

Abstract
Objective: To evaluate the prevalence of cervical spine abnormalities among patients with rheumatoid arthritis and correlate the imaging findings with the clinical state. Methods: A cross-sectional study on 35 patients was carried out at the School of Medicine of the Federal University of Goiás (UFG) in 2004. The following were evaluated: age, use of medications and the clinical picture of pain and neurological characteristics. The erythrocyte sedimentation rate (ESR) and rheumatoid factor were tested, and radiographs of the cervical spine were produced in anteroposterior, lateral and dynamic views. To evaluate the influence of the variables on the emergence of instabilities, univariate and multivariate logistic regression tests were used (p < 0.05). Results: Among the 35 patients evaluated, 13 (37.1%) presented a stable cervical spine. Out of the 22 patients with instability, six presented more than one type. Atlantoaxial instability was found in 15 patients, with a mean anterior atlantodental distance of 3.40 mm in the neutral lateral radiographic view and 6.54 mm in the lateral view with flexion. Basilar invagination was found in five patients and subaxial subluxation in seven patients. Two thirds of the asymptomatic patients had instabilities. Bicipital hyperreflexia presented statistically significant correlations with atlantoaxial instability (p = 0.024) and subaxial instability (p = 0.01). Age at diagnosis correlated with subaxial instability (p = 0.02). Conclusions: The prevalence of cervical instability was 62.9 % (22/35). The most frequent instabilities were: atlantoaxial subluxation (42.9 %), subaxial subluxation (20%) and basilar invagination (14.3%). The correlation between instabilities and clinical signs and symptoms was poor. The patients with subaxial subluxation presented disease onset at a younger age. Dynamic radiography was important for diagnosing atlantoaxial subluxation.
Keywords: Spine, Cervical vertebrae, Rheumatoid arthritis
INTRODUCTION
Rheumatoid arthritis is a chronic systemic inflammatory disease of unknown cause that mainly affects the synovial membrane of many joints1, 2. Its prevalence in Brazilian populations ranges from 0.2 to 1%(3).
Although it may affect the entire vertebral axis, its main involvement is in the cervical spine and especially at the craniocervical junction, which can be explained by the fact that the occipital-C1 and C1-C2 joints are purely synovial4, 5.
The various studies available show that 5% to 73% of the patients with rheumatoid arthritis will develop atlantoaxial subluxation between two and ten years after receiving their diagnosis. Of these, 20% will present significant abnormalities in the subaxial cervical spine. Around 17% of all patients with rheumatoid arthritis will develop neurological signs and symptoms (ranging from 5 to 67%) and, among those who develop myelopathy, half of them will only survive for one year6, 7, 8, 9.
There are several reports on the prevalence of cervical lesions and rheumatoid arthritis in European and North American populations, but the extent of this problem remains little known within the Brazilian setting.
The aims of this study were to evaluate the prevalence of abnormalities of the cervical spine among patients with rheumatoid arthritis and to establish which types are most frequent, with correlations between imaging findings and the clinical picture.
METHODS
This study was approved in July 2003 by the Ethics Committee for Human and Animal Research of Hospital das Clinicas, Federal University of Goiás (UFG). All the patients were evaluated and included in the study after they had signed an informed consent statement.
A cross-sectional investigation was then carried out in 2004, with a sample obtained from among patients at the outpatient clinic of the Rheumatology Service of the Department of Clinical Medicine, School of Medicine, UFG. Cases of rheumatoid arthritis were diagnosed in accordance with the criteria of the American College of Rheumatology (ACR), and patients were included in this study consecutively as they were attended.
Patients were excluded from the study if they started to present the disease before reaching 18 years of age; if they had a history of trauma to the cervical spine; if they had previously undergone surgery on the cervical spine; if they did not accept the informed consent statement; if they abandoned the study; or if they did not undergo the examinations that they were asked to have.
The following variables were evaluated: age at diagnosis, duration of the disease, use of and duration of use of corticoids, use of disease-modifying antirheumatic drugs (DMARDs) and neurological state.
