

Abstract
Access to Recovery (ATR) is a SAMHSA-funded initiative that offers a mix of clinical and supportive services for substance abuse. ATR clients choose which services will help to overcome barriers in their road to recovery, and a recovery consultant provides vouchers and helps link the client to these community resources. One of ATR's goals was to provide services to those involved in the criminal justice system in the hopes that addressing substance abuse issues could reduce subsequent criminal behaviors. This study examines this goal by looking at recidivism among a sample of clients in one state's ATR program who returned to the community after incarceration. Results suggest there were few differential effects of service selections on subsequent recidivism. However, there are significant differences in recidivism rates among the agencies that provided ATR services. Agencies with more resources and a focus on prisoner reentry had better recidivism outcomes than those that focus only on substance abuse services.
Keywords: substance abuse, former inmates, recidivism, recovery, holistic approach
Introduction
During the past three decades, there have been dramatic increases in the U.S. prison population. At the end of 2012, there were approximately 2.3 million incarcerated adults—a more than 300% increase since the 1980s—making the prison population in the United States the largest in the world (Carson & Sabol, 2012; Minton, 2012). Much of this mass expansion has been fueled by increases in the arrest, prosecution, and incarceration of drug-related offenses. Since the 1980s, the number of drug offenders in state and federal prisons has increased more than ten-fold (Clear & Frost, 2014).
Almost all inmates will eventually be released and are expected to reintegrate back into the community (Langan & Levin, 2002; Petersilia, 2005), and many of these returning inmates have a substance abuse problem. Over half of all inmates meet criteria for drug dependence, with rates four times higher among males and nine times higher among females in comparison to the general population (Carson & Sabol, 2012; Mumola & Karberg, 2006). Previous research has demonstrated that over half of all inmates are under the influence of drugs or alcohol at the time of their arrest (Karberg & James, 2002), while nearly three quarters have reported using drugs regularly prior to incarceration (Petersilia, 2005). Despite this disproportionate rate, evidence suggests few inmates will receive intensive substance abuse treatment while incarcerated (Mitchell, Wilson, & MacKenzie, 2007; Mumola & Karberg, 2006; Prendergast, 2009; Taxman, Perdoni, & Harrison, 2007). Drug-involved offenders are twice as likely to recidivate, suggesting that many returning inmates may be rearrested because of their inability to refrain from substance abuse (Blumstein & Beck, 2005; Karberg & James, 2002; Prendergast, 2009; Warner & Kramer, 2009).
Community-based drug treatment programs have developed as a potential intervention for adult offenders (Chanhatasilpa, MacKenzie, & Hickman, 2000). Here, treatment is offered and initiated post-release while offenders are reintegrating into the community. While these programs vary widely in their approach, a growing body of research has emerged to examine their effectiveness in reducing recidivism (see Bahr, Masters, & Taylor, 2012; Boyum, Caulkins, & Kleinman, 2011; Grommon, Davidson, & Bynum, 2013; Zhang, Roberts, & Callanan, 2006). The present study examines the Indiana Access to Recovery (ATR) program. ATR is a community-based SAMHSA initiative that offers a holistic approach to substance abuse recovery through a mix of clinical and supportive services. The program works with clients to identify their personal recovery goals, which are supported by services that clients choose and pay for using voucher funds provided to them. It is this combination of increased access to recovery support services, the accumulation of recovery capital (Cloud & Granfield, 2008; Granfield & Cloud, 2001), and individual choice that can facilitate pathways out of substance use and reduce subsequent criminal activity (SAMHSA, 2006). This is a less paternalistic approach than many programs that require clients to meet predetermined goals, which may not be relevant to their individual situations.
Although one of the target populations of the ATR program specified in the national initiative was formerly incarcerated individuals, very little research has examined outcomes for such ATR clients. We use a sample of previously incarcerated ATR clients to assess the association between ATR and recidivism. More specifically we look at the types of ATR services the client received, and the agency where the client received these services. Therefore, we ask whether it is the ATR services one receives or the agency delivering them that affects subsequent recidivism.
Substance Abuse Treatment for Offenders
Substance abuse treatment has the potential to produce beneficial outcomes for offenders under correctional supervision (Chandler, Fletcher, & Volkow, 2009; Lurigio, 2000; Taxman, Perdoni, & Caudy, 2013). Much of the evidence supporting the effectiveness of substance abuse treatment for offenders emanates from evaluations of prison-based therapeutic communities with aftercare upon release (Bahr, et al., 2012). A key element of these interventions is service continuity; efforts must be made to link participation in prison-based treatment to similar community-based programs. Unfortunately, given available correctional resources very few offenders have been able to access and participate in therapeutic communities while incarcerated. Generally, less than 10% of offenders are able to access any form of substance abuse treatment services in prison (Taxman, et al., 2007).
The movement from structured prison environment to unstructured life in the community can pose additional challenges for accessing substance abuse treatment services. Fewer community-based services are available relative to those offered in prison (Chandler, et al., 2009; Lurigio, 2000). Those services that are available are not uniformly distributed; some communities possess denser concentrations of services (Visher & Travis, 2003) that vary with regard to their adherence to evidence-based principles of service delivery and network connectedness to other agencies (Friedmann, Taxman, & Henderson, 2007). As such, less than 8% of offenders are able to access and receive community-based substance abuse treatment (Taxman, et al., 2013).
Furthermore, gaps in substance abuse service participation might be directly or indirectly affected by the need or desire to access other important resources. For instance, research has suggested that a lack of stable housing can reduce substance abuse treatment participation and ultimately increase drug use and recidivism (Grommon, 2013). In a recent study of a Missouri program that provided direct monetary assistance to 122 recently released offenders, members of the sample primarily allocated funds to food, transportation, clothing, and housing or housing utilities (Morani, Wikoff, Linhorst, & Bratton, 2011), which demonstrates the significant need for basic necessities among this population. Lack of these necessities has been demonstrated to act as a barrier to engagement in substance abuse services (Laudet, Stanick, & Sands, 2009).
Local community correctional agencies and service providers have been tasked with the responsibility of initiating—or in some instances, continuing—substance abuse treatment services. One of the main contributions of contemporary prisoner reentry literature is the ability to form community partnerships to integrate and enhance access to services. For instance, an evaluation of the Serious and Violent Offender Initiative indicated that incentives to develop coordinated reentry strategies can increase exposure to an assortment of available community services including substance abuse treatment (Winterfield, Lattimore, Steffey, Brumbaugh, & Lindquist, 2009). These efforts have translated to beneficial short-term housing, employment, and substance use outcomes, but may not be an effective means to reduce recidivism (Lattimore, Steffey, & Visher, 2009).
