagnosis of SV without using sigmoidoscopy, CT, or MRI; the diagnosis is currently made under laparotomy or on autopsy in 10-15% of patients.1-3,7,10
The principal strategy in the treatment of SV in uncomplicated patients is emergency endoscopic detorsion followed by elective surgery, while emergency surgical treatment is needed in patients with bowel gangrene, bowel perforation, peritonitis, or unsuccessful endoscopic detorsion. The mean morbidity rate of SV is 12.5%, while the mortality rate ranges from 8 to 28.3%.1,11-13
Indications and contraindications of sigmoidoscopy
Any evidence or suspicion of a large bowel obstruction, particularly SV, is one of the main indications of diagnostic and/or therapeutic sigmoidoscopy.1,3,13 Abdominal pain, abdominal distention, and obstipation (which are the symptoms of the classical SV triad) are observed on average in 93%, 89.9%, and 83% of SV patients, respectively.1-4,6,14,15 Abdominal X-ray film shows SV findings, including a sigmoid dilatation with intestinal air-fluid levels, in 57-90% of patients.1,3,10,16 CT or MR is able to accurately identify SV in 96.6% and 97.4% of patients, respectively. Signs that can help diagnose SV on CT or MR include the whirl sign in the sigmoid mesentery, sigmoid dilatation, and intestinal air-fluid levels.1,3,10,17 Contrast enema has been used to diagnose SV in the past (mostly in children) but has a 66.7-78.6% success rate and a mortality rate that ranges from 7.7-9%.2,18 Contrast enema is not advised because of the possibility of bowel perforation, peritonitis, and risk of missing bowel gangrene.1,3,13 Sigmoidoscopy helps to diagnose the bowel torsion, shows the viability of the bowel mucosa, and contributes to the bowel detorsion. Therefore, rigid or (preferably) flexible sigmoidoscopy is one of the best methods of diagnosing SV and is the preferred initial treatment of SV.1,3,13,19
One of the main contraindications to sigmoidoscopy is evidence or suspicion of bowel gangrene, bowel perforation, or peritonitis, which may clinically manifest as melanotic stool during anamnesis or rectal examination, guarding/rigidity, or rebound tenderness.1,3,13 Sigmoid gangrene develops in 6.1-30.2% of all SV cases and in 10.7-93.4% of surgically treated SV cases. Melanotic rectal stool is observed in 7.3-11.8% of SV patients, while bowel gangrene is diagnosed on average in 5.5% of patients during sigmoidoscopy, causing the need to terminate the procedure. Guarding/rigidity or rebound tenderness is found in 8.9-14.9% of SV patients.1,3,4,13,14,20,21
Sigmoidoscopy in diagnosis
Sigmoidoscopy helps establish the diagnosis of SV. The classical finding on sigmoidoscopy is a spiral sphincter-like twist of the lumen, usually 20-30 cm from the anal verge (Fig.1); additionally, the inability to insert the endoscope into the proximally twisted site helps lead to the correct diagnosis. Sigmoidoscopy allows for direct visualization of the bowel mucosa viability and may also be used in the differential diagnosis of SV by identifying the other causes of bowel obstruction, such as bowel malignancies or megacolon.1,3,5,6,10,14,19,22-25
Fig.1.
