

Abstract
To report the frequencies of congenital hand diseases in patients who underwent surgery on a collective mobilization basis at SOS Hand, Recife, Pernambuco, between 2005 and 2009. Methods: Information was collected from 833 children and adolescents who were examined in eight missions. Results: Among the patients, 306 (36.7%) underwent surgery: 240 (78.4%) because of congenital malformation and 66 (21.6%) because of acquired lesions. The most frequent congenital malformations were: syndactyly, 72 cases (30.0%); polydactyly, 30 cases (12.5%); bifid thumb, 19 cases (7.9%); complex hand malformation, 14 cases (5.8%); cleft hand, 13 cases (5.4%); trigger finger, 12 cases (5.0%); camptodactyly, 11 cases (4.6%); and brachysyndactyly, 9 cases (3.7%). The most frequently acquired injuries were: obstetric traumatic lesions, 26 cases (39.4%); hand trauma sequelae, 18 cases (27.3%); cerebral paralysis sequelae, 7 cases (10.6%); electric shock sequelae, 5 cases (7.6%); and burn sequelae, 4 cases (6.1%). Conclusion: The nosology of hand diseases is similar to that of large series of elective surgery, especially regarding congenital deformities. The frequency of acquired hand lesions seems to be higher than the frequency in international series. The collective mobilization system for hand surgery is important for decreasing the need for this activity in public institutions, and it has been shown to be very efficient. The success of the project may provide support for the Brazilian National Health System to enroll hand surgeons in the on-call system, in emergency units.
Keywords: Hand Deformities, congenital; Child; Adolescent
INTRODUCTION
Although robust epidemiological data as seen in India(1) is not available in Brazil, it has been observed that declines in the rates infectious, parasitic and malnutrition-related diseases have been occurring. On the other hand, there have been relative increases in the rates of non-communicable diseases, non-transmissible chronic diseases and diseases of a genetic nature. One of these sets of illnesses consists of congenital malformations.
The cardiocirculatory system is the most frequent location for congenital malformations and the second most frequent location is the musculoskeletal system(2). The incidence of congenital malformations in the United States is between 2% and 3% of live births3, 4, and these malformations may be located in different organs and systems.
In Brazil, congenital malformations are in second place among the causes of child mortality and in third place among mortality among children under the age of five years, and are responsible for 10.5% of these cases. Between 1995 and 1997, death due to malformations exceeded death due to diarrhea and respiratory infections. In 1997, cardiovascular abnormalities were responsible for 39.4% of the deaths due to malformations and abnormalities of the central nervous system accounted for 18.8%(5). In Pernambuco, between 1993 and 2003, there were increases in the coefficients of mortality at early neonatal, perinatal, neonatal and under-one-year ages, due to congenital malformations(6).
Although congenital malformations of the hand do not contribute towards child mortality, they may have an important effect on the functional capacity, psychological state and quality of life of young individuals. Few studies in Brazil have focused on the frequency and management of such malformations7, 8, 9, 10. In addition, few Brazilian papers, particularly from surgeons specializing in hand surgery, have been published in the international literature11, 12, 13.
In several countries, there has been abundant scientific production on the epidemiological, clinical and management features of diseases of the hand14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37. Even the issues involved in the genesis of these abnormalities have started to be revealed(34).
Children frequently use their hands to explore the environment surrounding them, with consequent risks of trauma or injury. Thus, accidents involving hands occur frequently, and thermal lesions are the commonest acquired condition. Obstetric trauma is also a common condition, and this may lead to paralysis of the brachial plexus38, 39, 39, 40, 41, 42, 43, 44, 45, 46.
The reorganization of public healthcare actions in Brazil that started from the creation of the National Health System (SUS) in 1988 has been strengthening the role of tertiary care hospitals. Nonetheless, the scarcity of provision of hospital care at secondary level has contributed towards the growth of waiting lists for surgical treatment for a variety of conditions of medium therapeutic complexity, among which hand surgery is included. Collective mobilization actions with the aim of carrying out operations on hand disease cases that require surgical treatment and thereby reducing the waiting lists in public hospitals are rare. Few institutions conduct such actions, and SOS Hand in Recife, State of Pernambuco, is one of them. Thus, the aim of the present study was to report on the nosology of hand diseases encountered in collective mobilization actions carried out in this institution, which is a reference point in this State.
METHODS
A retrospective observational case series study was conducted, involving young patients who underwent hand operations in eight collective mobilization actions at SOS Hand, in Recife, between 2005 and 2009.
The data were gathered from the electronic medical files that were made available by the institution's medical archives service.
The data analyzed were the name, origin, sex, age, weight and diagnosis.
For the general analysis, all the patients examined for whom management consisting of expectant procedures, physiotherapy and surgery was indicated were included.
The data were input into Excel spreadsheets and were expressed in terms of absolute and relative frequencies.