The presence of occipital headache, cervicalgia or paresthesia, and the subjective assessment of strength, were evaluated and correlated with the presence of cervical instability. The presence of abnormal reflexes, presence of Babinsky and L'Hermitté signs and presence of clonus were evaluated in the physical examination. Objective evaluation of strength was excluded because of interference from the disease activity, which made interpretation difficult. The classification of Ranawat et al(10) was used to objectively assess the painful symptoms and neurological involvement (Boxes 1 and 2).
Box 1.
Ranawat pain classification
| CLASS | |
|---|---|
| 0 | Free from pain |
| I | Intermittent pain, responsive to ordinary analgesics |
| II | Intermittent pain, responsive ordinary analgesics, with need for immobilization using a cervical collar |
| III | Continuous and incapacitating pain that does not respond to analgesics |
Adapted from Ranawat et al(10)
Box 2.
Ranawat classification for neurological involvement
| CLASS | Neurological abnormality |
|---|---|
| I | No neurological abnormalities |
| II | Subjective weakness, hyperreflexia, dysesthesia |
| III | Objective weakness, long tract signs A – Able to walk B – Unable to walk, quadriparetic |
Adapted from Ranawat et al(10)
The erythrocyte sedimentation rate (ESR) and rheumatoid factor were tested in the laboratory.
The imaging examinations consisted of simple radiography of the spine, using the anteroposterior and lateral views. The latter was performed in neutral position and dynamic (flexion and extension) positions. The tube-film distance was standardized as 1.50 m.
Atlantoaxial instability was diagnosed when the anterior atlantodental distance was greater than 3 mm, as measured between the anterior arch of the atlas and the odontoid process. Basilar invagination (upwards migration of the odontoid) was evaluated using the methods of Ranawat et al(10) (the normal value was taken to be 15 mm or more for men and 13 mm or more for women) (Figure 1) and the methods of Redlund-Johnell and Pettersson(11) (the normal value was taken to be 34 mm or more for men and 29 mm or more for women) (Figure 2). It was diagnosed when it was found to be positive using either of these two criteria. Subaxial subluxation was diagnosed when there was slippage of more than 3.5 mm.
Figure 1.
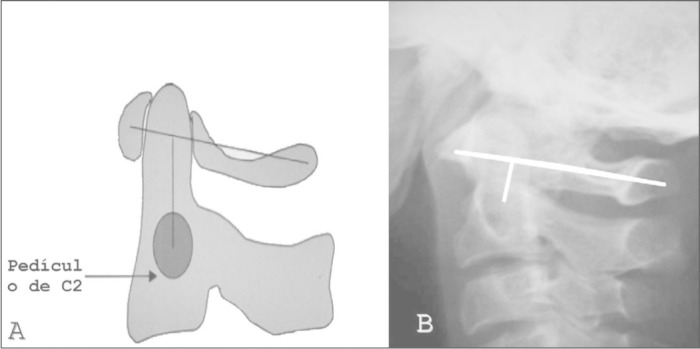
A) Illustration demonstrating Ranawat's method (measurement of the distance between the center of the pedicle of C2 and the transverse line on the C1 arch), as modified by Riew et al(12) (reproduced with permission from the Journal of Bone and Joint Surgery, Inc.). B) Lateral radiograph of the spine, demonstrating how the Ranawat index was measured.
Figure 2.