As a standalone intervention, community-based substance abuse treatment can reduce substance use and criminality (Aos, Miller, & Drake, 2006; Chandler et al., 2009). While service delivery mechanisms can vary, treatment interventions commonly involve active case management components that seek to improve participant access to local resources while receiving treatment services. Case managers work with offenders to assess strengths and weaknesses, develop individualized plans, and coordinate services within networks of providers. Within this framework substance abuse treatment is viewed as one factor among an assortment of additional needs including but not limited to housing, employment, education, and health.
Evidence of the effectiveness of this type of approach on relapse and recidivism outcomes is underdeveloped relative to the frequency with which it is used and mixed. In a meta-analysis of 15 outpatient treatment programs with rigorous research designs, Chanhatasilpa et al. (2000) found case management approaches with active referral and management elements to be largely ineffective for offenders with substance dependencies. Similar non-significant findings were observed from a 2006 meta-analysis of 12 available research studies (Aos, et al., 2006) and various evaluations (Grommon, et al., 2013; Longshore, Turner, & Fain, 2005; Martin & Inciardi, 1997). Support for case management is found in the multisite evaluation of Treatment Alternatives to Street Crime programs (Anglin, Longshore, & Turner, 1999). Reductions in drug use among participants relative to experimental and quasi-experimental comparison groups were observed, but only two of five sites achieved decreases in recidivism.
One issue influencing the effects of case managed community-based substance abuse treatment for offenders relates to the nature of participant choice. In many instances, offenders are mandated to attend referrals to substance abuse treatment and/or participate in treatment as a condition of community supervision. While the available research suggests that offenders in mandated substance abuse treatment achieve similar, if not better, programmatic and recidivism outcomes than voluntary participants (Farabee et al., 1999; Zhang, Roberts, & Lansing, 2013), very little information is available on the outcomes of those who voluntarily self-select into treatment services. Offenders who voluntarily choose to pursue community services above and beyond traditional referral and mandate processes of community supervision may be more motivated to maintain recovery gains.
Access to Recovery
ATR initiatives provide a useful framework to examine the effect of voluntary, client centered recovery models where services are tailored to individual needs and chosen recovery pathway (Laudet & Humphreys, 2013). A key element of the ATR program model is the recognition of active human agency. Clients are empowered to choose those ancillary wraparound services that they believe will best facilitate recovery and receive vouchers to access selected services. This dramatically differs from extant case management approaches where participants rely on case manager assessment and ongoing communication exchanges to broker access to services.
Recovery capital lies at the center of the ATR program model. Emanating from social capital theoretical perspectives (Bourdieu, 1985; Coleman, 1988), recovery capital is the personal and social resources that can be collected or deployed to aid efforts to begin and sustain pathways out of substance use and abuse (Cloud & Granfield, 2008; Granfield & Cloud, 2001). Social capital, physical capital, human capital, and cultural capital have been identified as the components of recovery capital that can be drawn upon to facilitate the ends of sobriety (Cloud & Granfield, 2008; Granfield & Cloud, 2001). Although the possession of more capital is often able to contribute better outcomes than the possession of less capital, the quantity and types of resources available are highly individualized and reflective of one's immediate needs, environment, and stage of recovery (Laudet & Humphreys, 2013; Cloud & Granfield, 2008). Moreover, one's resources may actually inhibit pathways and contribute to negative recovery capital (Cloud & Granfield, 2008). This is especially true for formerly incarcerated individuals as the prison experience affects the accumulation of social and cultural capital (Cloud & Granfield, 2008).
In recognition of unequal and highly differential access to recovery capital, ATR seeks to increase recovery capital and access to recovery support services. ATR serves to provide a wide network of resources and benefits to participants (social capital), economic and tangible resources (physical capital), as well as knowledge, empowerment, and independent choice (human and cultural capital). ATR also serves an important bridging capital function by connecting individuals to material resources that may not be otherwise obtained on one's own such as treatment, peer recovery support, housing, or transportation (Lyons & Lurigio, 2010).
Research on the effect of ATR suggests significant reductions in drug use in general population samples (Buchanan, 2014; Cousins, Antonini, & Rawson, 2012; Krupski, Campbell, Joesch, Lucenko, & Roy-Byrne, 2009). Slight reductions in self-reported drug use were observed among a sample of 3,008 drug court clients who were referred to ATR programs and unmatched sample of 3,008 drug court clients who were not referred to ATR programs across Texas (Mangrum, 2008). To date, only one study has examined the recidivism outcomes of an ATR program serving an offender population. Using a case file review of 434 offenders who participated in Lake City's Access to Recovery post-prison release or as an alternative to community supervision revocation across a 14 month period, 79% of the sample incurred a technical violation of community supervision, 30% were arrested, and 23% were reincarcerated (Seredycz, 2010). These findings are comparable to rates of recidivism with a large, nationally representative sample of offenders (Durose, Cooper, & Snyder, 2014).
ATR does not have a standalone facility or serve as a separate treatment provider; rather, the services provided by ATR are in addition to those already being provided by the client's treatment agency. For example, two separate treatment agencies could provide the same service that is billable through ATR vouchers but one might deliver that treatment in a better way than the other. So it is reasonable to examine whether the specific services provided by ATR are affecting outcomes or rather if there is something about the agency where one receives these services. The effect of organization over treatment has received limited attention in the criminal justice literature, though some have examined substance abuse treatment and practices. Generally speaking, this literature suggests that with the same treatment modalities, differences in organizational structure and service delivery can have direct effects on client program outcomes (see for example Joe, Singh, Lehman, Simpson, & Sells, 1983; Friedmann, Alexander, & D' Aunno, 1999; Heinrich & Lynn, 2002; Heinrich & Fournier, 2004; Heinrich & Fournier, 2005). Therefore, in the present study we assess whether there is an association between each of the billable ATR service categories and recidivism but also whether there is an association between the agency where the client received treatment and recidivism.
Data and Methods
Data for this study were provided to the research team as part of a broader evaluation of the statewide Indiana ATR program. Individuals eligible for Indiana ATR services were adults with a substance abuse problem including any illegal drug abuse, inappropriate prescription medication abuse, and alcohol abuse, who were residing in one of the participating counties, with household incomes at 200% or below the Federal Poverty Line (FPL). Eligible exceptions included individuals with a substance abuse problem who had served in the military and were residing anywhere in Indiana with household incomes at or below 500% FPL. For each client, an assigned recovery consultant collected information using the Center for Substance Abuse Treatment (CSAT) Government Performance and Results Act (GPRA) Client Outcome Measures for Discretionary Programs form (henceforth referred to as the “GPRA form”) during an intake and a six-month follow-up interview. The GPRA form included questions about each client's basic demographic characteristics as well as detailed questions about each client's substance use during the thirty days prior to intake and follow-up interviews. These survey data were then linked to data collected by Indiana ATR personnel on all of the service groupings for which the clients received vouchers.