The data gathering received prior authorization from the institution's director, and the data were used only for scientific publication.
RESULTS
During the study period, in the eight collective mobilization actions, 833 patients were examined. Among these, the diagnoses of 306 patients (36.7%) were confirmed and these individuals underwent operations. Nevertheless, for 91 patients (10.9%), although surgery was indicated, it was not carried out for a variety of reasons, including: non-acceptance by the parents; expectation that good functional results would not obtained; and presence of diseases that resulted in suspension of the surgery.
Among the patients operated, 161 (52.6%) were male and 145 (47.4%) were female. The ages of the patients operated ranged from six months to 25 years and seven months, with a mean age of seven years.
Regarding the patients' origins, the largest proportion 333/833 (40.0%) came from Recife, while 275/833 (33.0%) came from the surrounding metropolitan area (Figure 1).
Figure 1.
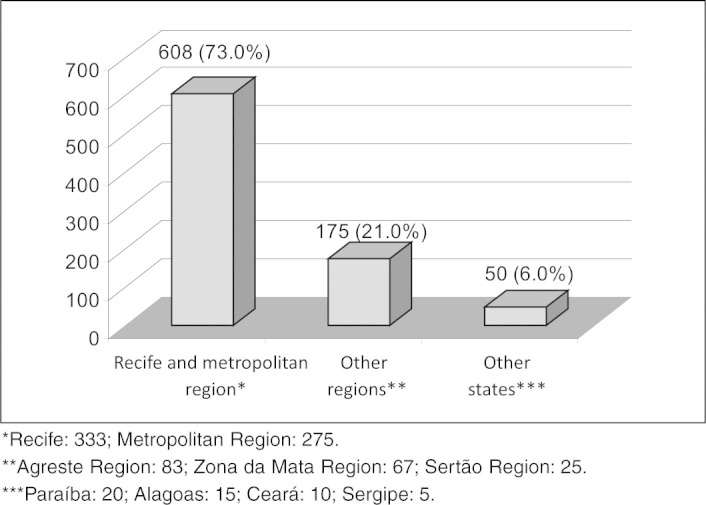
Absolute and relative frequencies of regions of origin of the patients attended during the eight collective mobilizations at SOS Hand, in Recife.
For 436 patients, there was no surgical indication at the time of the collective mobilizations; most of them were undergoing physiotherapy.
There were 240 cases of congenital malformation of the hand (78.4%). These cases resulted from abnormalities of embryonic development, and such conditions were the ones most commonly diagnosed and operated. The most frequent of these are described in order of prevalence in Table 1.
Table 1.
Distribution of frequencies of congenital malformations of the hand.
| Congenital malformations of the hand | N | % |
|---|---|---|
| Syndactyly* | 72 | 30.0 |
| Polydactyly | 30 | 12.5 |
| Bifid thumb | 19 | 7.9 |
| Complex malformation of the hand | 14 | 5.8 |
| Cleft hand | 13 | 5.4 |
| Trigger finger | 12 | 5.0 |
| Camptodactyly | 11 | 4.6 |
| Brachysyndactyly | 9 | 3.7 |
Simple syndactyly: 59/72 (81.9%); complex syndactyly: 8/72 (11.1%); and syndactyly associated with other malformations 5/72(6.9).
Other congenital malformations of the hand were: hemangioma of the hand, 8/240 cases (3.3%); arthrogryposis, 7/240 cases (2.9%); absence or deficiency of the thumb extensor, 6/240 cases (2.5%); lesion due to amniotic constriction bands on the fingers, 6/240 cases (2.5%); agenesis of the thumb, 5/240 cases (2.1%); triphalangism, 4/240 cases (1.7%); clinodactyly, 4/240 cases (1.7%); macrodactyly, 3/240 cases (1.2%); radioulnar synostosis, 3/240 cases (1.2%); ectodermal dysplasia with aplasia of the forearm, 3/240 cases (1.2%); aplasia of the forearm, 3/240 cases (1.2%); adductus thumb, 2/240 cases (0.8%); malformation of the thumb, 2/240 cases (0.8%); and one case (1/240; 0.4%) of each of the following conditions: finger hypoplasia, finger aplasia, Alpert syndrome and Polland syndrome.
The frequencies of the acquired conditions of the hand (66/306; 21.6%) are shown in Table 2.
Table 2.
Distribution of the frequencies of the acquired hand conditions.
| Acquired hand conditions | N | % |
|---|---|---|
| Lesions due to obstetric trauma | 26 | 39.4 |
| Sequelae from hand trauma | 18 | 27.3 |
| Sequelae from cerebral palsy | 7 | 10.6 |
| Sequelae from electric shock | 5 | 7.6 |
| Sequelae from burns | 4 | 6.1 |
Other acquired lesions were: sequelae from cerebral abscess, 2/66 cases (3.0%); scar neuroma, 2/66 cases (3.0%); acquired syndactyly, 1/66 case (1.5%); and claw hand due to leprosy, 1/66 case (1.5%).
