

Abstract
Objective: Assess the long-term results of distal femoral varusing osteotomy and try to establish predictive criteria that could help on selecting patients to be submitted to this technique. Methods: Fifteen patients with lateral compartment osteoarthritis and valgus deformity of the knee were submitted to distal femoral “V” varusing osteotomy fixated with lateral plate, pursuing knee alignment at 0° on the anatomical axis. The mean follow-up period was 81.4 months, ranging from 43 to 132 months. The Knee Society Rating System protocol was employed. Additional assessed variables were the following: patient age, follow-up time, and postoperative anatomical angle. Results: 11 results were regarded as excellent or good (73%) and four as fair or poor (27%). Conclusion: Distal femoral “V” varusing osteotomy constitutes a good treatment alternative for patients with lateral compartment osteoarthritis and valgus knee. The following variables have not been confirmed: patient age at the time of surgery, follow-up time, and postoperative anatomical angle as predictive factors for the results.
Keywords: Osteotomy, Osteoarthritis, Knee
INTRODUCTION
Gonarthrosis, or degenerative arthritis of the knee, often evolves with the axis of the limb changing, in varus or valgus, which is more rare. In varus knee, the primary deformity occurs in the tibia, while in valgus, the femur is most affected, leading to the obliquity of the joint line(1).
Valgus deformity tends to progress to osteoarthritis later in life, and is generally less symptomatic. This is explained by the adduction moment, which places the force of gravity primarily in the medial compartment during gait, requiring very sharp valgus deformity for there to be overloading of the lateral compartment2, 3, 4. This adductor moment also biomechanically justifies the need for alignment at 0° of the anatomical axis on the valgus knee osteotomies, since, under physiological conditions, 60% of body weight passes through the medial compartment5, 6.
The indication of osteotomy for the treatment of gonarthrosis is becoming more restricted due to the great improvement in long-term results of total knee arthroplasty(7). However, it has the great advantage of not being a procedure of substitution, which is more relevant in young patients. The femoral osteotomy is more effective than tibial osteotomy for addressing valgus deformity of the knee, for making the transcondylar line perpendicular to the mechanical axis and minimizing the loosening of the medial collateral ligament1, 8, 9.
The aim of this study is to evaluate the long-term results of distal femoral varisation osteotomy and seek predictive criteria that can assist in the selection of patients to undergo this technique.
METHODS
From July 1997 to November 2004, 23 varisation osteotomies of the distal femur were performed by the same surgeon for the treatment of gonarthrosis, using the technique described in this article. Eight patients were excluded from the study, six of whom were not located, one of whom deceased before beginning the evaluation and one of whom did not have the clinical conditions for a functional assessment because of terminal colon cancer. The final study group therefore consisted of 15 patients who underwent varisation osteotomy of the distal femur and blade plate fixation. Of the patients, 13 had primary lateral gonarthrosis and two had post-traumatic gonarthrosis.
Patients were categorized according to age (less than 20, 20-40, 40-60, and over 60 years), duration of postoperative follow-up (less than 50, 50 to 100, and over 100 months) and postoperative anatomic angle (more than 2° of varus, from 2° of varus to 3° of valgus, and more than 3° of valgus).
The patients' ages at the time of surgery ranged from 19 to 72 years (mean 49.8). Three were male and 12 female. The postoperative follow-up ranged from 43 to 132 months (mean 81.4). Ten osteotomies were performed in the right knee and five on the left. No patient underwent bilateral osteotomy of the femur. One patient was previously submitted to valgization osteotomy of the contralateral tibia and another patient to contralateral patellar realignment.
Preoperative evaluation and indication for the procedure
In the preoperative evaluation, patients underwent a private interview and orthopedic clinical examination by the senior author, and anteroposterior (AP) standing radiographs of the knees were performed in the single leg stance, on 30×40 cm film for measuring the anatomic angle, or the femorotibial angle, respecting the same rotational position of the lower limbs from the observation of the position of the patella and feet at the time of examination(10-15) (Figure 1). Profile radiographs of the knee and axial radiographs of the patella were used to confirm the diagnosis of lateral unicompartmental osteoarthritis.
Figure 1.