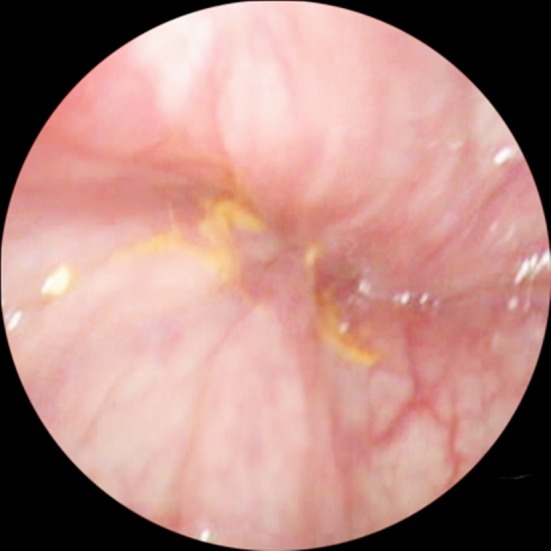
Endoscopic view of the sigmoid colon in a patient with sigmoid volvulus (spiral sphincter-like twist of the obstructed bowel lumen)
Although sigmoidoscopy is thought to have a high diagnostic value in patients with SV (with a 76-100% diagnostic success rate), there is no quantitative data available in the literature commenting on the overall diagnostic role of sigmoidoscopy.1,3,10,14,19,22-25
Sigmoidoscopy in treatment
SV requires an emergency treatment following an early and effective resuscitation.1,12,13 Endoscopic detorsion, including gentle inserting of the endoscope with rotation of the tip of the instrument towards the opposite side of the torsion direction while providing minimal air insufflation, is the initial treatment of choice in uncomplicated SV patients. A 48.1-100.0% success rate, 0.0-26.4% morbidity rate, and 0.0-19.0% of mortality rate has been reported using this technique.1-7,9,10,12-15,18,19,21-33 The results of endoscopic treatments in various series are shown in Table-I.
Table-I.
Endoscopic treatments of patients with sigmoid volvulus in different series.
| Author | Years | Patient No. | Success (%) | Morbidity (%) | Mortality (%) | Follow-up | Recurrence (%) |
|---|---|---|---|---|---|---|---|
| String and DeCosse22 | 1971 | 17 | 64.7 | 9.1 | 20.0 | ||
| Arnold and Nance2 | 1973 | 114 | 76.3 | 0.9 | 9.0 | 2 years | 55.5 |
| Ballantyne et al4 | 1985 | 31 | 83.9 | 49 months | 19.4 | ||
| Arigbabu et al26 | 1985 | 92 | 88.2 | ||||
| Bak and Boley15 | 1986 | 43 | 90.7 | 4.7 | 2.3 | ||
| Brothers et al19 | 1987 | 29 | 55.2 | 8.0 | 57.0 | ||
| Oncu et al27 | 1991 | 18 | 55.6 | 0.0 | |||
| Grossmann et al14 | 2000 | 189 | 81.5 | 69.7 | |||
| Salas et al18 | 2000 | 28 | 60.7 | ||||
| Turan et al28 | 2004 | 81 | 48.1 | 3.7 | 0.0 | 15.0 | |
| Bhuiyan et al29 | 2005 | 17 | 58.8 | 5.9 | |||
| Oren et al12 | 2007 | 562 | 78.3 | 2.5 | 0.7 | Early | 3.2 |
| Safioleas et al21 | 2007 | 33 | 78.8 | 3.0 | 14 months | 41.7 | |
| Heis et al7 | 2008 | 25 | 68.0 | 0.0 | |||
| Jangjoo et al23 | 2010 | 75 | 89.7 | ||||
| Mulas et al24 | 2010 | 24 | 70.1 | 26.4 | |||
| Tan et al25 | 2010 | 29 | 82.8 | 3.4 | |||
| Swenson et al9 | 2012 | 28 | 78.6 | 19.0 | 106 days | 47.6 | |
| Lou et al30 | 2013 | 28 | 92.9 | 0.0 | 0.0 | 26.9 | |
| Yassaie et al31 | 2013 | 31 | 100.0 | 0.0 | 31 days | 61.3 | |
| Atamanalp13 | 2013 | 673 | 77.3 | 2.1 | 0.6 | Early | 4.4 |
| Maddah et al32 | 2014 | 80 | 100.0 | 12.9 | |||
| Sugimoto et al33 | 2014 | 71 | 100.0 | 0.0 | 0.0 | 200 days | 55.6 |
During endoscopic detorsion, a variety of anesthetics or sedatives may be used.1,3,13 In detorsioned cases, a rectal tube may be placed in the sigmoid colon to prevent an early recurrence; it is withdrawn following a radiograph, which is obtained a few hours later.1,3,12,13,23-25,27,31,32 The use of flexible endoscopes instead of rigid endoscopes may increase the success rate and decrease the complication and mortality rates; overall, flexible endoscopes are better tolerated by the patients.1,3,22-26,28 Similarly, the success rate may be increased by the use of colonoscopes instead of sigmoidoscopies.1,3,13,22,23,28
The main complications of sigmoidoscopy-treated SV as well as the most common causes of sigmoidoscopy-related deaths are bowel perforation, peritonitis, shock, fluid-electrolyte imbalances, renal insufficiency, and cardiopulmonary problems.1,3,12,13,25,28 Because SV has a tendency to recur after endoscopic detorsion (3.2-69.7% of successfully detorsioned SV cases),2,4,10,12-14,19,21-23,28,30-34 elective surgery is recommended after 2-3 days in a select group of patients;1,3,12,13,23,34,35 this recommendation is particularly applicable to ASA 1-3 patients, in whom perioperative mortality is minimal.34