DISCUSSION
Collective mobilization for hand surgery
The human hand has specialized mechanisms that enable unique activities. It has great complexity of functions. This high specificity of functions makes it very sensitive to error during the process of embryogenesis, which frequently results in congenital abnormalities(34). These need to be repaired without much delay, so that children do not develop within environments that tend to marginalize them.
The fact that there are waiting lists for surgical treatment on children at tertiary-level university reference hospitals, because of high demand for beds in these hospitals for treating high-complexity conditions, is a stimulus towards adopting new programs for surgical care. Surgery performed on an outpatient basis is one of the strategies for reducing the length of waiting lists. One complementary approach has been to implement collective mobilization actions for a variety of diseases, including those of the hand. Such actions for hand surgery, with participation by the non-governmental organization “La Chaine de L'Espoir”, carried out at the SOS Hand Institute in Recife, has contributed towards diminishing the waiting lists for hand surgery, thereby creating a greater possibility for social inclusion of these patients, who are mostly children.
Emphasis needs to be given to another factor inherent to carrying out collective mobilization actions for hand surgery. There was an exchange of experiences between French and Brazilian hand surgeons through these actions at SOS Hand in Recife, and this contributed towards achieving the target. Thus, collective mobilization actions may lead to training for specialized human resources.
Nosology of congenital hand diseases
Syndactyly has appeared as the most common congenital malformation of the hand in several series, representing 50% of such anomalies. Nonetheless, in other series, polydactyly has been mentioned as having the highest incidence. With regard to syndactyly, an analysis of 7,478,746 births in China found 2,311 cases of this malformation, which represents an incidence of 3.09 cases per 10,000 live births and stillbirths. In a general analysis on large series, the incidence of this abnormality was found to be between 1/2,000 to 1/3,000 live newborns. Through stratifying this incidence as syndactyly alone or syndactyly associated with other malformations, the rates become 1.32/10,000 and 1.77/10,000, respectively(22). These data are concordant with the fact that this congenital malformation was the one most frequently treated in the collective mobilization actions at SOS Hand in Recife. This probably corresponds to greater incidence of this malformation in the regions of origin of the patients included in the present study.
With regard to polydactyly, a study comparing the incidence of polydactyly in Latin America (ECLAMC) involving 3,128,957 live and stillborn neonates and another collaborative study on congenital malformations in the Spanish Community (ECEMC) involving 1,093,865 live newborns and 7,271 stillbirths found that the incidence was 150.2/100,000 for ECLAMC and 67.4/100,000 for ECEMC. These rates were higher than the syndactyly rates(10). It seems that the most accepted incidence rate is 1/1,000 live newborns18, 19. In line with the prevalence trends for congenital hand diseases, polydactyly was the second most common malformation in the present study. This was similar to the findings from an important surgical series in another country(20). It needs to be emphasized that the cases of bifid thumb and triphalangism were stratified as malformations independent of polydactyly, whereas in reality they form part of the wider group of types of polydactyly. In this circumstance, the frequency would be 53/240 (22.1%).
It is possible that there may have been a bias towards relatively low frequency of polydactyly in the present study, given that simpler cases of this disease might have been operated by other professionals, such as pediatric surgeons or plastic surgeons, in institutions that attend cases of lower complexity.
Bifid or double thumb has been considered to be the most frequent abnormality of the upper extremity, and it has been reported as the most common form of polydactyly15, 16, 20. In studies based on registers of congenital abnormalities, this malformation presents a general prevalence that is estimated to be 2.08 per 10,000 live newborns. In some countries like Bolivia, the prevalence reaches 3.37 per 10,000 live newborns(22). It also needs to be considered that, over the eight collective mobilizations, four cases of triphalangism of the thumb were operated, and that these can also be considered to be within the spectrum of polydactyly, which would raise the prevalence of this condition to 53/240 (22.1%).
In the more consistent surgical series, bifid thumb is represented by a relatively modest number of cases. For example, in an international review covering 66 years of surgical experience, the complications from 54 cases were reviewed, of which 16 underwent simple excision and 38 underwent reconstructive surgery of greater complexity(14). Another example that demonstrates the small number of cases reported in the literature is a review of 10 years of experience of surgical treatment of radial polydactyly at a large plastic surgery center in Brazil, in which the surgical experience of 19 cases of bifid thumb was analyzed(14). In the present series, the inclusion of 19 cases operated over the eight collective mobilizations at SOS Hand, in Recife, over a five-year period, makes the present study one of the largest case series on this disease in Brazil and emphasizes not only the social importance but also the scientific importance of the collective mobilizations for hand surgery implemented at this institution.
