

Abstract
A 58-year-old male was admitted with history of shortness of breath and recurrent fever since two months. He had undergone permanent pacemaker implantation six years back for complete heart block. The patient was persistently having thrombocytopenia. Echocardiographic examination revealed mass (size 4.28 cm2) attached to pacemaker lead in right atrium. The patient was scheduled for open-heart surgery for removal of right atrial mass. During surgery, pacemaker leads and pulse generator were also removed along with mass considering the possible source of infection.
Keywords: Pacemaker leads, Thrombocytopenia, Infective endocarditis
A 58-year-old male was admitted with history of shortness of breath and recurrent fever since two months. He had undergone permanent pacemaker implantation six years back for complete heart block (Fig. 1). He was already on broad-spectrum antibiotics injections teicoplanin and meropenem intravenously for five days before coming to our center. The patient was evaluated thoroughly. Blood, urine, and sputum culture were investigated which were negative. The patient was persistently having thrombocytopenia with platelet counts less than 50,000 μL. Investigations ruled out any medical cause for thrombocytopenia. Echocardiographic examination revealed mass (size 4.28 cm2) attached to pacemaker lead in right atrium (Fig. 2, Fig. 3). The mass was bouncing on tricuspid valve, with high embolic potential (Video clips 1–3). The patient was scheduled for open-heart surgery for removal of right atrial mass. During surgery, pacemaker leads and pulse generator were also removed along with mass considering the possible source of infection (Fig. 4). Ventricular epicardial pacing lead was attached and the other end of the lead was brought to left infraclavicular subcutaneous fossa from the chest cavity. The lead was connected with new external pulse generator implanted in the infraclavicular subcutaneous fossa (Fig. 5). The patient received one unit of platelet apheresis intraoperatively. Histopathological examination of the mass revealed well-organized thrombotic tissue. Bacterial and fungal culture of mass, pacing lead, and pulse generator did not grow any organisms. Postoperative course was stable and uneventful. In the present case, mass might have been infective initially which later became sterile after considerable duration of antibiotics coverage. Thrombocytopenia was due to consumption of platelets by right atrial thrombotic mass. The patient was having normal platelet counts on follow-up.
Fig. 1.
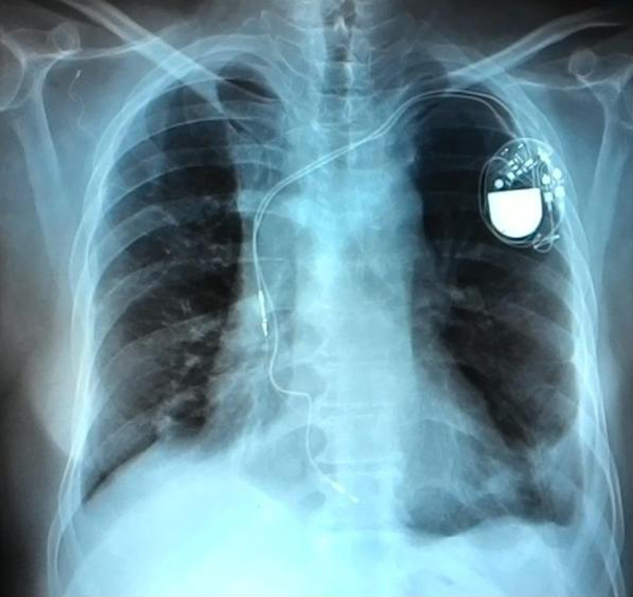
Preoperative chest X-ray showing permanent pacemaker.
Fig. 2.
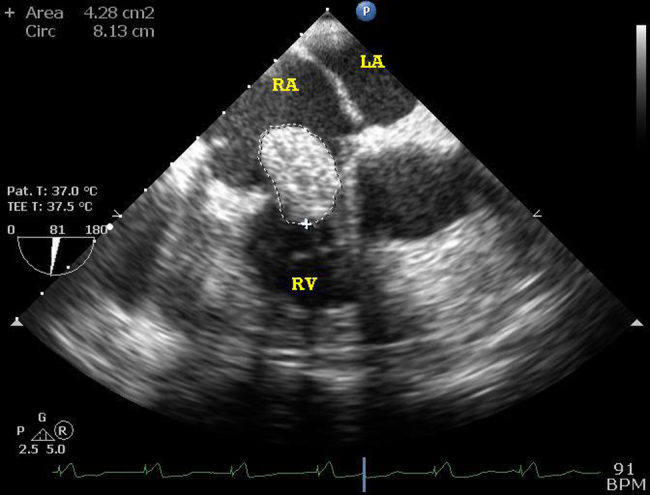
Transesophageal echocardiography showing size of RA thrombotic mass.
Fig. 3.

Transesophageal echocardiography showing RA thrombotic mass on tricuspid valve and RV pacing lead.
Fig. 4.

Thrombus with pacing lead.
Fig. 5.

Post-operative chest X-ray showing permanent pacemaker with epicardial ventricular pacing lead.
A 58-year-old male was admitted with history of shortness of breath and recurrent fever since two months. He had undergone permanent pacemaker implantation six years back for complete heart block (Fig. 1). He was already on broad-spectrum antibiotics injections teicoplanin and meropenem intravenously for five days before coming to our center. The patient was evaluated thoroughly. Blood, urine, and sputum culture were investigated which were negative. The patient was persistently having thrombocytopenia with platelet counts less than 50,000 μL. Investigations ruled out any medical cause for thrombocytopenia. Echocardiographic examination revealed mass (size 4.28 cm2) attached to pacemaker lead in right atrium (Fig. 2, Fig. 3). The mass was bouncing on tricuspid valve, with high embolic potential (Video clips 1–3). The patient was scheduled for open-heart surgery for removal of right atrial mass. During surgery, pacemaker leads and pulse generator were also removed along with mass considering the possible source of infection (Fig. 4). Ventricular epicardial pacing lead was attached and the other end of the lead was brought to left infraclavicular subcutaneous fossa from the chest cavity. The lead was connected with new external pulse generator implanted in the infraclavicular subcutaneous fossa (Fig. 5). The patient received one unit of platelet apheresis intraoperatively. Histopathological examination of the mass revealed well-organized thrombotic tissue. Bacterial and fungal culture of mass, pacing lead, and pulse generator did not grow any organisms. Postoperative course was stable and uneventful. In the present case, mass might have been infective initially which later became sterile after considerable duration of antibiotics coverage. Thrombocytopenia was due to consumption of platelets by right atrial thrombotic mass. The patient was having normal platelet counts on follow-up.
Conflicts of interest
The authors have none to declare.
Footnotes
Supplementary material related to this article can be found, in the online version, at doi:10.1016/j.ihj.2015.11.028.
Appendix A. Supplementary data
The following are Supplementary data to this article:
Transesophageal echocardiographic mid-esophageal modified bicaval view showing RA thrombotic mass bouncing on tricuspid valve.
{kind=link}
Transesophageal echocardiographic mid-esophageal RV inflow–outflow view showing RA thrombotic mass bouncing on tricuspid valve and pacing lead.
{kind=link}
Transesophageal echocardiographic mid-esophageal 4-chamber view showing RA thrombotic mass bouncing on tricuspid valve.
{kind=link}
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Transesophageal echocardiographic mid-esophageal modified bicaval view showing RA thrombotic mass bouncing on tricuspid valve.
Transesophageal echocardiographic mid-esophageal RV inflow–outflow view showing RA thrombotic mass bouncing on tricuspid valve and pacing lead.
Transesophageal echocardiographic mid-esophageal 4-chamber view showing RA thrombotic mass bouncing on tricuspid valve.