SIGMOIDOSCOPY IN SPECIAL SITUATIONS
Sigmoidoscopy in Childhood
SV is extremely rare in childhood, with less than 100 cases reported in the literature.1,3,13,18,32,36,37 In spite of the fulminant clinical presentation, it is difficult to obtain a preoperative accurate diagnosis.36,37 Although hydrostatic reduction via barium, water-soluble contrast, or saline was previously used during non-operative treatment, endoscopic reduction performed via pediatric endoscopes may also be used successfully in uncomplicated patients.1,18,36,37 The morbidity of SV in childhood remains high and occurs in approximately 30% of all patients; the mortality is also startling, which is observed more than 25% of patients.18,36,37
Sigmoidoscopy in the elderly
SV is common in the elderly and approximately 50% of SV patients are over 60 years old.1,5,13,15,21,38 Abnormal defecation and chronic constipation, which are features normally found in the elderly, may cloud the clinical picture. The clinical picture in these patients may therefore be less diagnostic.1,3,5,13,15,21,38 Endoscopic reduction is the first choice in the treatment of uncomplicated patients, and the avoidance of emergency surgery improves the prognosis.1,5 These elderly patientssuffer from high morbidity, which occurs in 6-24% of cases. Notably, the mortality increases to 75% after the age of 70; 50-85% of these patients have serious comorbidities.1,5,15,21,38
Sigmoidoscopy during Pregnancy
SV is relatively rare in pregnancy. As of 2014, there were fewer than 100 cases reported in the literature.1,3,13,39,40 Abdominal pain, nausea, and vomiting are normal findings in pregnancy; as such, these clinical findings are not reliable diagnostic features of SV.1,3,39,40 The management of SV in pregnancy requires a multidisciplinary approach involving general surgery, obstetrics, and neonatology.39,40 Although endoscopic detorsion was thought to be unsuccessful in most pregnant patients in the past due to an enlarged uterus as a mechanical impediment,40 gentle flexible endoscopic detorsion under careful monitoring is recommended as treatment of choice in all trimesters of pregnancy in the treatment of uncomplicated patients, but is particularly true for those women in the first and second trimesters.39 SV has a poor prognosis in pregnancy, with reported 6-60% maternal and 20-50% fetal mortality rates.1,39,40
Clinical Experience
The incidence of SV is high in Turkey, particularly in Eastern Anatolia3,13 where our university clinic is located. To the best of our knowledge, this report represents the largest single-center SV series.
A total of 987 patients with SV were treated over a 49-year period between June 1966 and June 2015 in the Department of General Surgery, Faculty of Medicine, Ataturk University. The data were collected retrospectively till 1986, and prospectively after. After resuscitation and clinical examination, abdominal X-rays were obtained for all patients (although CTs or MRIs have been obtained in several stable patients in recent years). Emergency surgery was performed in patients with acute abdominal findings, melanotic stool, and unsuccessful non-operative detorsion. Sigmoidoscopy was used in the diagnosis of several stable patients but has been used in the treatment of all stable SV patients. We used rigid sigmoidoscopy in the early years but have tended to use flexible sigmoidoscopy or colonoscopy over the past 26 years. In successfully detorsioned patients, a rectal tube was inserted into the sigmoid colon and was left in place for 12-24 hours. Elective surgery was recommended in several stable patients.