The classifications of congenital malformations of the hand make it possible to include most of the patients in specific phenotypes that provide the basis for nosological classification. However, in some cases, it is difficult to fit the anatomical details to specific lesions. Fusions and lack of organization of bone components may complicate the particular phenotypic features of a nosological type. These patients presented a diversity of phenotypes that were superposed within other diagnoses in the existing classification(35). Under these circumstances, 14/240 (5.8%) of the cases in the present series were thus catalogued. Most of them were patients with syndromes.
Cleft hand is an infrequent malformation, with an incidence of around one case per 20,000 live newborns. In some cases, it is associated with malformation of the feet. In an evaluation on 850,742 live births in Canada, the incidence was 1/19,784 neonates(36). It seems that there has been an increase in the prevalence of this abnormality, given that in Denmark in the 1940s, its prevalence was one case per 111,777 inhabitants(20). The diagnosis and treatment of 13 cases of cleft hand in the present study demonstrates the range of hand phenotypes that can be observed in collective mobilizations for surgery. Moreover, these cases provide density of surgical training and technical refinement for treating new cases, thereby increasing the credibility the institution and its professionals.
The thumb is the digit most frequently involved when trigger finger is diagnosed in children. The congenital nature of this malformation is still a matter of controversy and the etiology is unknown. This entity, which is also known as trigger thumb due to development error, corresponds to a spectrum of abnormalities that result in loss of extension and abduction of the digit. There are surgical series reported in the worldwide literature that include significant numbers of cases(20). For example, at a hand surgery service in Turkey, a series of surgical cases involving 47 trigger thumbs in 36 children was reported(23). In another important series of case reports from an international hand surgery service in the Netherlands, operations carried out on 27 children over a five-year period were reported. Of these, 16 were single abnormalities(37).
Likewise, the attendance provided for 12 children with trigger thumb in the present study shows the range of phenotypes of hand malformations that are diagnosed and treated in these collective mobilizations and, in some manner, mirrors the likely incidence of this malformation among the population of the State of Pernambuco.
Camptodactyly represents around 1% of congenital malformations of the hand and most frequently affects the fifth finger. The anatomical abnormalities of this condition are generally related to the lumbrical muscles, superficial digital flexors, superficial subcutaneous tissue and anomalous extensor muscles(31). The 11 cases (4.6%) that formed part of the present study are a larger phenotypic representation of this condition than in other series20, 31. They may constitute a more formal surgical indication because of the functional abnormality that this condition causes, or may indicate lower availability of conservative treatment in the region, thereby increasing the frequency of this condition on waiting lists.
Brachysyndactyly is generally recognized within the diagnostic context of syndromes such as Polland. Its incidence is very low, and it may be associated with other malformations of the musculoskeletal system. The record of nine cases operated during the collective mobilizations and reported in the present series confirm the nosological diversity observed in hand surgery carried out in the form of collective mobilization actions.
The management of eight cases (3.3%) of hemangioma of the hand in the present series of surgical conditions of the hand reinforces the idea of nosological variety of conditions treated in these collective mobilizations, given that this relatively common condition occurs most frequently in the skin of the head and neck region (60%) and trunk region (25%). The cases operated in the present series were of child hemangioma type, which is the most common type of vascular abnormality seen in hands. In this regard, hemangiomas represent around 5% of the benign tumors located in the hands.
The diagnosis of arthrogryposis involves a set of more than 300 diseases in which congenital contractures are present. The incidence of this abnormality has been estimated to be one case in every 3,000 to 5,000 live newborns. The point in common, among cases of this abnormality, is the lack of movement in a normally formed joint, which results in replacement of the muscle by fibrous and fatty tissue, thickening of the joint capsule and ligaments, and stiffness. Although this abnormality most frequently affects the lower limbs, it may affect the upper limbs, including the shoulder, elbow, hand and fingers(44). Most of these patients are treated conservatively, but some cases require surgical intervention. The inclusion of seven cases (2.9%) of arthrogryposis in the nosology of the congenital deformities operated in the collective mobilizations shows not only the importance of collective mobilization actions for hand surgery but also the need to expand the availability of reference centers for hand surgery.
The remaining cases, with lower relative frequencies, represent rare congenital malformations of the hand that are generally published in the form of case reports or small case series.
Overall, from analysis on the nosology and management of the congenital hand diseases treated over the eight collective mobilizations, it was observed that the field of knowledge of hand surgery is expanding, particularly with regard to congenital malformations of the hand. This has increased surgeons' knowledge and has resulted in new treatment methods and a more scientific surgical approach. The collective mobilizations carried out in partnership with specialists from abroad contributed towards this successful enterprise.
New technologies such as osteogenic distraction and transfers of pedicle flaps have been added to the treatment principles that were well established by the pioneers of hand surgery. These have made it possible for hand surgeons to treat new problems and deal with old problems in new ways. Nevertheless, despite the growing success, challenges persist for hand surgeons. Among these are the challenges of constructing joints and expanding within the field of fetal surgery(45).