Preoperative clinical and radiographic evaluation with delineation of the anatomic axis
Surgical technique
Through a lateral approach to the distal femur, supracondylar osteotomy in a 45° “V”15, 16, 17, 18 and lateral blade plate fixation were performed in all 15 patients. To obtain neutral alignment of the anatomical axis and, therefore, with 5° to 8° of varus from the mechanical axis12, 14, 15, 17, 19, 20, the blade of the 95° fixedangle plate was inserted in parallel or with an angle of up to 5° varus in relation to the tibial articular surface under radioscopic visualization. The plate was then fixed to the femur after verification of the mechanical axis by means of a wire positioned outside the center of the femoral head to the center of the ankle joint(21) (Figure 2).
Figure 2.

Surgical technique: A) medial access, guide wires to guide the placement of the blade plate, marking the osteotomy in “V”; B) osteotomy in “V” and cutting for insertion of the blade plate; C) blade plate fixed, with a view of the lateral translation of the distal fragment of the osteotomy
In the immediate postoperative period isometric and isotonic exercises were initiated with active knee flexion-extension under supervised physiotherapy. Weight bearing on the operated limb was allowed after six to eight weeks, according to clinical signs and radiographic consolidation of the osteotomy.
Long-term postoperative evaluation
For the subjective and objective long-term postoperative evaluation, patients returned to the institution for a private interview with the authors of the study, an orthopedic clinical examination, and radiographic evaluation of the operated knee (Figure 3). The standardized Knee Society Rating System (KSS) questionnaire was then applied(22), with the alignment criterion modified to suit the purposes of the study. The KSS was originally developed for the evaluation of patients undergoing knee arthroplasty aimed at mechanically aligning the knee in neutral, using the following criteria to score the alignment: final angle between 5° and 10° of valgus, no deduction made in score; between 0° and 4° or between 11° and 15° of valgus, three points are deducted for each degree; and varus angulation or greater than 15° of valgus, 20 points are deducted. In the present study, patients with a final angle between 2° of varus and 3° of valgus, no deduction was made in the score as it was considered the desired outcome for the procedure12, 16, 17, 23, 24. Three points were deducted for each degree between 3° and 7° of varus or between 4° and 8° of valgus, and 20 points for angles greater than 7° of varus or 8° of valgus.
Figure 3.

Postoperative radiographic evaluation with the desired anatomical axis delineated
AP radiographs in the orthostatic single leg stance on 30x40 cm film were used in the evaluation to measure the anatomic angle and a lateral radiograph of the knee for the assessment of the alignment in neutral of the osteotomy in the sagittal plane.
Statistical analysis
In order to evaluate the existence of statistically significant relationship between excellent/good and fair/poor results obtained by the KSS protocol with the variables patient age at the time of surgery, postoperative follow-up time, and postoperative anatomic angle, statistical analysis was performed using Fisher's exact test after categorization of the variables. We used p < 0.05 for statistical significance.
RESULTS
According to the KSS, five excellent results were obtained (above 170 points), six good (between 140 and 170 points), one fair (between 125 and 139 points) and three poor (below 125 points). The excellent and good results amounted to 73% and the fair and poor, 27% of the total (Figure 4).
Figure 4.
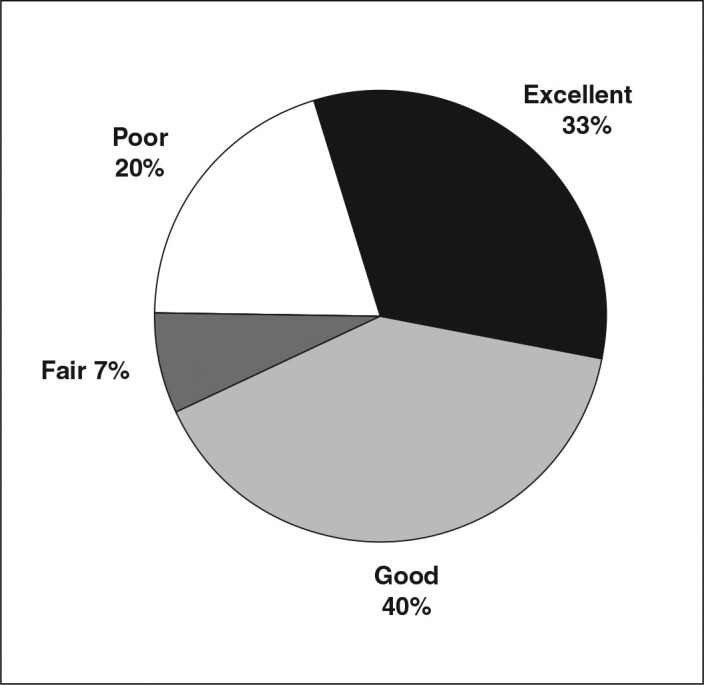
Percentage distribution of the results obtained by the Knee Society Rating System (KSS)
The final postoperative anatomical angle ranged from 11° of varus to 11° of valgus (mean 1.73° of valgus); seven patients (46%) were in the desired range of 2° of varus to 3° of valgus.