This research uses a total population sample of 230 ATR clients who were released from prison, returned to Marion County (Indianapolis), Indiana, and received ATR services at one of five designated treatment agencies in Indianapolis between December 2010 and June 2012. Marion County served as the targeted location and demonstration site for this research due to the disproportionate amount of releases to this county relative to all other counties in the state. Data on all ATR clients who completed both an intake and discharge GPRA were given to Indiana Department of Corrections (DOC) personnel who then supplied ATR staff with a merged de-identified file. This file contained the number of prior incarcerations in the DOC, the date of the first incarceration following the ATR GPRA discharge date, and the conviction charges of this first offense. DOC also confirmed that all clients in the sample had previously been incarcerated in prison and had returned to Marion County; however, they did not supply ATR with data on the nature of client's release conditions or the length of time from client's prison release to when they began ATR services. While we do not know the precise time from prison release to treatment, ATR personal reported that most of the clients who were returning inmates had been released within the past month. This was confirmed by the GPRA survey data which indicated that 55.7% (n = 127) of the sample reported currently being on parole or probation and 46.5% (n = 107) having been incarcerated in the 30 days prior to GPRA intake.
From the GPRA data we generated several control variables to be used in our subsequent analysis. Demographic measures of age at GPRA intake, sex, and race/ethnicity are included as well as sociodemographic measures such as the client's highest level of education, current living situation, and current employment status, which were determined using GPRA discharge data. While DOC did not provide ATR with data on the returning inmates condition of release there is a GPRA item that asks clients “Are you currently on parole or probation” which we used as a measure of supervision. As a proxy measure of positive social relationships we use this GPRA item asking “In the past 30 days did you have interaction with family and/or friends that are supportive of your recovery?” The GPRA discharge also asks about the self-reported use of illegal drugs (i.e., use of opiates, cocaine, prescription drugs, marijuana, and alcohol in the past 30 days). As all of the clients had a history of substance abuse, we created an item to measure abstinence (i.e., no self-reported usage) from illegal drugs and alcohol at discharge. Finally, DOC provided ATR staff with a count of the number of prior incarcerations in prison for each of the clients.
To explore ATR services and treatment agency with recidivism, we used billing data provided by ATR to create two independent measures to be used in the analysis below. First, we create a series of dichotomous measures for each of the primary billing categories of ATR services: clinical, social support, recovery, transportation, housing, and peer coaching. These services are not mutually exclusive and so a client might have been billed for any combination of these services. Next we created a variable to capture the agency to which the services were billed. ATR clients received substance abuse treatment and ancillary services at one of five nonprofit treatment agencies in Indianapolis during this study period. As this is not an evaluation of any specific agency we use pseudonyms (Agency A, B, C, D, E) rather than the actual agency names. The number of clients distributed across these agencies, ranged from 33 (Agency E) to 56 (Agency C), with an average number of clients per agency of 46.0 (SD = 8.28). In order to explain potential differences between agencies we gathered publically available information (e.g., IRS Forms 990, 990-EZ, and 990-PF) from an online nonprofit search engine for the years when clients were receiving ATR services.
The dependent variable in this study is recidivism, which is operationalized as readmission to the DOC after the ATR GPRA discharge interview. Recidivism data is collected across an 18 to 36 month follow-up period (M = 24.8). Research examining recidivism outcomes has offered a variety of recidivism definitions and measures. The operationalization used in this research is one of the most conservative measures of recidivism and may capture more information on the severity of the criminal justice system's response than the severity of individual behavior (Maltz, 1984). At the same time, this type of recidivism measure has the benefit of independent review of discretionary decisions (see Batiuk, Moke, & Wilcox Rountree, 1997). Records needed to create alternative measures recidivism were not available. Existing information did not allow for the determination of the offense initiating criminal justice system processing that resulted in a readmission to prison.
Cox regression, a form of survival analysis, was employed to examine recidivism outcomes. One of the strengths of survival analysis techniques is the management of censored data: left censoring occurs when data on the starting point are not available and right censoring when there are no data on the ending point, which often occurs when studying recidivism. In short, survival analysis methods are able to correct for the unequal distribution of follow-up time on the ATR clients. To do this, Cox regression uses the censored and uncensored (i.e., those that did recidivate) cases to calculate the probability of surviving (i.e., not recidivating) for each time point (Box-Steffensmeier & Jones, 2004). We added demographic and treatment agency covariates to the Cox regression equation to predict the hazard rate, which is the probability of the event occurring in a given time period given survival through prior time periods. Therefore, it is able to examine both the likelihood of and time to recidivism post-ATR. All analyses were conducted using IBM's Statistical Package for the Social Sciences© (SPSS) 21.
Results
Sample characteristics
Table 1 displays descriptive statistics for the sample. Average age at ATR entry was 34.9 (SD = 9.22). Nearly three quarters (72.2%) of the sample were males and about half (44.8%) of the population was White. Less than half (40.4%) of the ATR clients were employed six months post intake; of those who were employed, 60.2% (n = 56) were employed full time. Most of the respondents were in some type of housing (75.2%), though some were in a secure living facility (16.5%) or a shelter (8.3%). About one-third of the sample (34.8%) had not completed high school while 20.9% had some schooling beyond high school which included any additional vocational training or college. The majority of clients (90.0%) reported interaction with supportive family members and only 10.4% of clients reported having recently used alcohol or drugs; 89.6% had been abstinent at follow-up. Clients had an average of 3 incarcerations prior to ATR intake (M = 3.10; SD = 1.82) and 55.7% were on probation or parole. Finally, during the 18 to 36 months of the follow-up period, approximately one-third (32.6%, n = 75) of the sample recidivated. To place this recidivism rate in context, the three year post-release readmission rate to DOC in Marion County is 45.9% while the state of Indiana averages a rate of 36.1% during the same time period (Indiana Department of Corrections, 2012).2
Table 1. Sample Characteristics.
| Total Sample (N = 230) | ||
|---|---|---|
|
|
||
| Variable | Mean (SD) | |
| Age at intake | 34.9 (9.22) | |
| Number of prior incarcerations | 3.10 (1.82) | |
| Sex | N | % |
|
|
||
| Female | 64 | 27.8 |
| Male | 166 | 72.2 |
| Race | ||
| Nonwhite | 127 | 55.2 |
| White | 103 | 44.8 |
| Probation or Parole | ||
| Yes | 128 | 55.7 |
| No | 102 | 44.8 |
| Employed, Part/Full | ||
| Yes | 93 | 40.4 |
| No | 137 | 59.6 |
| Housing situation | ||
| Housed | 173 | 75.2 |
| Secure living facility | 38 | 16.5 |
| Shelter | 19 | 8.3 |
| Education | ||
| Less than HS | 80 | 34.8 |
| HS diploma/equiv | 102 | 44.3 |
| Post-HS schooling | 48 | 20.9 |
| Supportive family interaction | ||
| Yes | 207 | 90.0 |
| No | 23 | 10.0 |
| Abstinence from drugs and alcohol | ||
| Yes | 206 | 89.6 |
| No | 24 | 10.4 |
| Recidivism | ||
| Yes | 75 | 32.6 |
| No | 155 | 67.4 |
We conducted means and Chi-square tests to examine whether there were differences in recidivism by the sample characteristics listed in Table 1. Those who recidivated had a greater number of prior arrests than those who did not (3.27 and 2.75 respectively; t = 2.06, p < .05). Clients who are Nonwhite were less likely to recidivate than White clients (25.2% and 41.7% respectively; χ2 = 7.09, p < .01). We also found that clients who were living in a house at ATR discharge (n = 124; 46.1%) were significantly less likely to recidivate than those who were living in a shelter or secure living facility (28.3% and 45.6%, respectively; χ2 = 5.83, p < .05).