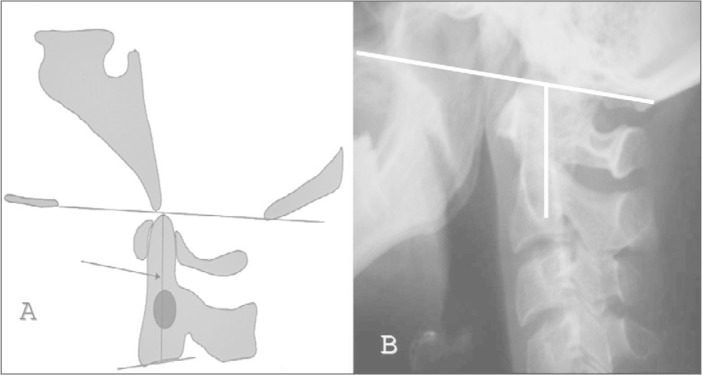
A) Illustration demonstrating Redlund-Johnell's method (measurement of the distance between McGregor's line and the midpoint of the lower margin of C2), as modified by Riew et al(12) (reproduced with permission from the Journal of Bone and Joint Surgery, Inc.). B) Lateral radiograph of the spine, demonstrating how the Redlund-Johnell index was measured.
The patients were asked whether they had previously undergone radiography on the spine and whether the physician attending them had informed them that they presented spinal abnormalities.
The Microsoft® Excel 2000 software was used to tabulate the data, and the statistical analysis was performed using the SPSS® software (Statistical Package for the Social Sciences) for Windows®, version 11.5. To evaluate the influence of the variables on the emergence of instabilities, univariate and multivariate logistic regression tests were used. The significance level was taken to be values less than 0.05 (p < 0.05).
RESULTS
Among the 35 patients evaluated, there were 31 women (88.6%) and four men (11.4%), with a mean age of 51.6 years (ranging from 32 to 68 years). The mean age at which rheumatoid arthritis was diagnosed was 36.6 years (ranging from 20 to 62 years). The patients had had the disease for a mean of 15 years (ranging from 4 to 33 years).
One patient was not using any medication.
With regard to corticoid use, only one patient was not doing so, while the other 34 patients had been using corticoids for a mean of 11.8 years (ranging from 5 to 32 years).
Two patients were not using disease-modifying antirheumatic drugs (DMARDs). Twenty-nine patients were using only one DMARD, while nine were using a double regimen and one was using a triple regimen.
Twenty-six patients had at least one of the clinical manifestations under evaluation: 14 patients with occipital headache, 19 with cervicalgia, 12 with paresthesia and nine with subjective loss of strength. Among the nine patients who did not have any complaints of headache, cervicalgia, paresthesia and loss of strength, or any complaints of pain in the Ranawat classification (class 0), six presented cervical instability (three cases of atlantoaxial subluxation, two of subaxial subluxation and one of atlantoaxial subluxation in association with basilar invagination) (Figure 3).
Figure 3.
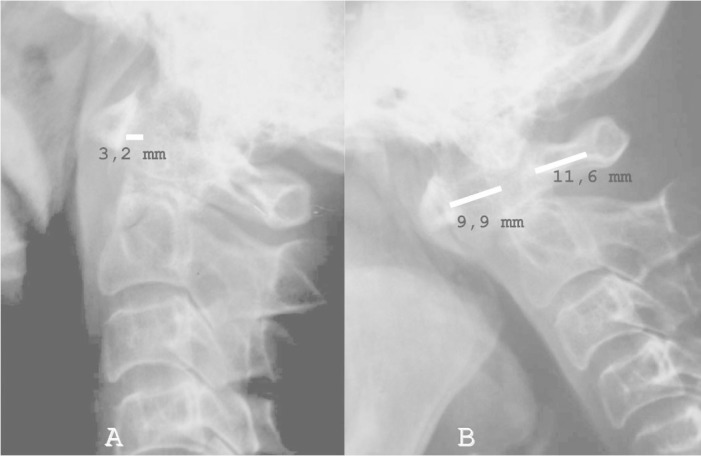
53-year-old female patient with the disease for the past 33 years. She did not present any complaint and, on Ranawat's scale, she was grade 0. Lateral radiograph showing anterior atlantoaxial distance of 3.2 mm, viewed in the neutral position (A) and anterior atlantoaxial distance of 9.9 mm, viewed laterally, in flexion (B). A posterior atlantoaxial distance of 11.6 mm can also been seen on the radiograph in flexion: this is a sign of high risk of irreversible paralysis.
