

Charcot joint (CJ), also known as neurotrophic arthropathy, is secondary to diabetes, syringomyelia, spinal tuberculosis, etc. The clinical manifestations are varied. The main performance includes pain, slightly restricted joint movement and very obvious swelling and damage of joint. It is easy to be misdiagnosed when the joint is the first symptom. We report a case of Charcot elbow joint as the initial symptom in Chiari malformation with syringomyelia.
A 44-year-old woman was admitted to our hospital with a 3-month history of left elbow pain. Three months ago, she had an onset of left elbow pain without apparent inducement. The pain was mild and intermittent. Her left elbow got swelling and deformity but the activities were not limited. Shortly afterward atrophy of the left-thenar muscle and numbness of ulnar two fingers on left hand had begun to surface. Her physical examination indicated left elbow deformity, swelling, bone rubbing feeling after the activity, without pain or tenderness in joint activity. The tactile, pain and temperature sensation below the left elbow decreased. The topesthesia and graphesthesia were normal yet. Double Hoffman and Babinski signs were also negative. X-ray films [Figure 1a] in outer court showed the destruction and abnormality of the left elbow joint. Cervical magnetic resonance imaging (MRI) [Figure 1b] in our hospital pointed out: Chiari malformation associated with syringomyelia.
Figure 1.
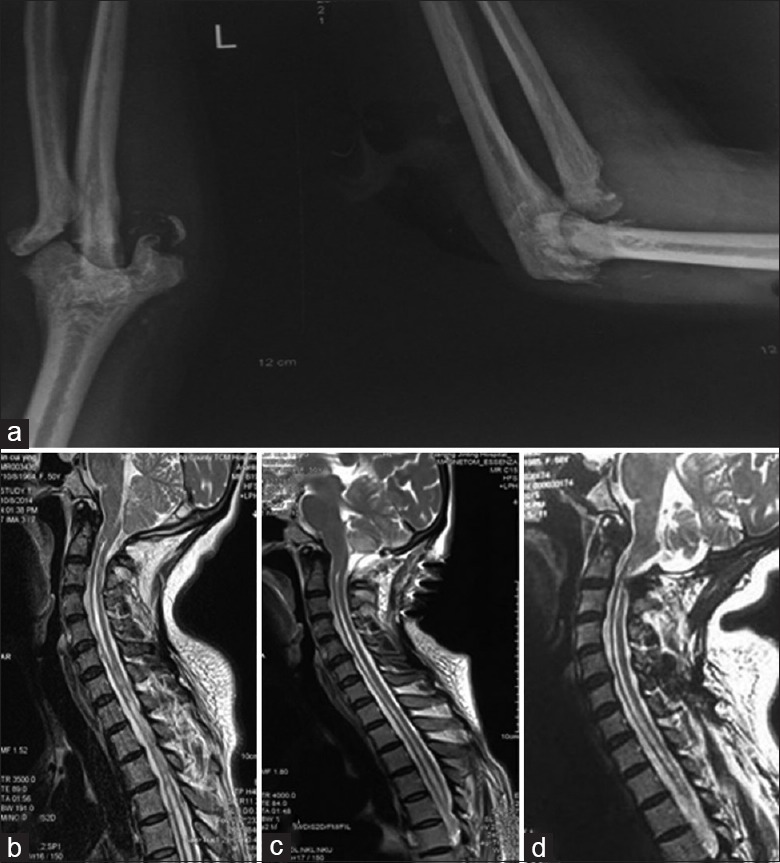
X-ray radiograph of the left Charcot elbow joint and sagittal T2-weighted magnetic resonance imaging demonstrating the evolution of Chiari malformation associated with syringomyelia. (a) X-ray radiograph of the left elbow demonstrating destructive arthropathy and slight calcification. (b) Sagittal T2-weighted of preoperative magnetic resonance imaging demonstrating type I Chiari malformation with syringomyelia from cervical region to thoracic region. (c) Seven days after surgery demonstrating good cerebellar retraction and significant reduced syringomyelia. (d) Half a year after surgery demonstrating no significantly changed syringomyelia.