ATR Services and Treatment Agencies
We conducted means tests to examine whether there were differences in the sample characteristics listed in Table 1 by treatment agency. The only significant differences were by race and gender. Agency A and Agency C had fewer males (58.3% and 58.9% respectively) than Agency B (89.4%), Agency D (80.4%), and Agency E (78.8%) (χ2 = 18.66, p < .001). Agency B had relatively fewer Nonwhite clients (23.4%) while Agency D had more Nonwhite clients (80.4%) than Agency A (50.0%), Agency C (62.5%), and Agency E (60.6%) (χ2 = 33.18, p < .001). None of the remaining sample characteristics varied by Agency.
Next we explored the use of ATR services by treatment agency. Table 2 shows the primary billing categories of ATR services: clinical, social support, recovery, transportation, housing, and peer coaching. As illustrated in Table 2, the services most utilized by ATR clients were clinical services (78.3%), which included assessments, individual addictions treatment, and detoxification. The next most utilized service was transportation (54.3%), followed by recovery group services (42.6%), housing (39.1%), social support (32.2%), and peer coaching (17.8%). We used analysis of variance (ANOVA) tests to assess whether there were differences in the types of services utilized by ATR clients across the five agencies. As illustrated by the ANOVA results presented on the right hand side of Table 2—with the exception of clinical services, which were the most utilized in each of the treatment agencies—there were significant differences in the use of ATR services by clients across the agencies. For instance, Agency B's clients made use of most of the available ATR services whereas Agency E's clients were below average in their use of ATR recovery group, transportation, housing, and peer group services. Across ATR services, transportation services were more often used by Agency A's clients than Agency E and Agency D's clients.
Table 2. ATR Services Used by Agency.
| Total (N = 230) | Agency A (n = 48) | Agency B (n = 47) | Agency C (n = 56) | Agency D (n = 46) | Agency E (n = 33) | ANOVA | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||||||
| Variable | N | % | N | % | N | % | N | % | N | % | N | % | F(4, 229) |
| Clinical Services | 180 | 78.26 | 38 | 79.17 | 43 | 91.49 | 42 | 75 | 31 | 67.39 | 26 | 78.79 | 2.13 |
| Social Support | 74 | 32.17 | 13 | 27.08 | 9 | 19.15 | 27 | 48.21 | 14 | 30.43 | 11 | 33.33 | 2.8* |
| Recovery Group | 98 | 42.61 | 29 | 60.42 | 35 | 74.47 | 12 | 21.43 | 17 | 36.96 | 5 | 15.15 | 14.36*** |
| Transportation | 125 | 54.35 | 32 | 66.67 | 29 | 61.7 | 35 | 62.5 | 18 | 39.13 | 11 | 33.33 | 4.1** |
| Housing | 90 | 39.13 | 17 | 35.42 | 34 | 72.34 | 24 | 42.86 | 8 | 17.39 | 7 | 21.21 | 10.42*** |
| Peer Coaching | 41 | 17.83 | 12 | 25 | 11 | 23.4 | 9 | 16.07 | 9 | 19.57 | 0 | 0 | 2.57* |
Note. ATR = Access to Recovery.
p < .05.
p < .01.
p < .001.
We used Chi-square tests first to examine the association between ATR services and treatment agencies on the likelihood of recidivism. There were no significant differences between any of the ATR services utilized and the likelihood of recidivism. We examined the services question further by running regression analyses with each of the service categories and recidivism and also explored various combinations of services, yet we found no significant relationship between services and recidivism. However, there was a significant difference between the agency from which ATR clients received treatment and the likelihood of recidivism (χ2 = 23.58, p < .001). As shown in Table 3, Agency A, Agency B, and Agency C had recidivism rates of 43.8%, 46.8%, and 42.4% respectively. Agency C and Agency D both had rates of recidivism that were much lower than the other agencies. Of the 56 ATR clients who received treatment from Agency C, only 26.8% went back to prison and at Agency D only 6.5% of ATR clients' recidivated.
Table 3. Recidivism Rate and Agency Differences.
| Total N | Recidivsma, *** | Number of | Approximate Revenue | |||
|---|---|---|---|---|---|---|
| N | % | NTEE Code | ||||
| Agency A | 48 | 21 | 43.8 | Human Services | 1 | $200,000 |
| Agency B | 47 | 22 | 46.8 | Crime, Legal Related | 1 | $300,000 |
| Agency C | 56 | 15 | 26.8 | Crime, Legal Related | 5 | $300,000 |
| Agency D | 46 | 3 | 6.5 | Crime, Legal Related | 15 | $500,000 |
| Agency E | 33 | 14 | 42.4 | Crime, Legal Related | 5 | $100,000 |
χ2;
p<.001
To further examine the variability of recidivism outcomes of the five agencies where ATR clients received services we descriptively analyzed 2011 and 2012 Internal Revenue Service (IRS) 990 tax form data for each agency (see Table 3). Similar procedures are often used by public affairs and public administration scholars to examine and differentiate the operations of non-profits (see Lecy & Van Slyke, 2013). The IRS uses a classification system, the National Taxonomy of Exempt Entities (NTEE), to categorize nonprofits. As shown in Table 3, with the exception of Agency A, all of the agencies providing ATR services classified themselves as providing crime, legal related, rehabilitation services for offenders (NTEE code I – Crime, Legal Related). Agency A classified themselves as providing human services for personal social services (NTEE code P – Human Services). The relative size of each agency's personnel is measured by 990 tax form by asking about the agency's current officers, directors, trustees, and key employees. Agency size varies from a high of 15 (Agency D) to a low of one (Agencies A and B). At approximately $500,000 Agency D also had the highest total yearly revenue of the agencies. Finally, in looking at each of the organization's mission statement most described substance abuse treatment, prevention, or education, but only Agency D focused specifically on returning inmates. Thus, while all of the agencies worked with those who were involved in the criminal justice system, this was only a primary aim for Agency D. Agency D also differed from the other agencies in the size of their organization.