Eleven patients did not present any abnormalities of reflexes. Two patients were positive for Babinsky's sign, four were positive for L'Hermitté's sign and two presented clonus.
The pain presented by the patients was classified as follows on the Ranawat scale: 13 in class 0, 20 in class I and two in class III. The functional evaluation showed that there were 24 cases in class I, nine cases in class II and two cases in class III-A.
The erythrocyte sedimentation rate (ESR) was high in 16 patients, with a mean of 52.5 mm/h. Twenty-seven patients were positive for rheumatoid factor.
Only two patients had previously undergone radiography on the spine. One of them presented atlantoaxial instability and did not know about it, while the other was aware of having a spinal abnormality but did not know which one it was.
Among the patients evaluated, 13 (37.1%) presented spinal stability. Among the 22 patients (62.9%) with a radiographic picture of instability, six had more than one type of instability (one case of invagination and subaxial subluxation, two cases of invagination and atlantoaxial subluxation and three cases of atlantoaxial subluxation and subaxial subluxation).
Atlantoaxial instability was found in 15 patients (42.9%), with a mean anterior atlantodental distance of 3.4 mm (ranging from 1.5 to 9.4 mm) on lateral radiographs in neutral position and 6.5 mm (ranging from 3.1 to 10.1 mm) on lateral radiographs in flexion. Among these 15 patients, the anterior atlantodental distance was normal on lateral radiographs in neutral position. Measurements of the posterior atlantodental distance showed that two patients presented an interval of less than 14 mm.
Basilar invagination was found in five patients (14.3%), among whom four were diagnosed using the Ranawat method, three were diagnosed using the Redlund-Johnell method and two were diagnosed using both methods.
Subaxial subluxation was observed in seven patients (20%).
The statistical analysis demonstrated significant correlations between the following variables: bicipital hyperreflexia and atlantoaxial instability (p = 0.024); bicipital hyperreflexia and subaxial instability (p = 0.01); and age at diagnosis and subaxial instability (p = 0.02). The mean age at diagnosis among the patients with subaxial instability was 34.9 years (± 10), while the mean age of the patients without subaxial instability was 42.5 years (± 12.7). There was no significant correlation between the other variables and the different types of instability (atlantoaxial subluxation, basilar invagination and subaxial subluxation).
DISCUSSION
Studies on the involvement of the cervical spine in patients with rheumatoid arthritis have not been prominent within the Brazilian setting. Systematic periodic evaluation of the cervical spine among patients with rheumatoid arthritis should be performed routinely in rheumatology and orthopedics services, but it is not even done preoperatively for a significant proportion of the patients(13).
Despite the advances due to new types of imaging examinations (computed tomography and magnetic resonance), investigations using simple radiography form the ideal method for screening for instabilities of the cervical spine because of their low cost (less than 10% of the cost of magnetic resonance) and easy access (practically universal availability in clinics and hospital, even in those of small size)14, 15, 16, 17, 18.
In our sample, we did not find any statistical correlation between the use of DMARDs and the development of cervical abnormalities, but it is important to emphasize that the study model used (cross-sectional) had a major influence on this finding, given that this methodology is not ideal for making this specific investigation.
The prevalence of instability found in our series (62.9%) was within the range reported in the literature1, 15, 17, 18, 19, 20, 21, 22.
