

Abstract
Objective: The purpose of this study was to evaluate the relationship between the lateral projection of the acromion and rotator cuff tears (RCTs) in the Brazilian population. Methods: The lateral projection of the acromion was measured using anteroposterior radiographs of the shoulders, carried out with the glenoid cavity in absolute profile and the humeral head in the neutral position or with internal rotation. The acromion index (AI) was defined as the ratio between the distance from the plane of the glenoid cavity to the lateral edge of the acromion and the distance from the plane of the glenoid cavity to the lateral edge of the humeral head. This index was measured in 83 patients (mean age of 54 years) with RCTs and compared with a group of 28 individuals (mean age of 48 years) without RCTs. The presence or absence of RCTs was determined by means of magnetic resonance imaging. Results: The mean AI was 0.7194 for the patients with RCTs and 0.6677 for the individuals without RCTs, in the Brazilian population. This difference was statistically significant, with P < 0.001. Conclusion: A relationship can be established between AI and rotator cuff tears in the Brazilian population.
Keywords: Rotator cuff, Acromion, Radiography
INTRODUCTION
The etiology of rotator cuff tears (RCTs) is still controversial(1). However, they have been correlated with the format of the acromion(2). Bigliani et al(3) described three types of acromion and correlated type III (hooked) with greater prevalence of RCTs. Wang and Shapiro(4), along with Ikemoto et al(5), reported greater prevalence of this type of acromion among older patients.
Zuckerman et al(6) conducted a morphometric study on the shoulders of cadavers and found greater anterior projection and less inclination of the acromion in cadavers with RCTs, in comparison with those without such lesions. Another parameter for evaluating the format of the acromion is its lateral angulation, which was studied by Banas et al(7) using magnetic resonance images. They found smaller angles in patients with RCTs.
Analyzing the lateral appearance of the acromion shape, Nyffeler et al(2) and Torrens et al(8) found a direct relationship between lateral projection of the acromion and the presence of RCTs. From this relationship, Nyffeler et al(2) proposed a model to explain this, in which the vector of the muscle force resulting from the deltoid muscle would be influenced by the lateral projection of the acromion. Contraction of the deltoid muscle during active abduction would pull the humeral head upwards and would also put pressure on it, against the glenoid cavity. The orientation of the resultant force vector depends on the orientation of the muscle fibers of the deltoid at their origin in the acromion. The more lateral their origin is in the acromion, the greater the ascending component of the resultant force will be; and the less the lateral projection of the acromion is, the greater the compressive component of the force against the glenoid cavity will be (Figure 1). It might be imagined that a greater ascending force component (Fa) would favor subacromial impact and, consequently, degenerative changes to the supraspinal tendon, while a greater compressive force (Fc) would favor degenerative changes to the shoulder joint(2). However, there is no consensus in the literature regarding this relationship, given that neither Van Nüffel and Nijs(9) nor Itoi* found it in their studies, even though their work was carried out using similar methodology.
Figure 1.
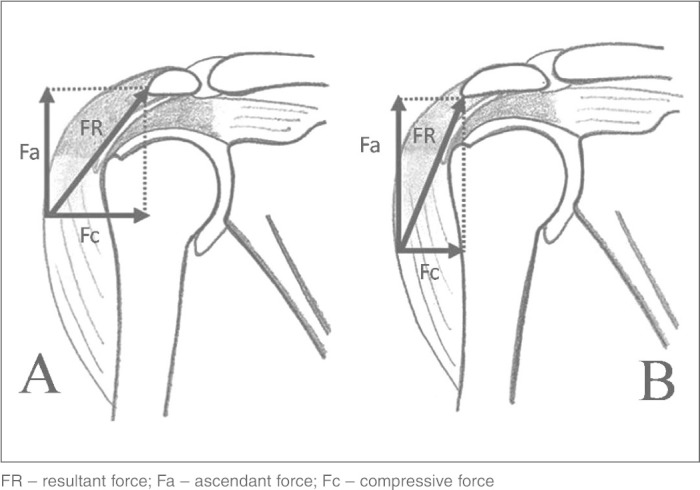
A) Schematic representation of the resultant force that acts on the humeral head when there is a minor lateral projection of the acromion. B) Representation of the resultant force when the insertion of the deltoid is more lateral.
Our study had the aim of evaluating the shape of the acromion, and specifically its lateral projection, using methodology similar to that of Van Nüffel and Nijs(9) and Itoi*, with radiographic measurements using an index that was then correlated with RCT occurrences.
SAMPLE AND METHODS
Radiographs from patients who undergone operations performed by the Shoulder and Elbow Surgery Group of the Department of Orthopedics and Traumatology, School of Medical Sciences, Santa Casa de Misericórdia de São Paulo, Pavilhão “Fernandinho Simonsen舡, between July 1995 and December 2007.