Predicting Recidivism
To further examine the effect of agency on recidivism we used Cox Regression to predict the hazard of recidivism while controlling for sociodemographic variables.1 Whether or not the event occurs (i.e., recidivism) is dichotomous (1 = yes; 0 = no) and time is measured in days. Table 4 presents the results of these models predicating recidivism. Model 1 looks at the effect of the variables that preceded ATR discharge and shows that race is the only significant predictor of recidivism. Specifically, the hazard of recidivism is 1.8 times greater for White ATR clients than Nonwhite clients.
Table 4. Cox Regression Predicting Redivism Post ATR Discharge.
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| B (SE) | Exp b (95% CI) | B (SE) | Exp b (95% CI) | B (SE) | Exp b (95% CI) | |
| Age | 0.00 (0.01) | 1.00 (0.97-1.03) | 0.00 (0.01) | 1.00 (0.97-1.02) | 0.00 (0.01) | 1.00 (0.97-1.03) |
| Male (yes = 1) | 0.22 (0.27) | 1.25 (0.73-2.13) | 0.21 (0.28) | 1.23 (0.72-2.12) | 0.21 (0.29) | 1.23 (0.69-2.18) |
| Nonwhite (yes = 1) | -0.57 (0.24)* | 0.57 (0.36-0.90) | -0.57 (0.24)* | 0.57 (0.35-0.90) | -0.30 (0.26) | 0.74 (0.44-1.23) |
| Number of prior incarcerations | -0.15 (0.09) | 0.86 (0.73-1.01) | -0.15 (0.09) | 0.86 (0.73-1.02) | -0.12 (0.09) | 0.89 (0.75-1.05) |
| Parole or Probation (yes = 1) | -0.49 (0.25) | 0.61 (0.37-1.00) | -0.42 (0.26) | 0.65 (0.40-1.08) | -0.36 (0.27) | 0.70 (0.41-1.18) |
| Housing situation (1 = home) | -0.59 (0.26)* | 0.56 (0.34-0.92) | -0.68 (0.26)** | 0.51 (0.30-0.85) | ||
| Employment (1 = full or part time) | -0.21 (0.26) | 0.81 (0.49-1.34) | -0.20 (0.26) | 0.81 (0.49-1.37) | ||
| Education (1 = high school or more) | 0.01 (0.25) | 1.01 (0.63-1.64) | 0.14 (0.26) | 1.15 (0.69-1.90) | ||
| Supportive family interaction (1 = yes) | 0.46 (0.45) | 1.58 (0.65-3.82) | 0.37 (0.47) | 1.45 (0.57-3.67) | ||
| Abstinence from drugs and alcohol (1 = yes) | 0.27 (0.39) | 1.32 (0.61-2.83) | 0.33 (0.40) | 1.39 (0.63-3.04) | ||
| Agency A | 0.50 (0.35) | 1.65 (0.83-3.30) | ||||
| Agency B | 0.37 (0.39) | 1.44 (0.67-3.09) | ||||
| Agency C | - | - | ||||
| Agency D | -1.51 (0.64)** | 0.22 (0.06-0.77) | ||||
| Agency E | 0.65 (0.40) | 1.91 (0.86-4.23) | ||||
| -2 log likelihood x2 | 772.91* | 765.44* | 745.54*** | |||
N = 230;
p<.05,
p<.01,
p<.001
Model 2 adds measures that were captured at ATR discharge. Dummy variables were created for employment (1 = employed full or part time, 0 = unemployed), education (1 = high school degree or above, 0 = no high school degree), and housing (1 = living in a house, 0 = living in either a shelter, institution, or other). In Model 2, race remains significant and shows that housing is also a significant predictor of recidivism post ATR; those ATR clients who were not living in their own home at ATR discharge had a hazard of recidivism 2.0 times higher than those who were living in their own home.
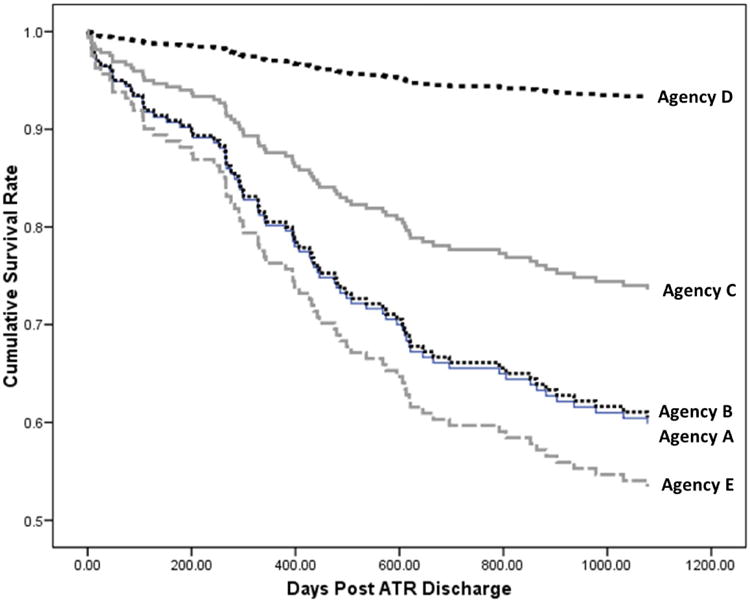
Finally, Model 3 adds the dummy variables to measure the effect of the treatment agency on recidivism. We use Agency C as the reference group because it has the largest size and would produce the smallest standard errors (Hardy, 1993). Model 3 shows that after controlling for social demographics, prior arrests, and substance abstinence, there is a strong effect of treatment agency on recidivism; ATR clients from Agency D were significantly less likely to recidivate. In separate models not shown we used Agency D as the reference category and here ATR clients from Agency A, Agency B, Agency C, and Agency E were all significantly more likely to recidivate than those from Agency D. The ATR clients who were at Agency D had a hazard of recidivism 1.2 times less than those at other agencies, controlling for other variables in the model. To illustrate this, Figure 1 displays the estimated cumulative probability of recidivism by treatment agency net of the variables in Model 3. The cumulative survival rate is the proportion of ATR clients who had not recidivated during each follow-up month, with the distance between the lines representing the additional effect of the treatment agency at each time point. As shown in the figure, ATR clients from Agency D had a significantly lower rate and longer time to recidivism than clients from the other agencies.
Figure 1. Time to Recidivism for ATR Clients Post Discharge.
Discussion
The increasing rate of returning prisoners in the United States has forced policy makers to recognize the needs of this growing population (Clear & Frost, 2014). A large portion of these returning inmates have a substance abuse problem yet few of them receive any treatment while incarcerated. Many offenders will use community-based treatment to address their substance use. This study examined a sample of former Indiana inmates with substance abuse problems who were engaged ATR, a community-based treatment program that offers ancillary wraparound support services. We examined participation ATR and recidivism and explored whether reduced recidivism was associated with any specific ATR service or the agency where client's received services.