Atlantoaxial subluxation is the type of instability that most frequently affects the cervical spine of patients with rheumatoid arthritis14, 18, 19, 21, 23, 24. The anterior atlantodental distance measurement is the reference for diagnosing anterior atlantoaxial subluxation, although Boden et al(21) observed in a study on factors predicting paralysis that the posterior atlantodental distance is the main parameter to be evaluated. In their study, they observed that patients with a posterior atlantodental distance smaller than 10 mm did not achieve neurological recovery through surgical treatment, and that when there was an association with basilar invagination, the minimum posterior atlantodental distance should be 13 mm, for there to be neurological recovery. However, all the patients with paralysis and a posterior atlantodental distance of at least 14 mm achieved complete neurological recovery. The authors concluded that surgical treatment, whether in cases of neurological deficit or not, was indicated for all patients with atlantoaxial subluxation and a posterior atlantodental distance of 14 mm or less. This approach was reinforced by the study by Zeidman and Ducker(7) who, in studying the craniocervical junction, observed that the minimum space for the neural structures was 13 to 14 mm. In our sample, two of the 15 patients with atlantoaxial subluxation presented a posterior atlantodental distance smaller than 14 mm on the radiograph in flexion, and one of these cases was asymptomatic (Figure 4).
Figure 4.
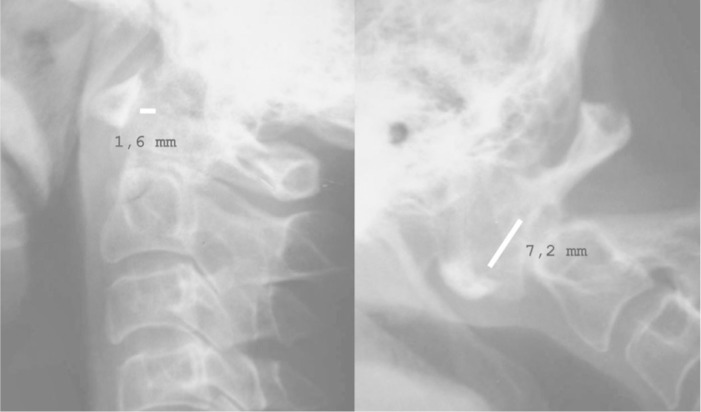
Case demonstrating the importance of producing dynamic radiographs. Lateral radiographic views showing a normal anterior atlantodental distance in the neutral position (1.6 mm) and a significant increase in the anterior atlantodental distance in the flexed position (7.2 mm)
One point to be emphasized in studying atlantoaxial instability is the use of dynamic radiographs. We observed in our study that 60% (9/15) of the patients with atlantoaxial subluxation presented a normal anterior atlantodental distance (less than 3 mm) on the lateral radiograph in neutral position (Figure 4). Kwek et al(13) demonstrated that the difference in the detection rate for instabilities of the cervical spine between radiographic views in a stressed position (dynamic) and non-stressed position (neutral) was statistically significant (p < 0.05). Basilar invagination may be difficult to diagnose on simple radiographs, to such an extent that several techniques for diagnosing it exist. Riew et al(12) conducted a study to evaluate the radiographic criteria that are most accepted for diagnosing basilar invagination among patients with rheumatoid arthritis (Clark's stages, Chamberlain's line, McRae's line, McGregor's line, Redlund-Johnell's criterion, Ranawat's criterion, Fischgold-Metzger's line and Wackenheim's line). The study demonstrated that no test alone had sensitivity or negative predictive value greater than 90%. These authors suggested that a combination of tests should be used (Clark's stages, Redlund-Johnell's criterion and Ranawat's criterion), in order to attain higher sensitivity and negative predictive value, and that if any of these tests were to suggest the presence of basilar invagination, computed tomography or magnetic resonance examinations should be performed. Even with a combined approach, the authors reported that around 6% of the basilar invagination would pass by unnoticed, and they concluded that whenever there was any diagnostic doubt based on simple radiograph examinations, computed tomography or magnetic resonance examinations should be performed. In our study, we chose to use the methods of Redlund-Johnell and Ranawat, and this standard was also used by Souza and Defino(20). These authors found prevalences of basilar invagination of 11% and 13.5% among their patients, using the criteria of Ranawat and Redlund-Johnell respectively, but they did not comment on the simultaneous findings. The advantage of these techniques is that the diagnosis is made independent of viewing the tip of the odontoid, which is difficult to see in rheumatic patients because of osteoporosis. Riew et al(12) were able to identify the tip of the odontoid in only 34% of their cases and, for this reason, they did not recommend the use of techniques for direct measurement of the migration of the odontoid (McRae's, Chamberlain's and McGregor's lines). This opinion has also been shared by other authors9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24. We observed a prevalence of basilar invagination of 14.3% (five patients) in our group of patients, with diagnoses using Ranawat's method in four cases and using Redlund-Johnell's method in three cases, and simultaneous diagnosis using both methods in two cases.