Patient underwent local brake of the left elbow joints immediately and craniocervical decompression within 3 days after initial admission. After symptomatic treatment postoperation, the pain of left elbow and the numbness on the left hand were relieved. Three days after the operation, MRI [Figure 1c] showed that the cerebellar retraction was good, and syringomyelia was significantly reduced. Half a year after discharge, review of MRI [Figure 1d] showed syringomyelia had no significant change.
CJ was described in detail for the 1st time by a French Doctor Charcot in 1868, which was a destructive joint disease due to abnormal sensory nerve and nervous nutritional disorders. It is more common in adults and patients over the age of 40. Mostly one joint is involved, and sometimes two or three joints maybe. CJ has an occult onset. It has only sensory nerve involvement and no motor nerve invasion, so it would not affect body movement. Frequent symptoms include the swelling and relaxation of the joint, abnormal activity, numbness of the affected limb, hypalgesia or analgesia, walking instability. It even has a deformity or overactive joint, which has the touch of cystic sensation or mobilizable lumps. The severity of joint destruction and symptoms of patients are disproportionate.[1] Correspondingly, our patient displayed elbow deformity, the mild pain of left elbow, numbness on left ulnar two fingers without pain or tenderness in joint activity. Nevertheless, correct diagnosis of CJ needs further assistant examination due to nonspecific clinical manifestations.
As the X-ray examination can display the bone change well, X-ray combined with the clinical situation are the first choice for the diagnosis of CJ. According to the X-ray manifestations, CJ is divided into the hardening type, the absorption type and the mixed type.[2] The X-ray film in our case showed narrow elbow space, dislocation of the joint, bone resorption and ossification in the surrounding soft tissue. Thus, our case belonged to the absorption type, which was consistent with the diagnostic criteria of CJ. However, treatment of CJ should first focus the primary disease, and it is important to find the primary disease. MRI has received more and more attention in virtue of its role and value in the examination of the joints lesions. It is very useful for the cause of CJ. MRI findings of our case confirmed the existence of Chiari malformation and syringomyelia.
Cases of elbow CJ as the initial symptom in Chiari malformation associated with syringomyelia are rare so far. The treatment focuses on the early treatment of the primary disease, which refers to craniocervical decompression mainly. In general, lesions of the joints do not need surgical treatment. Instead, the temporary brake can protect the joint well.[3] Our example took above methods and achieved good results. With regard to the late CJ, the knee fusion can be considered for the greatest degree of retention of limb function and improvement of the quality of life.
In conclusion, for CJ induced by Chiari malformation with syringomyelia, early diagnosis is the key to improve the prognosis. Since the pain of CJ patients is not obvious, they rarely receive regular treatment in the early stage, and more of them see a Doctor in Department of Orthopedics or Department of Rheumatism. It is important that doctors should not only pay attention to the joint performance while ignoring the signs and symptoms of the nervous system but also interrogate history at length, make a careful physical examination and combine with imaging examination to make comprehensive analysis to avoid misdiagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Yi Cui
REFERENCES
- 1.Deng X, Wu L, Yang C, Xu Y. Neuropathic arthropathy caused by syringomyelia. J Neurosurg Spine. 2013;18:303–9. doi: 10.3171/2012.11.SPINE12860. [DOI] [PubMed] [Google Scholar]
- 2.Kumar S, Sharma V, Kumar S, Jain S. Imaging findings in Chiari I malformation with syringomyelia in a case of Charcot shoulder. J Clin Imaging Sci. 2011;1:46. doi: 10.4103/2156-7514.85173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sahoo SK, Salunke P. Charcot arthropathy of the elbow joint as a presenting feature of Chiari malformation with syringomyelia. Br J Neurosurg. 2014;28:811–2. doi: 10.3109/02688697.2014.944482. [DOI] [PubMed] [Google Scholar]