Overall, 36.2% of the ATR clients in the sample recidivated across an 18 to 36 month follow-up period. Our analysis of ATR follow-up interview data showed that after discharge, the majority of clients reported not using any alcohol or drugs and having positive interactions with family and friends regarding their recovery; however, these outcomes were not associated with decreased recidivism. Contrastingly, race and housing were associated with recidivism. Nonwhite clients and those living in a house were significantly less likely to recidivate than White clients and those living in a shelter or secure facility. While the differences by race categories are inconsistent with much of the criminal justice literature on recidivism correlates (see Huebner & Berg, 2011), it is worth noting that there are not significant disparities in recidivism rates by race within Marion County. According to DOC, the recidivism rate is 39.2% for Caucasian inmates and 40.0% for African American inmates (IDOC, 2012). Nationally, recidivism is highest among African American inmates but the gap between African American and Caucasian inmates has significantly narrowed in the past 11 years (Durose et al., 2014). In terms of housing, previous research has demonstrated the ability of permanent supportive housing to decrease substance use, increase services engagement, and decrease engagement in criminal behavior (Bean, Shafer, & Glennon, 2013; Tsemberis, Kent, & Respress, 2012).
In considering these findings as well as the non-significant association between demographic measures of age, sex, and criminal history on recidivism it is important to note that we are looking at a very niche sample of inmates. Recall the sample consists of persons from a low socioeconomic status home 200% to 500% below the Federal Poverty Line in one county, who had a history of substance abuse, who were receiving substance abuse treatment, and completed both the intake and exit GPRA. It is therefore difficult to ascertain whether relationships between demographic characteristics and recidivism should or should not be expected for the sample used in this research. Replication of this study using similar sampling frames will be needed to examine the robustness of common recidivism factors among persons in extreme poverty. Considerable care must be exercised when attempting to generalize the findings of this research to the broader formerly incarcerated client population.
In analyzing the ATR billing codes, we found that clinical services were the most frequently used by all treatment agencies. Beyond that, significant differences in the use of other services by agency suggest that that ATR services fluctuated according to the resources of the agency and needs of their clients. Services offered by ATR were not associated with clients' likelihood of recidivism, whether categorized differently, or examined separately.
While the type of ATR services clients received was not associated with recidivism, the treatment agency delivering the services was. Agencies C and D had relatively lower rates of recidivism relative to Agency A, Agency B, and Agency E. Agency D in particular had a tremendously low recidivism rate. Of the 43 ATR clients who received treatment and support services at Agency D, 93.5% had not been re-incarcerated. This is an especially important finding in that our post-hoc analysis of IRS tax forms showed that Agency D had the highest total revenue, the largest number of administrators and key employees, and was the only agency to focus specifically on offender reentry issues and not just substance abuse for those in the criminal justice system. To further examine these effects on the likelihood of recidivism we conducted survival analysis. This analysis reflected the previously discussed association between race and housing on recidivism and also showed that net of sociodemographic covariates, the treatment agency from which ATR clients received services had an effect on the likelihood to recidivate. Specifically, we found that after controlling for social demographics and substance use, ATR clients who received services from Agency D were less likely to recidivate than clients who attended any of the other agencies. Given the importance of housing on recidivism among this sample, it is also important to point out that clients at Agency D were less likely to utilize housing services than the other agencies. It is possible that this group may not have needed housing, which appears to be a protective factor for the overall sample.
In interpreting these results, some limitations should be kept in mind. First, ATR eligibility criteria and the program model's active elements of voluntary participation and client empowered choice to select the best combination of clinical and support services make it difficult to construct an adequate comparison group for a rigorous outcome evaluation. Randomized controlled trials assigning eligible clients to ATR and non-ATR conditions or quasi-experimental approaches using a pool of recently released individuals with substance abuse problems matched on relevant variables can provide important evidence on the efficacy of ATR. Either approach would be incapable of randomizing or prospectively matching individual decision-making and choice of services. Future research will need to make use of innovative methods to ameliorate these challenges and add to the ATR knowledge base for offender populations. Second, there were limitations related to ATR service delivery. It was not possible to assess the quality of the ATR services provided by treatment agencies, examine the supplemental services provided by the treatment agencies, or dissect the organizational and operational differences among ATR agencies. Finally, this study was under the constraints of having to use multiple sources of administrative data. From the ATR GPRA data to DOC measures of recidivism, there were many data collection aspects of this study that could be improved upon. For example, alternative measures of recidivism, precise measures of when offenders were released and when they started ATR, measures of supervision type and length of supervision, information on the communities where ATR clients resided, and how they came to select an ATR provider. Unfortunately, we do not have access to identifiable data on the ATR clients in this sample and cannot obtain any additional information. While it is difficult to control for everything that might affect recidivism, these additional measures would help to rule out rival explanations and help to explain the association between agency and recidivism found in this study. Moreover, we do not have data on how ATR clients came to select the agency where they received services, which is a key factor that might help to explain the results in this study. Yet, despite these limitations, this study offers important insight into the usefulness of ATR, and similar substance abuse recovery support services for returning inmates, and adds to the literature on community-based substance abuse treatment for correctional populations. It is our hope that this study will stimulate further research into these programs to determine how they can be most effective for offender's reintegration process.
Conclusion
While the literature on ATR is scarce, preliminary evidence suggests that the additional services provided by ATR help to fill in the gaps left by other substance abuse recovery programs and that this has a positive effect on substance use (Buchanan, 2014; Cousins, et al., 2012; Krupski, et al., 2009; McCabe et al., 2013). In this study we did not look at ATR and substance abuse but rather we examined ATR's goal to serve the substance abuse needs of returning inmates in an effort to reduce rates of recidivism. Based on the findings of this study we suggest that reductions in recidivism are largely driven by the agency where clients received the ATR services. Agencies that use ATR services who are more established in terms of revenue and staff, and who have the explicit goal to deal with returning inmates, can be more successful in reducing recidivism than less established agencies that focus only on substance abuse. This suggests that when conceptualizing and implementing community-based treatments, or supplementing existing services through ATR initiatives, is important to assess the overall goals, missions, and capabilities of the agencies providing services. Those treatment agencies with experience working with offender populations and assisting reentry needs are the best able to utilize the ancillary services provided by ATR to reduce subsequent criminal behaviors. As one of the key principles for effective correctional interventions, responsivity can limit or amplify the effectiveness of community-based substance abuse treatment and shape recidivism outcomes (Andrews & Bonta, 2010). While research should continue to inform substance abuse treatment policies and initiatives for recently released offenders, future efforts should examine organizational components and the capacity for treatment agencies to deliver clinical and supportive services. Attention to these dynamics will provide much needed knowledge on the use of community-based substance abuse treatment approaches.
Acknowledgments
Funding for this project was provided by the Indiana Family and Social Services Administration's Division of Mental Health and Addiction, The Solution Center at Indiana University-Purdue University Indianapolis, and the National Institutes of Health/National Center for Advancing Translational Science (Award #KL2TR001106). We would like to thank Julia Carboni for helpful comments on previous drafts of this manuscript.