Nosology of acquired diseases of the hand
Lesions caused by obstetric trauma that affect the upper limbs are the diseases most frequently operated. These represented around 40% of the acquired lesions that were operated during the eight collective mobilizations. Such diseases present very variable incidence, ranging from 0.42 to 5.1 per 1,000 live newborns45, 46. It seems that this disease is associated with the type of delivery, such that it is seen more frequently in newborns coming from normal delivery. It should be emphasized that surgical cases only constitute 25% of the children with this obstetric complication. Since the great majority of the children operated during the collective mobilizations were from lower socioeconomic classes, it is possible that because natural delivery is more common among mother from these classes, the higher representation in this study results from this reality. On the other hand, it is important to note that preventive measures such as indications for cesarean delivery in appropriate situations, particularly for fetuses with estimated weights greater than 4,500 grams, and avoidance of “excessive” lateral traction of the fetus at the time of delivery labor, may diminish the frequency of occurrence of this complication(46).
Sequelae from hand trauma occur more frequently among young adults, and men are more commonly affected. The most common causes are work accidents through using machines, followed by trauma due to vehicle accidents. Among children, domestic accidents and accidents within the children's environment38, 39, 40, particularly at school and in traffic, are the most common causes. Like in the present series, other studies have shown that accidents with glass receptacles and falls at home were the most common causes of hand sequelae. Likewise, as in other series, breakage of the finger flexor tendons was the most common injury. It is important to note that the children in the present study had first been attended at hospital units that did not specialize in hand treatment.
It should be emphasized that the numbers of traumatic events affecting the upper limbs have been increasing, with increases in the kinetic energy involved and, consequently, greater complexity of injuries. Traumatic injuries to the hand, with loss of skin tissue and exposure of prime structures, require coverage in order to protect these structures or to facilitate future reconstruction. These points provide support for the notion that individuals with hand lesions should primarily be attended in reference units. On the other hand, it is important to mention that preventive measures can be taken in order to diminish the cost of these interventions, and that the costs of implementing preventive measures may be lower than the costs of surgical treatment for such lesions(41).
Sequelae in the upper limbs resulting from spastic cerebral palsy are presented by children who have cerebral ischemia. This condition affects around one in every 500 births. There are no reliable statistics in Brazil, but in developed countries, the prevalence of this condition has grown with the advent and dissemination of neonatal intensive care units. It is important to note that the preventive measures for this condition include the use of progesterone of corticoids to prolong pregnancy, thereby avoiding the birth of premature infants; limitation of the number of fetuses in pregnancies induced through fertilization; and induced hypothermia for newborns with encephalopathy due to hypoxia and cerebral ischemia(46).
Sequelae from electric shocks to the upper limbs of children generally occur, like in the present series, in situations of inadequate electrical installations, in homes or elsewhere, especially on the periphery of urban centers47, 48. The attendance provided for five children with such conditions during the eight collective mobilizations attests to the need to prevent such lesions, which generally comes through education.
Sequelae from burns on hands frequently occur in developed countries and probably also in Brazil. In the United States, one third of burn patients are of pediatric age. Involvement of the arm and hand is a common occurrence(49). It is important to emphasize that adequate management in specialized units at the time of the initial attendance improves the functional result and diminishes the sequelae that give rise to subsequent surgical interventions, like in the present series.
Other acquired lesions such as sequelae from cerebral abscess, scar neuroma, acquired syndactyly and cleft hand due to leprosy have occurred sporadically in hand surgery series carried out as collective mobilizations. In this respect, the present study is novel within the Brazilian literature.
Attendance for surgically-treated hand disease through the Brazilian National Health System
With regard to attendance provided for individuals with surgically-treated hand disease through the Brazilian National Health System (SUS), it needs to be noted that although the decentralization of SUS activities to municipalities has achieved a variety of advances (primary care in all municipalities and increased implementation of the Family Healthcare Program and Community Health Agent Program, etc), this movement has not enabled the same degree of expansion of specialized services, hospital beds, intensive care, elective surgery or emergency surgery, including hand surgery.
SUS maintains its provision of these services through the private sector, and SUS administrators have been unable to regulate such services adequately, with a few honorable exceptions. There has not been any expansion of the capacity to link together several municipalities in order to integrate and hierarchically organize these services and to do this between these services and primary care. The result has been fragmentation, multiplication of procedures, inadequate incorporation of technology, and so on(50). In this regard, professionals specializing in hand surgery should form an essential part of the attendance for SUS users, with advisory systems or on-call presence in emergency units, and as departments or services in public hospitals dealing with medium and high-complexity cases, particularly in university hospitals.