Involvement of the subaxial cervical spine occurs in 7 to 29% of patients with rheumatoid arthritis8, 25, and this considered to be the second most frequently occurring type of cervical subluxation9, 18, 24. In our sample, we found subaxial subluxation in 20% of our patients, and this was the second most frequent instability. The patients with subaxial subluxation started to present rheumatoid arthritis at a younger age, which was a statistically significant difference (34.8 years versus 42.5 years; p = 0.02). According to Bouchard-Chabot and Lioté(8), the subaxial cervical spine is more affected among older patients, but they did not make any comments regarding the onset of rheumatoid arthritis at younger ages. The mean age among the group of patients with subaxial subluxation in our sample was 56.1 years (ranging from 43 to 68 year), while the mean age among the patients without subaxial subluxation was 50.5 years (ranging from 32 to 65 years), which was a difference without statistical significance.
Castro et al(19) evaluated 50 patients with a diagnosis of rheumatoid arthritis and observed that the correlation between the neurological clinical signs and the severity of the radiographic findings was low. Souza and Defino(20) concluded that there was no statistically significant correlation between cervical instabilities and complaints of cervicalgia or signs of neurological compression, and they commented that this is a fact of great practical value, since it shows that even in the absence of symptoms, the cervical spine should be investigated. In our series, we observed that 66% (6/9) of the patients who did not have any complaints presented instabilities of the cervical spine. Moreover, one of these patients had a posterior atlantodental distance of less than 14 mm (11.65 mm) (Figure 3), which would be an absolute indication for investigation using magnetic resonance,(18) in order to evaluate a likely indication for surgical treatment because of the risk of irreversible paralysis(21). In the present sample, it could be seen that there was a lack of correlation between instabilities of the cervical spine and clinical signs and symptoms.
Kauppi et al(26) carried out a study to evaluate risk factors for anterior atlantoaxial subluxation and concluded that the erythrocyte sedimentation rate did not have any correlation with the development of the instability. According to these authors, the rapid relative changes in inflammatory parameters were not reflected in the slowly progressive changes that occur in the rheumatic cervical spine.
Positive findings of rheumatoid factor (seropositivity) have been implicated as a risk factor for cervical involvement5, 15, 17. Paimela et al(27) observed that patients with cervical involvement were more frequently positive for rheumatoid factor than were patients with a normal cervical spine (85% versus 57%; p < 0.05).
In the laboratory evaluation on our patients, no statistical correlation was found between the instabilities and positive findings of VHS or rheumatoid factor.
The prevalence of instabilities of the cervical spine found in our patients reflects the data in the worldwide literature. The high frequency of instabilities in asymptomatic patients reinforces the need for routine investigation of the cervical spine in patients with rheumatoid arthritis. The possibility of severe and even fatal neurological complications should serve as a warning to medical teams involved in treating patients with rheumatoid arthritis, so that they maintain a high level of alertness regarding involvement of the cervical spine.
CONCLUSIONS
The prevalence of cervical instability in the present sample was 62.9 % (22/35).
The most frequent instabilities, in decreasing order, were: atlantoaxial subluxation, affecting 42.9% (15/35); subaxial subluxation, affecting 20% (7/35); and basilar invagination, affecting 14.3% (5/35).
The correlation between the instabilities of the cervical spine and the clinical signs and symptoms was poor. Only bicipital hyperreflexia showed a significant correlation with atlantoaxial subluxation (p = 0.024) and subaxial instability (p = 0.01). Among the asymptomatic patients, 66% presented cervical instabilities.