By categorizing the age into four age groups (less than 20, 20-40, 40-60, and over 60 years), there were no statistically significant differences between groups of excellent/good and fair/poor results (p = 0.73).
When considering the duration of follow-up in three periods (less than 50, 50 to 100, and more than 100 months), there were no statistically significant differences between groups of excellent/good and fair/poor results (p = 0.58).
Dividing the postoperative angle into three groups of values (more than 2° of varus, from 2° of varus to 3° of valgus, and more than 3° of valgus), there were no statistically significant differences between groups of excellent/good and fair/poor results (p = 0.50).
DISCUSSION
Distal femoral varisation osteotomy is indicated in lateral unicompartmental osteoarthritis presenting an anatomical angle greater than 12° of valgus or inclination of the articular surface of the knee greater than 10° in the coronal plane in relation to the horizontal12, 13, 15, 17, 23, 24, 25. The procedure is contraindicated in patients with nonspecific knee pain, arthritis, or previous meniscectomy in the medial compartment and inflammatory disease. Age over 60 years, obesity, severe arthritis, knee range of motion less than 90°, and moderate or severe knee ligament instability are considered relative contraindications1, 12, 13, 15. Severe patellofemoral arthritis, characterized by predominantly anterior pain and radiographic signs of osteophytes and joint clamping, was considered an absolute contraindication to femoral osteotomy, although in a recent study by Wang and Hsu(26) there was no difference in the outcome of osteotomy in eight patients with severe patellofemoral arthrosis in relation to cases of unicompartmental osteoarthritis.
The measurement of the anatomic axis on AP radiographs with the single leg stance was used because it is easier to perform and less expensive when compared with use of the measure of the mechanical axis(15), considering that, regardless of the technique for measuring the axis, there is not a precise correlation between the radiographic (static) findings and load distribution (dynamic), even after corrective osteotomy3, 4.
The results of femoral varisation osteotomy for the treatment of valgus knee in the literature are quite varied, reflecting the influence of factors such as patient selection, surgical technique, postoperative alignment, and follow-up period8, 20, 27, 28. Of these factors, the influence of postoperative alignment on the clinical course is well documented12, 16, 17, 23, 24. Although no prospective clinical studies have been conducted, alignment with a femorotibial angle of 0° is generally accepted as the desired postoperative correction(24). This study considered an axis between 2° of varus and 3° of valgus as a good alignment, based on a modification of the range of proper alignment of the KSS to suit the anatomical alignment in neutral desired after the procedure. There was no statistically significant association between the final anatomic angle and the KSS score results, although three of the four fair/poor results occurred in patients with final anatomical angles (10° of varus, 10° of valgus, and 11° of valgus) further away from the ideal range.
The number of patients in this study (n = 15) is small but comparable with the literature concerning distal femoral varisation osteotomy using a “V” technique, which in the reviewed articles ranged from 11 to 17, with an average of 13.715, 16, 17, 18.
The postoperative follow-up period in this study (81.4 months) was higher than that of most of the literature. Of 18 studies reviewed8, 10, 11, 14, 15, 16, 17, 18, 19, 23, 24, 26, 29, 32, 33, only six10, 11, 17, 26, 29, 32 had a higher average.
The age group between 19 and 72 years (mean 49.8 years) was also similar to other studies, which in the literature ranged from 14 to 79 years, averaging between 34.8 and 58 years14, 15, 16, 17, 18, 23, 27, 30, 31, 33.
A comparison of the results obtained in this study with the application of the KSS is made complicated by the wide variety of methodologies found in the literature. However, when comparing these data, it can be seen that the rate of excellent and good results (73%) was greater than in six8, 10, 11, 15, 27, 31 studies, with rates between 57.1 and 71.4%. Of the 12 studies14, 16, 17, 18, 19, 23, 24, 26, 29, 30, 32, 33 with superior results (indexes between 76.4 and 100%), only four17, 26, 29, 32 had longer follow-up. This data becomes relevant to the extent that, in the literature, deterioration of results is described over time during follow-up6, 10, 26, 30. However, Edgerton et al.(11) did not observe this trend, which is also true for this study.