The alternative, in which hand surgery is performed in private hospitals in a system of collective mobilization actions, with interactions with non-governmental organizations, as described in the present study, shows the possibility that society can successfully seek to partially replace the State with regard to its constitutional function of providing healthcare as a right for all Brazilians.
CONCLUSION
The nosology of hand diseases among the patients operated during the eight humanitarian collective mobilizations included in this study was, in a general manner, similar to that of large elective hand surgery series, particularly with regard to congenital deformities.
The system of collective mobilization for hand surgery is important for diminishing the lack of such activities in public institutions and was shown to be very efficient. This report on the nosology of hand diseases that were operated under the collective mobilization system may be useful for SUS, regarding provision of professional participation in hospital units, especially in emergencies, for SUS users.
Footnotes
Work performed at the SOS Hand Institute, Recife, PE.
Declaramos inexistência de conflito de interesses neste artigo
REFERENCES
- 1.Suresh S, Thangavel G, Sujatha J, Indrani S. Methodological issues in setting up a surveillance system for birth defects in India. Natl Med J India. 2005;18(5):259–262. [PubMed] [Google Scholar]
- 2.Sípek A, Gregor V, Sípek A, Jr, Horácek J, Klaschka J, Skibová J. Birth defects in the Czech Republic in 1994-2007. Ceska Gynekol. 2009;74(1):;31–;44. [PubMed] [Google Scholar]
- 3.Edmonds LD, James LM. Temporal trends in the prevalence of congenital malformations at birth based on the birth defects monitoring program, United States, 1979-1987. MMWR CDC Surveill Summ. 1990;39(4):19–23. [PubMed] [Google Scholar]
- 4.Mattos TC, Giuliani R, Hasse HB. Congenital malformations detected in 731 autopsies of children aged 0 to 14 years. Teratology. 1987;35(3):305–307. doi: 10.1002/tera.1420350303. [DOI] [PubMed] [Google Scholar]
- 5.Victora CG. Intervenções para reduzir a mortalidade infantil, pré-escolar e materna no Brasil. Rev Bras Epidemiol. 2001;4(1):3–69. [Google Scholar]
- 6.Arruda TAM, Amorim MM, Souza AS. Mortalidade determinada por anomalias congênitas em Pernambuco, Brasil, de 1993 a 2003. Rev Assoc Med Bras. 2008;54(2):122–126. doi: 10.1590/s0104-42302008000200013. [DOI] [PubMed] [Google Scholar]
- 7.Tuma Júnior P, Arrunategui G, Wada A, Friedhofer H, Ferreira MC. Rectangular flaps technique for treatment of congenital hand syndactily. Rev Hosp Clin Fac Med São Paulo. 1999;54(4):107–110. doi: 10.1590/s0041-87811999000400001. [DOI] [PubMed] [Google Scholar]
- 8.Boeing M, Paiva LCF, Garcias GL, Roth MGM, Santos IS. Epidemilogia das polidactilias: um estudo de casos e controles na população de Pelotas-RS. J Pediatria. 2001;77(2):148–152. doi: 10.2223/jped.196. [DOI] [PubMed] [Google Scholar]
- 9.Pardini AG, Santos MA, Freitas AD. Bandas de constrição congênitas. Acta Ortop Bras. 2001;9(2):3–10. [Google Scholar]
- 10.Barboza LE, Prestes Neto R, Fonseca MJA, Santos JBG, Falopas F. Tratamento cirúrgico das sindactilias congênitas da mão pela técnica de Bauer. Rev Bras Ortop. 2006;41(3):54–60. [Google Scholar]
- 11.Castilla EE, Lugarinho da Fonseca R, da Graca Dutra M, Bermejo E, Cuevas L, Martínez-Frías ML. Epidemiological analysis of rare polydactylies. Am J Med Genet. 1996;65(4):295–303. doi: 10.1002/(SICI)1096-8628(19961111)65:4<295::AID-AJMG10>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 12.Castilla EE, Lugarinho R, da Graça Dutra M, Salgado LJ. Associated anomalies in individuals with polydactyly. Am J Med Genet. 1998;80(5):459–465. doi: 10.1002/(sici)1096-8628(19981228)80:5<459::aid-ajmg5>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 13.Siqueira MA, Sterodimas A, Boriani F, Pitanguy I. A 10-year experience with the surgical experience of surgical treatment or radial polydactyly. Ann Ital Chir. 2008;79(6):441–444. [PubMed] [Google Scholar]