Diagnostic sigmoidoscopy was used in 151 patients; the correct diagnosis was obtained in 149 of those patients (accuracy rate, 98.7%). Endoscopic misdiagnosis included colonic invagination in one patient and partial colonic volvulus in another; notably, there were colonic malignancies in both patients. Nonoperative therapeutic procedures were used in 712 patients; barium enema in 13 patients, rigid sigmoidoscopy in 351 patients, and flexible sigmoidoscopy in 348 patients. The results of these procedures are shown in table 2. When the patients with bowel gangrene are excluded, the therapeutic success rate of then on operative procedures is 82.1%, with a highest success rate in the flexible sigmoidoscopy group (82.9%). In the nonoperatively treated group, 5 patients (0.7%) died: 3 died from toxic shock and two died from peritonitis; the lowest mortality rate was in the flexible sigmoidoscopy group (0.3%). Complications were observed in 17 of the nonoperatively treated patients (2.4%). These complications included renal insufficiency in 13 patients, myocardial infarction in two patients, and peritonitis in 2 patients, with the lowest morbidity rate in the flexible sigmoidoscopy group (1.4%). Early recurrence was observed in 26 patients (4.7%) with the lowest early recurrence rate in the rigid sigmoidoscopy group (3.3%).
Table-II.
Non-operative procedures in patients with sigmoid volvulus and their respective results.
| Barium enema | Rigid sigmoidoscopy | Flexible sigmoidoscopy | Total | |
|---|---|---|---|---|
| Total | 13(1.8%) | 351(49.3%) | 348(48.9%) | 712 |
| Success | 9(69.2%) | 274(78.1%) | 266(76.4%) | 549(77.1%) |
| Failure | 4(30.8%) | 61(17.4%) | 55(15.8%) | 120(16.9%) |
| Bowel gangrene | 0(0.0%) | 16(4.6%) | 27(7.8%) | 43(6.0%) |
| Success except gangrenous cases | 9/13(69.2%) | 274/335(81.8%) | 266/321(82.9%) | 549/669(82.1%) |
| Mortality | 1(7.7%) | 3(0.9%) | 1(0.3%) | 5(0.7%) |
| Morbidity | 3(23.1%) | 9(2.6%) | 5(1.4%) | 17(2.4%) |
| Earlyr ecurrence (in the hospitalization period) | 1(11.1%) | 9(3.3%) | 16(6.0%) | 26(4.7%) |
DISCUSSION
As regards the diagnosis of SV, clinical features are not pathognomonic, and abdominal X-ray films are usually not helpful. However, CT and MR are almost always diagnostic. Rigid or (preferably) flexible sigmoidoscopy helps to the diagnosis of SV by direct visualization of the obstructive bowel lumen. Additionally, sigmoidoscopy may demonstrate the viability of the bowel mucosa and identify other potential causes of bowel obstruction.
Spontaneous detorsion of SV is not common and therefore requires emergency treatment. Rigid or (preferably) flexible endoscopic detorsion is the initial treatment of choice in SV in the absence of bowel gangrene, bowel perforation, or peritonitis. Hydrostatic reduction has historical value, and endoscopic detorsion via pediatric endoscopes is the preferable treatment method in children. Endoscopic reduction is the treatment of choice in the elderly, improving the overall prognosis by avoiding emergent surgery. Endoscopic detorsion via monitorization is also the first choice in pregnancy, particularly in the first and second trimesters.
There is minimal morbidity and mortality from flexible sigmoidoscopy-treated SV. Because SV has a tendency to recur and because each subsequent SV episode has different morbidity and mortality, elective surgery is recommended in a select group of patients.
Footnotes
Declaration of Interest: None.
Grant Support & Financial Disclosure: None
Authors’ contribution
SSA designed the study, collected and analysed the data, reviewed the literature and wrote the manuscript.
RSA reviewed the literature and controlled the text.