The patients with subaxial subluxation started to present rheumatoid arthritis at a younger age (34.8 years versus 42.5 years; p = 0.02).
Dynamic radiography was important for diagnosing atlantoaxial instability, since 60% (9/15) of the patients with atlantoaxial subluxation presented a normal anterior atlantodental distance (< 3 mm) on the lateral radiographic view in the neutral position.
Footnotes
Work performed in the Rheumatology Service and Spinal Surgery Service, School of Medicine, Federal University of Goiás (UFG).
REFERENCES
- 1.Alberstone CD, Benzel EC. Cervical spine complications in rheumatoid arthritis patients. Awareness is the key to averting serious consequences. Postgrad Med. 2000;107(1):199–200, 205-8. doi: 10.3810/pgm.2000.01.833. [DOI] [PubMed] [Google Scholar]
- 2.Hellmann DB, Stone JH. Arthritis & musculoskeletal disorders. In: Tierney LM Jr, McPhee SJ, Papadakis MA, editors. Current medical diagnosis & treatment 2000. 39th ed. Lange Medical Books; New York: 2000. pp. 826–833. [Google Scholar]
- 3.Marques Neto JF, Gonçalves NT, Langen LFOB, Cunha MFL, Radominski S, Oliveira SM. Estudo multicentrico da prevalencia da AR no adulto em amostras da população brasileira. Rev Bras Reumatol. 1993;33:169–173. [Google Scholar]
- 4.Crockard HA. Surgical management of cervical rheumatoid problems. Spine (Phila Pa 1976) 1995;20(23):2584–2590. doi: 10.1097/00007632-199512000-00022. [DOI] [PubMed] [Google Scholar]
- 5.Reiter MF, Boden SD. Inflammatory disorders of the cervical spine. Spine (Phila Pa 1976) 1998;23(24):2755–2766. doi: 10.1097/00007632-199812150-00017. [DOI] [PubMed] [Google Scholar]
- 6.Casey AT, Crockard HA, Pringle J, O'Brien MF, Stevens JM. Rheumatoid arthritis of the cervical spine: current techniques for management. Orthop Clin North Am. 2002;33(2):291–309. doi: 10.1016/s0030-5898(01)00009-8. [DOI] [PubMed] [Google Scholar]
- 7.Zeidman SM, Ducker TB. Rheumatoid arthritis. Neuroanatomy, compression, and grading of deficits. Spine (Phila Pa 1976) 1994;19(20):2259–2266. doi: 10.1097/00007632-199410150-00003. [DOI] [PubMed] [Google Scholar]
- 8.Bouchaud-Chabot A, Lioté F. Cervical spine involvement in rheumatoid arthritis. A review. Joint Bone Spine. 2002;69(2):141–154. doi: 10.1016/s1297-319x(02)00361-5. [DOI] [PubMed] [Google Scholar]
- 9.Gurley JP, Bell GR. The surgical management of patients with rheumatoid cervical spine disease. Rheum Dis Clin North Am. 1997;23(2):317–332. doi: 10.1016/s0889-857x(05)70332-x. [DOI] [PubMed] [Google Scholar]
- 10.Ranawat CS, O'Leary P, Pellicci P, Tsairis P, Marchisello P, Dorr L. Cervical spine fusion in rheumatoid arthritis. J Bone Joint Surg Am. 1979;61(7):1003–1010. [PubMed] [Google Scholar]
- 11.Redlund-Johnell I, Pettersson H. Radiographic measurements of the craniovertebral region. Designed for evaluation of abnormalities in rheumatoid arthritis. Acta Radiol Diagn (Stockh) 1984;25(1):23–28. doi: 10.1177/028418518402500105. [DOI] [PubMed] [Google Scholar]
- 12.Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001;83(2):194–200. doi: 10.2106/00004623-200102000-00006. [DOI] [PubMed] [Google Scholar]
- 13.Kwek TK, Lew TW, Thoo FL. The role of preoperative cervical spine X-rays in rheumatoid arthritis. Anaesth Intensive Care. 1998;26(6):636–641. doi: 10.1177/0310057X9802600604. [DOI] [PubMed] [Google Scholar]