- 14.Townsend DJ, Lipp EB, Jr, Chun K, Reinker K, Tuch B. Thumb duplication, 66 years' experience–a review of surgical complications. J Hand Surg Am. 1994;19(6):973–976. doi: 10.1016/0363-5023(94)90099-X. [DOI] [PubMed] [Google Scholar]
- 15.Ozalp T, Coskunol E, Ozdemir O. Thumbs duplication: an analysis of 72 thumbs. Acta Orthop Traumatol Turc. 2006;40(5):388–391. [PubMed] [Google Scholar]
- 16.Vasseur C, Martinot V, Pellerin P, Herbaux B, Debeugny P. Palmar burns of the hand in children. 81 cases. Ann Chir Main Memb Super. 1994;13(4):233–239. doi: 10.1016/s0753-9053(05)80001-8. [DOI] [PubMed] [Google Scholar]
- 17.Leck I, Lancashire RJ. Birth prevalence of malformations in members of different ethnic groups and in the offspring of matings between them, in Birmingham, England. J Epidemiol Community Health. 1995;49(2):171–179. doi: 10.1136/jech.49.2.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kostakoglu N, Kayikcioglu A, Safak T, Ozcan G, Kecik A, Gursu G. Macrodactyly: report of eight cases of a rare anomaly. Turk J Pediatr. 1996;38(1):73–79. [PubMed] [Google Scholar]
- 19.de la Torre J, Simpsom RL. Complete digital duplication: a case report and review of ulnar plydactyly. Ann Plast Surg. 1998;40(1):76–79. doi: 10.1097/00000637-199801000-00017. [DOI] [PubMed] [Google Scholar]
- 20.Larsen CF. Demography and social impact. In: Gupta A, Kay SPJ, Scheker LR, editors. The growing hand: diagnosis and management of the upper extremity in children. Mosby; New York: 2000. pp. 121–124. [Google Scholar]
- 21.Orioli IM, Castilla EE. Thumb/hallux duplication and preaxial polydactyly type I. Am J Med Genet. 1999;82(3):219–224. [PubMed] [Google Scholar]
- 22.Herdem M, Bayram H, Togrul E, Sarpel Y. Clinical analysis of the trigger thumb of childhood. Turk J Pediatr. 2003;45(3):237–239. [PubMed] [Google Scholar]
- 23.Dautel G. Camptodactylies. Chir Main. 2003;22(3):115–124. doi: 10.1016/s1297-3203(03)00044-1. [DOI] [PubMed] [Google Scholar]
- 24.Deunk J, Nicolai JP, Hamburg SM. Long-term results of syndactyly correction: full-thickness versus split-thickness skin grafts. J Hand Surg. 2003;28(2):125–130. doi: 10.1016/s0266-7681(02)00306-6. [DOI] [PubMed] [Google Scholar]
- 25.Fernández-Vázquez JM, Schenk-Palao J, Fernández-Palomo J, Camacho-Galindo J. Triphalangeal thumb. Cir Cir. 2003;71(6):469–474. [PubMed] [Google Scholar]
- 26.Dai L, Zhou GX, Zhu J, Mao M, Heng ZC. Epidemiological analysis of syndactyly in Chinese perinatals. Zhonghua Fu Chan Ke Za Zhi. 2004;39(7):436–438. [PubMed] [Google Scholar]
- 27.Abdel-Ghani H, Amro S. Characteristics of patients with hypoplastic thumb: a prospective study of 51 patients with the results of surgical treatment. J Pediatr Orthop B. 2004;13(2):127–138. doi: 10.1097/00009957-200403000-00013. [DOI] [PubMed] [Google Scholar]
- 28.Sebastin SJ, Puhaindran ME, Lim AY, Lim IJ, Bee WH. The prevalence of absence of the palmaris longus–a study in a Chinese population and a review of the literature. J Hand Surg Br. 2005;30(5):525–527. doi: 10.1016/j.jhsb.2005.05.003. [DOI] [PubMed] [Google Scholar]
- 29.Velisavljev-Filipović G. Arthrogryposis multiplex congenita – a rare congenital stiff joints syndrome. Med Pregl. 2006;59(7-8):375–379. doi: 10.2298/mpns0608375v. [DOI] [PubMed] [Google Scholar]
- 30.Forrester MB, Merz RD. Rates for specific birth defects among offspring of Japanese mothers, Hawaii, 1986-2002. Congenit Anom (Kyoto) 2006;46(2):76–80. doi: 10.1111/j.1741-4520.2006.00106.x. [DOI] [PubMed] [Google Scholar]
- 31.Salazard B, Quilici V, Samson P. Camptodactyly. Chir Main. 2008;27(Suppl 1):S157–S164. doi: 10.1016/j.main.2008.07.018. [DOI] [PubMed] [Google Scholar]
- 32.Al-Qattan MM, Al-Shanawani B, Al-Thunayan A, Al-Namla A. The clinical features of ulnar polydactyly in a middle eastern population. J Hand Surg Eur. 2008;33(1):47–52. doi: 10.1177/1753193407087888. [DOI] [PubMed] [Google Scholar]