Comparing the results with only the studies of “V” osteotomies, similar success rates could be observed. Aglietti et al.(15) showed 71.4% excellent and good results in a group of 14 patients after a mean follow-up of 21.8 months. In 1991, Cerqueira et al.(16) obtained 81.8% excellent and good results in 11 patients, with a mean follow-up of 42 months. Costa et al.(18) evaluated 13 patients with a mean follow-up of 24 months, and 76.9% had satisfactory results. Aglietti and Menchetti(17), after a mean follow-up period of 108 months for 17 patients, had 76.4% excellent or good results.
CONCLUSION
We conclude that the distal femoral varisation osteotomy in “V” is a good option for the treatment of patients with lateral compartment osteoarthritis and valgus knee. However, patient age on the time of surgery, follow-up period, and postoperative anatomic angle failed to be confirmed as predictive factors of the outcome.
REFERENCES
- 1.Leone JM, Hansen AD. Osteotomy about the knee: american perspective. In: Scott WN, editor. Insall & Scott surgery of the knee. 4th ed. Churchill Livingstone; New York: 2006. pp. 1301–1314. [Google Scholar]
- 2.Andriacchi TP. Dynamics of knee malalignment. Orthop Clin North Am. 1994;25(3):395–403. [PubMed] [Google Scholar]
- 3.Harrington IJ. Static and dynamic loading patterns in knee joints with deformities. J Bone Joint Surg Am. 1983;65(2):247–259. doi: 10.2106/00004623-198365020-00016. [DOI] [PubMed] [Google Scholar]
- 4.Johnson F, Leitl S, Waugh W. The distribution of load across the knee. A comparison of static and dynamic measurements. J Bone Joint Surg Br. 1980;62(3):346–349. doi: 10.1302/0301-620X.62B3.7410467. [DOI] [PubMed] [Google Scholar]
- 5.Franco V, Cerullo G, Cipolla M, Gianni E, Puddu G. Open wedge high tibial osteotomy. Techn Knee Surg. 2002;1(1):43–53. [Google Scholar]
- 6.Poilvache P. Osteotomy for the arthritic knee: a european perspective. In: Scott WN, Scott WN, editors. Surgery of the Knee. 4th ed. Churchill Livingstone; New York: 2006. pp. 1351–1358. [Google Scholar]
- 7.Crockarell JR, Jr, Guyton JL. Artroplastia de tornozelo e joelho. In: Canale ST, editor. Cirurgia ortopédica de Campbell. 10a. ed. Manole; Barueri, SP: 2006. pp. 245–251. [Google Scholar]
- 8.Mathews J, Cobb AG, Richardson S, Bentley G. Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics. 1998;21(4):437–440. doi: 10.3928/0147-7447-19980401-08. [DOI] [PubMed] [Google Scholar]
- 9.Jackson JP. Osteotomy for osteoarthritis of the knee. Proceedings of the Sheffield Regional Orthopaedic Club. J Bone Joint Surg Br. 1958;40:826. [Google Scholar]
- 10.Finkelstein JA, Gross AE, Davis A. Varus osteotomy of the distal part of the femur. A survivorship analysis. J Bone Joint Surg Am. 1996;78(9):1348–1352. doi: 10.2106/00004623-199609000-00008. [DOI] [PubMed] [Google Scholar]
- 11.Edgerton BC, Mariani EM, Morrey BF. Distal femoral varus osteotomy for painful genu valgum. A five-to-11-year follow-up study. Clin Orthop Relat Res. 1993;(288):288–289. [PubMed] [Google Scholar]
- 12.Coventry MB. Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am. 1973;55(1):23–48. [PubMed] [Google Scholar]
- 13.Coventry MB. Current concepts review: upper tibial osteotomy for osteoarthritis. J Bone Joint Surg Am. 1985;67(7):1136–1140. [PubMed] [Google Scholar]
- 14.Queiroz AAB, Navarro RD, Kubota MS. Correção da deformidade em valgo do joelho através da osteotomia cuneiforme de subtração supracondiliana do fêmur e utilização simultânea de enxerto autológo do ilíaco. Rev Bras Ortop. 1993;28(5):258–262. [Google Scholar]