REFERENCES
- 1.Raveenthiran V, Madiba TE, Atamanalp SS, De U. Volvulus of the sigmoid colon. Colorectal Dis. 2010;12(7):e1–e17. doi: 10.1111/j.1463-1318.2010.02262.x. doi:10.1111/j.1463-1318.2010.02262.x. [DOI] [PubMed] [Google Scholar]
- 2.Arnold GJ, Nance FC. Volvulus of the sigmoid colon. Ann Surg. 1973;177(5):527–537. doi: 10.1097/00000658-197305000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Atamanalp SS. Sigmoid volvulus: Diagnosis in 938 patients over 45.5 years. Tech Coloproctol. 2013;17(4):419–424. doi: 10.1007/s10151-012-0953-z. doi:10.1007/s10151-012-0953-z. [DOI] [PubMed] [Google Scholar]
- 4.Ballantyne GH, Brandner MD, Beart RW, Ilstrup DM. Volvulus of thecolon. Ann Surg. 1985;202(1):83–92. doi: 10.1097/00000658-198507000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Atamanalp SS, Ozturk G. Sigmoid volvulus in theelderly: Outcomes of a 43-year, 453-patient experience. SurgToday. 2011;41(4):514–519. doi: 10.1007/s00595-010-4317-x. doi:10.1007/s00595-010-4317-x. [DOI] [PubMed] [Google Scholar]
- 6.Lal SK, Morgenstern R, Vinjirayer EP, Matin A. Sigmoid volvulus an update. Gastrointest Sigmoidoscopy Clin N Am. 2006;16(1):175–187. doi: 10.1016/j.giec.2006.01.010. doi:10.1016/j.giec.2006.01.010. [DOI] [PubMed] [Google Scholar]
- 7.Heis HA, Bani-Hani KE, Rabadi DK, Elheis MA, Bani-Hani BK, Mazahreh TS, et al. Sigmoid volvulus in the Middle East. World J Surg. 2008;32(3):459–464. doi: 10.1007/s00268-007-9353-3. doi:10.1007/s00268-007-9353-3. [DOI] [PubMed] [Google Scholar]
- 8.Atamanalp SS, Ozturk G, Aydinli B, Oren D. Therelationship of theanatomicaldimensions of the sigmoid colonwith sigmoid volvulus. Turk J Med Sci. 2011;41(3):377–382. doi:10.3906/sag-1011-3. [Google Scholar]
- 9.Swenson BR, Kwaan MR, Burkart NE, Wang Y, Madoff RD, Rothenberger DA, et al. Colonicvolvulus: Presentation and management in Metropolitan Minnesota, Unites States. Dis Colon Rectum. 2012;55(4):444–449. doi: 10.1097/DCR.0b013e3182404b3d. doi:10.1097/DCR.0b013e3182404b3d. [DOI] [PubMed] [Google Scholar]
- 10.Atamanalp SS, Kantarci A, Ozogul B, Kisaoglu A, Atamanalp RS. The role of CT and MRI in thediagnosis of sigmoid volvulus. Turk J Med Sci. 2014;44(2):352. doi:10.3906/sag-1307-147. [PubMed] [Google Scholar]
- 11.Madiba TE, Thomson SR. The management of sigmoid volvulus. J R Coll Surg Edinb. 2000;45(1):74–80. [PubMed] [Google Scholar]
- 12.Oren D, Atamanalp SS, Aydinli B, Yildirgan MI, Basoglu M, Polat KY, et al. An algorithm for the management of sigmoid colon volvulus and the safety of primary Resection: Experience with 827 cases. Dis Colon Rectum. 2007;50(4):489–497. doi: 10.1007/s10350-006-0821-x. doi:10.1007/s10350-006-0821-x. [DOI] [PubMed] [Google Scholar]
- 13.Atamanalp SS. Treatment of sigmoid volvulus: a single-center experience of 952 patients over 46.5 years. Tech Coloproctol. 2013;17(5):561–569. doi: 10.1007/s10151-013-1019-6. doi:10.1007/s10151-013-1019-6. [DOI] [PubMed] [Google Scholar]