- 14.Chang DJ, Paget SA. Neurologic complications of rheumatoid arthritis. Rheum Dis Clin North Am. 1993;19(4):955–973. [PubMed] [Google Scholar]
- 15.Kramer J, Jolesz F, Kleefield J. Rheumatoid arthritis of the cervical spine. Rheum Dis Clin North Am. 1991;17(3):757–772. [PubMed] [Google Scholar]
- 16.Boden SD. Rheumatoid arthritis of the cervical spine. Surgical decision making based on predictors of paralysis and recovery. Spine (Phila Pa 1976) 1994;19(20):2275–2280. doi: 10.1097/00007632-199410150-00005. [DOI] [PubMed] [Google Scholar]
- 17.Rawlins BA, Girardi FP, Boachie-Adjei O. Rheumatoid arthritis of the cervical spine. Rheum Dis Clin North Am. 1998;24(1):55–65. doi: 10.1016/s0889-857x(05)70377-x. [DOI] [PubMed] [Google Scholar]
- 18.Dreyer SJ, Boden SD. Natural history of rheumatoid arthritis of the cervical spine. Clin Orthop Relat Res. 1999;(366):366–406. doi: 10.1097/00003086-199909000-00013. [DOI] [PubMed] [Google Scholar]
- 19.Castro S, Verstraete K, Mielants H, Vanderstraeten G, de Reuck J, Veys EM. Cervical spine involvement in rheumatoid arthritis: a clinical, neurological and radiological evaluation. Clin Exp Rheumatol. 1994;12(4):369–374. [PubMed] [Google Scholar]
- 20.Souza CP, Defino HLA. Estudo radiográfico das alteraçes da coluna cervical na artrite reumatoide e sua associação com sinais e sintomas da doença. Acta Ortop Bras. 2005;13(1):38–41. [Google Scholar]
- 21.Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993;75(9):1282–1297. doi: 10.2106/00004623-199309000-00004. [DOI] [PubMed] [Google Scholar]
- 22.Collins DN, Barnes CL, FitzRandolph RL. Cervical spine instability in rheumatoid patients having total hip or knee arthroplasty. Clin Orthop Relat Res. 1991;(272):272–285. [PubMed] [Google Scholar]
- 23.Kauppi M, Konttinen YT, Honkanen V, Sakaguchi M, Hamalainen M, Santavirta S. A multivariate analysis of risk factors for anterior atlantoaxial subluxation and an evaluation of the effect of glucocorticoid treatment on the upper rheumatoid cervical spine. Clin Rheumatol. 1991;10(4):413–418. doi: 10.1007/BF02206662. [DOI] [PubMed] [Google Scholar]
- 24.Roche CJ, Eyes BE, Whitehouse GH. The rheumatoid cervical spine: signs of instability on plain cervical radiographs. Clin Radiol. 2002;57(4):241–249. doi: 10.1053/crad.2001.0745. [DOI] [PubMed] [Google Scholar]
- 25.Oostveen JC, van de Laar MA, Geelen JA, de Graaff R. Successful conservative treatment of rheumatoid subaxial subluxation resulting in improvement of myelopathy, reduction of subluxation, and stabilisation of the cervical spine. A report of two cases. Ann Rheum Dis. 1999;58(2):126–129. doi: 10.1136/ard.58.2.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kauppi M, Hakala M. Prevalence of cervical spine subluxations and dislocations in a community-based rheumatoid arthritis population. Scand J Rheumatol. 1994;23(3):133–136. doi: 10.3109/03009749409103045. [DOI] [PubMed] [Google Scholar]
- 27.Paimela L, Laasonen L, Kankaanpää E, Leirisalo-Repo M. Progression of cervical spine changes in patients with early rheumatoid arthritis. J Rheumatol. 1997;24(7):1280–1284. [PubMed] [Google Scholar]