- 15.Aglietti P, Stringa G, Buzzi R, Pisaneschi A, Windsor RE. Correction of valgus knee deformity with a supracondylar V osteotomy. Clin Orthop Relat Res. 1987;(217):217–220. [PubMed] [Google Scholar]
- 16.Cerqueira NB, Souza JMB, Mendes ML. Osteotomia frontal supracondiliana do fêmur em “V” no perfil. Nova técnica para tratamento da deformidade em valgo do joelho. Rev Bras Ortop. 1991;26(10):365–368. [Google Scholar]
- 17.Aglietti P, Menchetti PP. Distal femoral varus osteotomy in the valgus osteoarthritic knee. Am J Knee Surg. 2000;13(2):89–95. [PubMed] [Google Scholar]
- 18.Costa RA, Santos HRO, Meneses LC. Osteotomia supracondiliana do fêmur em “V” no tratamento da deformidade em valgo do joelho. Rev Bras Ortop. 1992;27(4):222–226. [Google Scholar]
- 19.Learmonth ID. A simple technique for varus supracondylar osteotomy in genu valgum. J Bone Joint Surg Br. 1990;72(2):235–237. doi: 10.1302/0301-620X.72B2.2312562. [DOI] [PubMed] [Google Scholar]
- 20.Maquet P. The treatment of choice in osteoarthritis of the knee. Clin Orthop Relat Res. 1985;192:108–112. [PubMed] [Google Scholar]
- 21.Dietrick TB, Bugbee WD. Distal femoral osteotomy utilizing a lateral opening-wedge technique. Techn Knee Surg. 2005;4(3):186–192. [Google Scholar]
- 22.Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989;(248):244–248. [PubMed] [Google Scholar]
- 23.Healy WL, Anglen JO, Wasilewski SA, Krackow KA. Distal femoral varus osteotomy. J Bone Joint Surg Am. 1988;70(1):102–109. [PubMed] [Google Scholar]
- 24.McDermott AG, Finklestein JA, Farine I, Boynton EL, MacIntosh DL, Gross A. Distal femoral varus osteotomy for valgus deformity of the knee. J Bone Joint Surg Am. 1988;70(1):110–116. [PubMed] [Google Scholar]
- 25.Coventry MB. Proximal tibial varus osteotomy for osteoarthritis of the lateral compartment of the knee. J Bone Joint Surg Am. 1987;69(1):32–38. [PubMed] [Google Scholar]
- 26.Wang J, Hsu C. Distal femoral varus osteotomy for osteoarthritis of the knee. Surgical technique J Bone Joint Surg Am. 2006;(88 Suppl 1):88. doi: 10.2106/JBJS.E.00827. [DOI] [PubMed] [Google Scholar]
- 27.Terry GC, Cimino PM. Distal femoral osteotomy for valgus deformity of the knee. Orthopedics. 1992;15(11):1283–1289. doi: 10.3928/0147-7447-19921101-07. [DOI] [PubMed] [Google Scholar]
- 28.Johnson E, Jr, Bodell LS. Corrective supracondylar osteotomy for painful genu valgum. Mayo Clin Proc. 1981;56(2):87–92. [PubMed] [Google Scholar]
- 29.Cameron HU, Botsford DJ, Park YS. Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg. 1997;40(2):114–118. [PMC free article] [PubMed] [Google Scholar]
- 30.Oliveira LP, Elias N, Cunha S, Mesquita KC. Osteotomia varizante distal do fêmur no tratamento do joelho valgo associado a artrose unicompartimental. Rev Bras Ortop. 1993;28(11/12):85–88. [Google Scholar]
- 31.Severino NR, Camargo OPA, Aihara T, Cury RPL, Oliveira VM, Barbi L, Medeiros SF. Osteotomia supracondiliana femoral no tratamento da deformidade em valgo do joelho. Rev Bras Ortop. 1998;33(4):282–286. [Google Scholar]
- 32.Cognet JM, Rouvillain JL, Mousselard HP. Résultat des ostéotomies fémorales de varisation pour genu valgum: a propos de 75 cas revus ´ plus de cinq ans de recul. Rev Chir Orthop Reparatrice Appar Mot. 1998;84:46. [Google Scholar]
- 33.Navarro RD, Laredo Filho J. Correção da deformidade em valgo do joelho, por via de acesso anterior, pela osteotomia de subtração supracondiliana do fêmur. Rev Bras Ortop. 1992;27(4):217–221. [Google Scholar]