Footnotes
We conducted the same analysis looking at ATR services and did not find any significant effects.
Separate analysis were conducted (not shown here) in which we consolidated services categories (e.g., clinical vs. social support services), and still no significant differences were found.
According to the IDOC 5,307 inmates were released in Marion County, Indiana in 2009 with 2,435 readmitted to prison in a three year follow-up period. Similarly, 18,873 inmates were released to the state of Indiana as a whole with 6,812 readmitted to prison in a three year follow-up period. It is important to note that IDOC recidivism rates for Marion County and the overall state of Indiana are provided for contextual purposes. IDOC rates should not be used to determine the efficacy of ATR as the methods used to estimate recidivism rates are different. IDOC rates are based on a full three-year follow-up period, while the rate for the current sample is based upon an 18 to 36 month follow-up period. Also, IDOC rates are estimated using an at risk period beginning at release from prison. The at-risk period in this study begins post-ATR discharge.
References
- Andrews DA, Bonta J. The psychology of criminal conduct. 5th. New Providence, NJ: Matthew Bender & Company, Inc; 2010. [Google Scholar]
- Anglin MD, Longshore D, Turner S. Treatment alternatives to street crime - An evaluation of five programs. Criminal Justice and Behavior. 1999;26(2):168–195. [Google Scholar]
- Aos S, Miller MG, Drake E. Evidence-based adult corrections programs: What works and what does not. Olympia, WA: Washington State Institute for Public Policy; 2006. [Google Scholar]
- Bahr SJ, Masters AL, Taylor BM. What works in substance abuse treatment programs for offenders? Prison Journal. 2012;92(2):155–174. [Google Scholar]
- Batiuk ME, Moke P, Wilcox Rountree P. Crime and rehabilitation: Correctional education as an agent of change – A research note. Justice Quarterly. 1997;14(1):167–180. [Google Scholar]
- Bean KF, Shafer MS, Glennon M. The impact of housing first and peer support on people who are medically vulnerable and homeless. Psychiatric Rehabilitation Journal. 2013;36(1):48–50. doi: 10.1037/h0094748. [DOI] [PubMed] [Google Scholar]
- Blumstein A, Beck AJ. Reentry as a transient state between liberty and recommitment. In: Travis J, Visher C, editors. Prisoner reentry and crime in America. New York: Cambridge University Press; 2005. pp. 50–79. [Google Scholar]
- Bourdieu P. The forms of capital. In: Richardson JG, editor. Handbook of theory and research for the sociology of education. New York, NY: Greenwood; 1985. pp. 241–258. [Google Scholar]
- Boyum DA, Caulkins JP, Kleinman MAR. Drugs, crime, and public policy. In: Wilson JQ, Petersilia J, editors. Crime and public policy. Oxford, UK: Oxford University Press; 2011. pp. 368–410. [Google Scholar]
- Box-Steffensmeier JM, Bradford SJ. Event history modeling : a guide for social scientists. New York: Cambridge University Press; 2004. [Google Scholar]
- Buchanan V. Effective addiction recovery support: A quantitative evaluation of Indiana's Access to Recovery (INATR) Program Unpublished master's thesis. Indiana University Richard M. Fairbanks School of Public Health at IUPUI; Indianapolis, IN: 2014. [Google Scholar]
- Carson AE, Sabol WJ. Prisoners in 2011. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2012. [Google Scholar]
- Chandler RK, Fletcher BW, Volkow ND. Treating drug abuse and addiction in the criminal justice system: Improving public health and safety. Journal of the American Medical Association. 2009;301(2):183–190. doi: 10.1001/jama.2008.976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chanhatasilpa C, MacKenzie DL, Hickman LJ. The effectiveness of community-based programs for chemically dependent offenders - A review and assessment of the research. Journal of Substance Abuse Treatment. 2000;19(4):383–393. doi: 10.1016/s0740-5472(00)00131-8. [DOI] [PubMed] [Google Scholar]
- Clear TR, Frost N. The punishment imperative: The rise and failure of mass incarceration in America. New York, NY: New York University Press; 2014. [Google Scholar]
- Cloud W, Granfield R. Conceptualizing recovery capital: Expansion of a theoretical construct. Substance Use & Misuse. 2008;43(12-13):1971–1986. doi: 10.1080/10826080802289762. [DOI] [PubMed] [Google Scholar]
- Coleman JS. Social capital and the creation of human capital. The American Journal of Sociology. 1988;94(S):S95–S120. [Google Scholar]
- Cousins SJ, Antonini VP, Rawson RA. Utilization, measurement, and funding of recovery supports and services. Journal of Psychoactive Drugs. 2012;44(4):325–333. doi: 10.1080/02791072.2012.718924. [DOI] [PubMed] [Google Scholar]
- Durose MR, Cooper A, Snyder HN. Recidivism of prisoners released in 30 states in 2005: Patterns from 2005 to 2010. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2014. [Google Scholar]
- Farabee D, Prendergast ML, Cartier J, Wexler H, Knight K, Anglin MD. Barriers to implementing effective correctional drug treatment programs. The Prison Journal. 1999;72(2):150–162. [Google Scholar]
- Friedmann PD, Alexander JA, D'Aunno TA. Organizational correlates of access to primary care and mental health services in drug abuse treatment units. Journal of Substance Abuse Treatment. 1999;16(1):71–80. doi: 10.1016/s0740-5472(98)00018-x. [DOI] [PubMed] [Google Scholar]
- Friedmann PD, Taxman FS, Henderson CE. Evidence-based treatment practices for drug-involved adults in the criminal justice system. Journal of Substance Abuse Treatment. 2007;32(3):267–277. doi: 10.1016/j.jsat.2006.12.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granfield R, Clouds W. Social capital and natural recovery: The role of socila relationships in overcoming addiciton without treatment. Substance Use & Misuse. 2001;36(11):1543–1579. doi: 10.1081/ja-100106963. [DOI] [PubMed] [Google Scholar]
- Grommon E, Davidson W, Bynum T. A randomized trial of a multimodal community-based prisoner reentry program emphasizing substance abuse treatment. Journal of Offender Rehabilitation. 2013;52(4):287–309. [Google Scholar]
- Grommon EL. Prisoner reentry programs: Penetrating the black box for better theory and practice. El Paso: LFB Scholarly Pub; 2013. [Google Scholar]
- Hardy MA. Regression with dummy variables. Newbury Park, CA: Sage; 1993. [Google Scholar]
- Heinrich CJ, Lynn LE., Jr Improving the organization, management, and outcomes of substance abuse treatment programs. The American journal of drug and alcohol abuse. 2002;28(4):601–622. doi: 10.1081/ada-120015871. [DOI] [PubMed] [Google Scholar]
- Heinrich CJ, Fournier E. Dimensions of Publicness and Performance in Substance Abuse Treatment Organizations. Journal of Policy Analysis and Management. 2004;23(1):49–70. doi: 10.1002/pam.10178. [DOI] [PubMed] [Google Scholar]
- Heinrich CJ, Fournier E. Instruments of Policy and Administration for Improving Substance Abuse Treatment Practice and Program Outcomes. Journal of Drug Issues. 2005;28(4):601–22. [Google Scholar]
- Huebner BM, Berg MT. Examining the sources of variation in risk for recidivism. Justice Quarterly. 2011;28(1):146–173. [Google Scholar]
- Indiana Department of Corrections. 2012 Recidivism Report: 2009 Releases. 2012 Retrieved from http://www.in.gov/idoc/files/2012_Adult_Recidivism_CountyofCommit.pdf.