The shoulder radiographs were standardized and only those that had been produced with correction for anteversion of the glenoid cavity were used. The arm was radiographed in a resting position alongside the body, with the proximal region of the humerus in a neutral position or with internal rotation. According to the study published by Nyffeler et al(2), there is no difference in measuring the acromiale index with the shoulder in neutral position of with internal rotation.
Two measurements were made on these radiographic images, taking the reference points to be the plane of the glenoid cavity, the lateral extremity of the humeral head and the lateral extremity of the acromion. The distance between the lateral extremity of the acromion and the plane of the glenoid cavity was called GA. The distance between the lateral extremity of the humerus and the plane of the glenoid cavity was called GU. The ratio between the values of GA and GU forms an index known as the acromion index (AI) (Figure 2).
Figure 2.

Radiographic image of the right shoulder, in anteropos-terior view, after scanning with the millimeter ruler used to calibrate the software. From this, the acromion index (AI) is demonstrated: this is obtained as the ratio between the distance from the glenoid cavity to the lateral edge of the acromion (GA) and the distance from the glenoid cavity to the lateral edge of the humerus (GU).
There was no concern regarding the distance between the ampoule of the X-ray apparatus and the radiographic film, since was an index and changes to the parameters would not interfere with the result. To check that variation in the inclination of the X-ray ampoule would not alter the AI measurements, we created a control group of 10 patients. This group underwent radiography centered on the glenoid cavity in anteroposterior view, at angles of 0°, 30° of caudal inclination and 30° of cranial inclination. The AI from these radiograph views was measured and subjected to statistical analysis (Friedman test). This analysis on the three views showed similar values, with a p-value of 0.999, and it was concluded that the inclination of the X-ray ampoule did not have any influence on the result (Table 1).
Table 1.
Variation in the acromion index according to radiographic incidence view
| Acromion index | n | Mean | Standard deviation | Minimum | Maximum | Median | 25th percentile | 75th percentile | P value |
|---|---|---|---|---|---|---|---|---|---|
| 30° cranially | 10 | 0.66309 | 0.09457 | 0.51820 | 0.80240 | 0.66585 | 0.59290 | 0.73233 | |
| 0° | 10 | 0.66489 | 0.09368 | 0.50930 | 0.79950 | 0.67545 | 0.59438 | 0.73433 | >0.999 |
| 30° caudally | 10 | 0.66434 | 0.09338 | 0.52780 | 0.80230 | 0.65980 | 0.59245 | 0.74283 |
Source: SAME DOT-ISCMSP
n = total number of patients
The inclusion criterion was that the patients selected should present a completely torn rotator cuff, proven by magnetic resonance images and through observation during the surgery. For the control group, patients treated for shoulder diseases who did not show RCTs on magnetic resonance images were selected. We defined the exclusion and non-inclusion criteria as cases of antecedents of fractures of the scapular belt, arthritis, degenerative arthrosis, osteonecrosis and sequelae from infection.
The patients selected were divided into two groups: group I, with a completely torn rotator cuff (83 cases); and group II, with an undamaged rotator cuff (28 cases) (Table 2).
Table 2.
Distribution of groups I and II in relation to sex, mean age and side affected
| Group I | Group II | |
|---|---|---|
| n | 83 | 28 |
| Mean age (years) | 54 (32-77) | 48 (35-63) |
| Sex | 30 men (36%) 53 women (64%) | 12 men (43%) 16 women (57%) |
| Side | 65 right (78%) 18 left (22%) | 18 right (64%) 10 left (36%) |
Source: SAME-DOT ISCMSP
n = total number of patients
The radiographs were digitized using a scanner (HP Deskjet F4180®). These images were then analyzed using the Image J 1.41 software (Wayne Rasband, Research Services Branch, National Institute of Mental Health, Bethesda, Maryland, USA), which is available for download from the website http://rsbweb.nih.gov. This enables precise measurement of distances in figures, starting from a parameter for calibration. A ruler marked out in millimeters was used as the calibration parameter (Figure 2).
The data obtained were subjected to statistical analysis by means of Student's t test, which was controlled using Levene's test for equality of variance, with a significance level of 5%. The chi-square test was also used, with the aim of investigating a possible difference in the sex distribution between the study groups.
RESULTS
In group I, the mean age was 54 years, with a range from 32 to 77 years, while in group II, the mean age was 48 years, ranging from 35 to 63 years. In group I, females predominated, accounting for 64% (53 women). This was also found in group II, in which 57% of the patients were female (16 women). However, this difference in sex distribution in groups I and II was not statistically significant (p = 0.527) (Table 2).
With regard to the side affected, there was predominance of the right side in both groups, accounting for 78% of the shoulders in group I and 64% of the shoulders in group II (Table 2).