- 14.Grossmann EM, Longo WE, Stratton MD, Virgo KS, Johnson FE. Sigmoid volvulus in department of Veterans Affairs medical centers. Dis Colon Rectum. 2000;43(3):414–418. doi: 10.1007/BF02258311. [DOI] [PubMed] [Google Scholar]
- 15.Bak MP, Boley SJ. Sigmoid volvulus in the elderly. Am J Surg. 1986;151(1):71–75. doi: 10.1016/0002-9610(86)90014-0. [DOI] [PubMed] [Google Scholar]
- 16.Wai CT, Lau G, Khor CJL. Clinics in diagnostic imaging: Sigmoid volvulus causing intestinal obstruction, with successful endoscopicde compression. Singapore Med J. 2005;46(9):483–487. [PubMed] [Google Scholar]
- 17.Levsky JM, Den EI, DuBrow RA, Wolf EL, Rozenblit AM. CT findings of sigmoid volvulus. AJR. 2010;194(1):136–143. doi: 10.2214/AJR.09.2580. doi:10.2214/AJR.09.2580. [DOI] [PubMed] [Google Scholar]
- 18.Salas S, Angel CA, Salas N, Murillo C, Swischuk L. Sigmoid volvulus in children and adolescents. J Am Coll Surg. 2000;190(6):717–723. doi: 10.1016/s1072-7515(00)00270-2. [DOI] [PubMed] [Google Scholar]
- 19.Brothers TE, Strodel WE, Eckhauser FE. Sigmoidoscopy in colonic volvulus. Ann Surg. 1987;206(1):1–4. doi: 10.1097/00000658-198707000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Atamanalp SS, Kisaoglu A, Ozogul B. Factorsaffectingbowelgangrenedevelopment in patientswith sigmoid volvulus. Ann Saudi Med. 2013;33(2):144–148. doi: 10.5144/0256-4947.2013.144. doi:10.5144/0256-4947.2013.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Safioleas M, Chatziconstantinou C, Felekouras E, Stamatakos M, Papaconstantinou I, Smirnis A, et al. Clinicalconsiderationsandtherapeuticstrategy for sigmoid volvulus in theelderly: A study of 33 cases. World J Gastroenterol. 2007;13(6):921–924. doi: 10.3748/wjg.v13.i6.921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.String ST, DeCosse JJ. Sigmoid volvulus. An examination of themortality. Am J Surg. 1971;121(3):293–297. doi: 10.1016/0002-9610(71)90207-8. [DOI] [PubMed] [Google Scholar]
- 23.Jangjoo A, Soltani E, Fazelifar S, Saremi E, Aghaei MA. Proper management of sigmoid colonvolvulus: our experience with 75 cases. Int J Colorectal Dis. 2010;25(3):407–409. doi: 10.1007/s00384-009-0792-1. doi:10.1007/s00384-009-0792-1. [DOI] [PubMed] [Google Scholar]
- 24.Mulas C, Bruna M, Garcia-Armengol J, Roig JV. Management of colonic volvulus. Experience in 75 patients. Rev Esp Enferm Dig. 2010;102:239–248. doi: 10.4321/s1130-01082010000400004. [DOI] [PubMed] [Google Scholar]
- 25.Tan KK, Chong CS, Sim R. Management of acute sigmoid volvulus: an institution'sexperienceover 9 years. World J Surg. 2010;34(8):1943–1948. doi: 10.1007/s00268-010-0563-8. doi:10.1007/s00268-010-0563-8. [DOI] [PubMed] [Google Scholar]
- 26.Arigbabu AO, Badejo OA, Akinola DO. Colonoscopy in the emergency treatment of colonic volvulus in Nigeria. Dis Colon Rectum. 1985;28(11):795–798. doi: 10.1007/BF02555478. doi:10.1007/BF02555478. [DOI] [PubMed] [Google Scholar]
- 27.Oncu M, Piskin B, Calik A, Yandi M, Alhan E. Volvulus of the sigmoid colon. South Afr J Surg. 1991;29(2):48–49. [PubMed] [Google Scholar]