- 33.Ali M, Jackson T, Rayan GM. Closing wedge osteotomy of abnormal middle phalanx for clinodactyly. J Hand Surg Am. 2009;34(5):914–918. doi: 10.1016/j.jhsa.2009.01.007. [DOI] [PubMed] [Google Scholar]
- 34.Ogino T. Clinical features and teratogenic mechanisms of congenital absence of digits. Dev Growth Differ. 2007;49(6):523–531. doi: 10.1111/j.1440-169X.2007.00939.x. [DOI] [PubMed] [Google Scholar]
- 35.Elliot AM, Reed MH, Evans JÁ. Central ray deficiency with extensive syndactily: a dilemma for classification. Genet Couns. 2009;20(1):27–43. [PubMed] [Google Scholar]
- 36.Elliot AM, Reed MH, Chudley AE, Chodirker BN, Evans JA. Clinical and epidemiological findings in patients with central ray deficiency: split hand foot malformation (SHFM) in Manitoba, Canada. Am J Med Genet A. 2006;140(13):1428–1439. doi: 10.1002/ajmg.a.31245. [DOI] [PubMed] [Google Scholar]
- 37.van Loveren M, van der Biezen JJ. The congenital trigger thumb: is release of the first annular pulley alone sufficient to resolve the triggering? Ann Plast Surg. 2007;58(3):335–337. doi: 10.1097/01.sap.0000238336.30617.72. [DOI] [PubMed] [Google Scholar]
- 38.Choi M, Armstrong MB, Panthaki ZJ. Pediatric hand burns: thermal, electrical, chemical. J Craniofac Surg. 2009;20(4):1045–1048. doi: 10.1097/scs.0b013e3181abb25f. [DOI] [PubMed] [Google Scholar]
- 39.Evans-Jones G, Kay SP, Weindling AM, Cranny G, Ward A, Bradshaw A. Congenital brachial palsy: Incidence, causes, and outcome in the United Kingdom and Republic of Ireland. Arch Dis Child Fetal Neonatal Ed. 2003;88(3):F185–F189. doi: 10.1136/fn.88.3.F185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Andersen J, Watt J, Olson J, Aerde JV. Perinatal brachial plexus palsy. Paediatr Child Health. 2006;11(2):93–100. doi: 10.1093/pch/11.2.93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sahin F, Dalgic Yücel S, Ylmaz F, Ercalik C, Esit N, Kuran B. Characteristics of pediatric hand injuries followed up in a hand rehabilitation unit. Ulus Travma Acil Cerrahi Derg. 2008;14(2):139–144. [PubMed] [Google Scholar]
- 42.Claudet I, Toubal K, Carnet C, Rekhroukh H, Zelmat B, Debuisson C, Cahuzac JP. When doors slam fingers jam! Arch Pediatr. 2007;14(8):958–963. doi: 10.1016/j.arcped.2007.03.019. [DOI] [PubMed] [Google Scholar]
- 43.Ljunberg EM, Carlsson KS, Dahlin LB. Cost per case or total cost? The potential prevention of hand injuries in young children – retrospective and prospective studies. BMC Pediatr. 2008;8(28):1–11. doi: 10.1186/1471-2431-8-28. Disponível em: http://www.biomedcentral.com/1471-2431/8/28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Parsch K, Pietrzak S. Congenital multiple arthrogryposis. Orthopade. 2007;36(3):281–290. doi: 10.1007/s00132-007-1044-0. [DOI] [PubMed] [Google Scholar]
- 45.McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000;25(6):1007–1037. doi: 10.1053/jhsu.2000.6457. [DOI] [PubMed] [Google Scholar]
- 46.O'Shea TM. Diagnosis, treatment, and preventions of cerebral palsy. Clin Obstet Gynecol. 2008;51(4):816–828. doi: 10.1097/GRF.0b013e3181870ba7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Choi M, Armstrong MB, Panthaki ZJ. Pediatric hand burns: thermal, electrical, chemical. J Craniofac Surg. 2009;20(4):1045–1048. doi: 10.1097/scs.0b013e3181abb25f. [DOI] [PubMed] [Google Scholar]
- 48.Ogilvie MP, Panthaki ZJ. Electrical burns of the upper extremity in the pediatric population. J Craniofac Surg. 2008;19(4):1040–1046. doi: 10.1097/SCS.0b013e318175f523. [DOI] [PubMed] [Google Scholar]
- 49.Birchenough SA, Gampper TJ, Morgan RF. Special considerations in the management of pediatric upper extremity and hand burns. J Craniofac Surg. 2008;19(4):933–934. doi: 10.1097/SCS.0b013e318175f3f6. [DOI] [PubMed] [Google Scholar]
- 50.Assis E, Cruz VS, Trentin EF, Lucio HM, Meira A, Monteiro JCK, Cria SM, Focesi MR, Cielo CA, Guerra LM, Farias RMS. Regionalização e novos rumos para o SUS: a experiência de um colegiado regional. Saude Soc. [online] 2009;18(1):17–21. [Google Scholar]