- Joe GW, Singh BK, Lehman W, Simpson DD. Agency Differences in Posttreatment Outcomes: A Follow-Up of Drug Abuse Treatment Clients. Substance Use & Misuse. 1983;18(4):523–538. doi: 10.3109/10826088309033035. [DOI] [PubMed] [Google Scholar]
- Karberg JC, James DJ. Substance dependence, abuse, and treatment of jail inmates, 2002. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2002. [Google Scholar]
- Krupski A, Campbell K, Joesch JM, Lucenko BA, Roy-Byrne P. Impact of Access to Recovery services on alcohol/drug treatment outcomes. Journal of Substance Abuse Treatment. 2009;37(4):435–442. doi: 10.1016/j.jsat.2009.05.007. [DOI] [PubMed] [Google Scholar]
- Langan PA, Levin DL. Recidivism of prisoners released in 1994. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2002. [Google Scholar]
- Lattimore PK, Steffey DM, Visher CA. Prisoner reentry experiences of adult males: Characteristics, service receipt, and outcomes of participants in the SVORI multi-site evaluation. Washington, DC: US Department of Justice, National Institute of Justice; 2009. [Google Scholar]
- Laudet AB, Humphreys K. Promoting recovery in an evolving policy context: What do we know and what do we need to know about recovery support services? Journal of Substance Abuse Treatment. 2013;45(1):126–133. doi: 10.1016/j.jsat.2013.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laudet AB, Stanick V, Sands B. What could the program have done differently? A qualitative examination of reasons for leaving outpatient treatment. Journal of Substance Abuse Treatment. 2009;37(2):182–190. doi: 10.1016/j.jsat.2009.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lecy JD, Van Slyke DM. Nonprofit sector growth and density: Testing theoris of government suport. Journal of Public Administration Research and Theory. 2013;23(1):189–214. [Google Scholar]
- Longshore D, Turner S, Fain T. Effects of case management on parolee misconduct- The Bay Area Services Network. Criminal Justice and Behavior. 2005;32(2):205–222. [Google Scholar]
- Lurigio AJ. Drug treatment availability and effectiveness- Studies of the general and criminal justice populations. Criminal Justice and Behavior. 2000;27(4):495–528. [Google Scholar]
- Lyons T, Lurigio A. The role of recovery capital in the community reentry of prisoners with substance use disorders. Journal of Offender Rehabilitation. 2010;49(7):445–455. [Google Scholar]
- Mangrum L. Creating access to recovery through drug courts. Austin, TX: Gulf Coast Addiction Technology Transfer Center; 2008. [Google Scholar]
- Martin SS, Inciardi JA. Case management outcomes for drug-involved offenders. The Prison Journal. 1997;77(2):168–183. [Google Scholar]
- McCabe BE, Santinsteban DA, Mena MP, Duchene DM, McClean C, Monroe M. Engagement, retention, and abstinence for three types of opioid users in Florida. Substance Use & Misuse. 2013;48:623–643. doi: 10.3109/10826084.2013.800112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minton TD. Jail inmates at midyear 2011: Statistical tables. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2012. [Google Scholar]
- Mitchell O, Wilson DB, MacKenzie DL. Does incarceration-based drug treatment reduce recidivism? A meta-analytic synthesis of the research. Journal of Experimental Criminology. 2007;3:353–375. [Google Scholar]
- Morani NM, Wikoff N, Linhorst DM, Bratton S. A Description of the self-identified needs, service expenditures, and social outcomes of participants of a prisoner-reentry program. Prison Journal. 2011;91(3):347–365. [Google Scholar]
- Mumola C, Karberg JC. Drug Use and Dependence, State and Federal Prisoners, 2004. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 2006. [Google Scholar]
- Petersilia J. From cell to society: Who is returning home? In: Visher JTC, editor. Prison reentry and crime in America. New York, NY: Cambridge University Press; 2005. pp. 15–49. [Google Scholar]
- Prendergast ML. Interventions to promote successful re-entry among drug abusing parolees. Addiction Science and Clinical Practice. 2009;5:4–13. doi: 10.1151/ascp09514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seredycz MA. Offender drug abuse and recidivism: An Access to Recovery program. El Paso, TX: LFB Scholarly Pub; 2010. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Access To Recovery Programming. 2006 Document retrieved January 11, 2006: http://atr.samhsa.gov/AggregateDataProfiles.aspx.
- Taxman F, Perdoni M, Caudy M. The plight of providing appropriate substance abuse treatment services to offenders: Modeling the gaps in service delivery. Victims & Offenders. 2013;8:70–93. [Google Scholar]
- Taxman F, Perdoni M, Harrison L. Drug treatment services for adult offenders: The state of the state. Journal of Substance Abuse Treatment. 2007;32(3):239–254. doi: 10.1016/j.jsat.2006.12.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsemberis S, Kent D, Respress C. Housing stability and recovery among chronically homeless persons with co-occuring disorders in Washington, DC. American Journal of Public Health. 2012;102(1):13–16. doi: 10.2105/AJPH.2011.300320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Visher CA, Travis J. Transitions from prison to community: Understanding individual pathways. Annual Review of Sociology. 2003;29:89–113. [Google Scholar]
- Warner TD, Kramer JH. Closing the revolving door? Substance abuse treatment as an alternative to traditional sentencing for drug-dependent offenders. Criminal Justice & Behavior. 2009;36:89–109. [Google Scholar]
- Winterfield L, Lattimore PK, Steffey DM, Brumbaugh S, Lindquist C. The Serious and Violent Offender Reentry Initiative: Measuring the effects on service delivery. Western Criminological Review. 2009;72(2):3–19. [Google Scholar]
- Zhang SX, Roberts REL, Callanan VJ. Preventing parolees from returning to prison through community-based reintegration. Crime & Delinquency. 2006;52:551–571. [Google Scholar]
- Zhang SX, Roberts REL, Lansing AE. Treatment or else: Coerced treatment for drug-involved California parolees. International Journal of Offender Therapy and Comparative Criminology. 2013;57(7):766–791. doi: 10.1177/0306624X12440253. [DOI] [PubMed] [Google Scholar]