- 28.Turan M, Sen M, Karadayi K, Koyuncu A, Topcu O, Yildirir C, et al. Our sigmoid colonvolvulusexperiencesandbenefits of colonoscope in Detorsion process. Rev Esp Enferm Dig. 2004;96(1):32–35. doi: 10.4321/s1130-01082004000100005. [DOI] [PubMed] [Google Scholar]
- 29.Bhuiyan MM, Machowski ZA, Linyama BS, Modiba MC. Management of sigmoid volvulus in Polokwane-MankwengHospital. S Afr J Surg. 2005;43(1):17–19. [PubMed] [Google Scholar]
- 30.Lou Z, Yu ED, Zhang W, Meng RG, Hao LQ, Fu GC. Appropriate treatment of acute sigmoid volvulus in the emergency setting. World J Gastroenterol. 2013;19(30):4979–4983. doi: 10.3748/wjg.v19.i30.4979. doi:10.3748/wjg.v19.i30.4979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yassaie O, Thompson-Fawcett M, Rossaak J. Management of sigmoid volvulus: is earlysurgeryjustifiable?ANZ J Surg. 2013;83(1-2):74–78. doi: 10.1111/j.1445-2197.2012.06182.x. doi:10.1111/j.1445-2197.2012.06182.x. [DOI] [PubMed] [Google Scholar]
- 32.Maddah G, Kazemzadeh GH, Abdollahi A, Bahar MM, Tavassoli A, Shabahang H. Management of sigmoid volvulus: options and prognosis. J Coll Physicians Surg Pak. 2014;24(1):13–17. doi:01.2014/JCPSP.1317. [PubMed] [Google Scholar]
- 33.Sugimoto S, Hosoe N, Mizukami T, Tsunoda Y, Ito T, Imamura S, et al. Effectiveness and clinical results of endoscopic management of sigmoid volvulus using unsedated water-immersion colonoscopy. Dig Endosc. 2014;26(4):564–568. doi: 10.1111/den.12235. doi:10.1111/den.12235. [DOI] [PubMed] [Google Scholar]
- 34.Atamanalp SS, Oren D, Aydinli B, Ozturk G, Polat KY, Basoglu M, et al. Elective treatment of detorsioned sigmoid volvulus. Turk J Med Sci. 2008;38(3):227–234. [Google Scholar]
- 35.Tsai MS, Lin MT, Chang KJ, Wang SM, Lee PH. Optimal interval from decompression to semi-elective operation in sigmoid volvulus. Hepatogastroenterology. 2006;53(69):354–356. [PubMed] [Google Scholar]
- 36.Atamanalp SS, Yildirgan MI, Basoglu M, Kantarci M, Yilmaz I. Sigmoid colonvolvulus in children. Pediatr Surg Int. 2004;20(7):492–495. doi: 10.1007/s00383-004-1222-7. [DOI] [PubMed] [Google Scholar]
- 37.Smith SD, Golladay ES, Wagner C, Seibert JJ. Sigmoid volvulus in childhood. South Med J. 1990;83(7):778–781. doi: 10.1097/00007611-199007000-00015. [DOI] [PubMed] [Google Scholar]
- 38.Avots-Avotins KV, Waugh DE. Colonvolvulusandthegeriatricpatient. Surg Clin North Am. 1982;62(2):249–260. doi: 10.1016/s0039-6109(16)42684-8. [DOI] [PubMed] [Google Scholar]
- 39.Atamanalp SS, Ozturk G. Sigmoid volvulus in pregnancy. Turk J Med Sci. 2012;42(1):9–15. [Google Scholar]
- 40.Aftab Z, Toro A, Abdelaal A, Dasovky M, Gehani S, Mola AA, et al. Endoscopicreduction of a volvulus of the sigmoid colon in pregnancy: Casereportand a comprehensive review of the literature. World J Emerg Surg. 2014;9(1):41. doi: 10.1186/1749-7922-9-41. doi:10.1186/1749-7922-9-41. [DOI] [PMC free article] [PubMed] [Google Scholar]