We found a mean AI of 0.7194 among the individuals who presented RCTs (group I); and a mean AI of 0.6677 among the individuals who presented an undamaged rotator cuff (group II). The statistical analysis showed a correlation with p = 0.001, i.e. there was a statistically significant relationship between RCTs and greater lateral projection of the acromion.
DISCUSSION
In 1972, Neer(10) made an important study on impact syndrome and identified that forces impacting on the lower portion of the acromion, the coracoacromial ligament and the inferior surface of the acromioclavicular ligament were the agents responsible for the narrowing of the subacromial space, which led to tendon lesions. However, it is now known that the pathogenesis of RCTs is probably multifactorial(1). One of the possible causes for such lesions is greater lateral projection of the acromion, as proposed by Nyffeler et al(2). However, there is no consensus in the literature in relation to this association, in the way seen for the anterior projection of the acromion3, 6, 7, 10.
Our results support the theory of Nyffeler et al(2), since individuals with RCTs presented a greater AI, i.e. greater lateral projection of the acromion. This shape of the acromion causes the origin of the deltoid to be more lateral, thereby producing a resultant force with a more ascendant orientation (Fa), which probably favors subacromial impact. Among the patients with an undamaged rotator cuff, this index was lower, i.e. there was less lateral projection of the acromion, with a resultant force that was oriented more towards compression (Fc) against the glenoid cavity. Although not part of the objective of our study, we did not find any signs of arthrosis in the shoulder joint of these patients, as this theory would suppose. Our findings also in some way corroborate the results of Torrens et al(8), given that we also found a relationship between greater lateral projection of the acromion and occurrences of RCTs, even though the calculation used to determine the lateral projection of the acromion was made differently, i.e. using another index.
On the other hand, our results and those of Nyffeler et al(2) are not the same as those of Van Nüffel and Nijs(9) and Itoi*, even though we used the same way of measuring the lateral projection of the acromion and our groups were similar regarding sex and age. The only difference was that both the group with RCTs and the control group in the study by Itoi* consisted mostly of men, which could constitute a form of bias, given that there have been reports that RCTs are more prevalent among women, although this too is not a matter of consensus in the literature(11).
The individuals with RCTs and with undamaged rotator cuffs who were selected both in previous studies and in ours had mean ages between 45 and 65 years. Thus, they were in phase III of the impact syndrome, as described by Neer(12), i.e. the stage at which complete tearing of the rotator cuff occurs.
Another factor that might have influenced the results was that the radiographic images used for measuring the AI were not standardized. However, we took care to select radiographs with correction for anteversion of the glenoid cavity, and in which the humerus was in a neutral position or in internal rotation, as already demonstrated by Nyffeler et al(2), since in this way neither position would have any influence on the AI. Torrens et al(8) reported previously that the distance from the ampoule to the film, at the time of producing the radiograph, also did not alter the AI because it is determined as the ratio between two measurements made on the same radiographic image. In our study, we demonstrated that the angulation of the X-ray ampoule also did not influence the determination of the AI, thereby avoiding such bias in carrying out our study.
One factor that should be taken into consideration is that Itoi* made measurements on a Japanese population, Nyffeler et al(2) on a Swiss population and Van Nüffel and Nijs(9) on a Belgian population, while our study was conducted on a Brazilian population. Since each ethnic group has its own characteristics, it could be that the differences between the results may come from a factor relating to the biotype of each ethnic group. However, to investigate this question better, further studies should be conducted, taking into consideration other morphological parameters such as the type of acromion, lateral angle and anterior inclination of the acromion, in an attempt to find the precise etiological factor that causes RCTs.
CONCLUSION
We conclude that RCTs may be associated with greater AI, i.e. greater lateral projection of the acromion.
Footnotes
Work performed in the Department of Orthopedics and Traumatology, School of Medical Sciences, Santa Casa de Sao Paulo, Pavilhão “Fernandinho Simonsen”. Director: Prof. Dr. Osmar Avanzi.
REFERENCES
- 1.Uhtof HK, Loehr J, Sarkar K. The pathogenesis of rotator cuff tears. The shoulder. In: Proceedings of the Third International Conference on Surgery of the Shoulder, Fukuoka – Japan; 1986. p. 211-2.
- 2.Nyffeler RW, Werner CM, Sukthankar A, Schmid MR, Gerber C. Association of a large lateral extension of the acromion with rotator cuff tears. J Bone Joint Surg Am. 2006;88(4):800–805. doi: 10.2106/JBJS.D.03042. [DOI] [PubMed] [Google Scholar]
- 3.Bigliani LU, Morrison DS, April EW. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans. 1986;10:216. [Google Scholar]
- 4.Wang JC, Shapiro MS. Changes in acromial morphology with age. J Shoulder Elbow Surg. 1997;6(1):55–59. doi: 10.1016/s1058-2746(97)90071-9. [DOI] [PubMed] [Google Scholar]
- 5.Ikemoto RY, Bezerra AD, Monte FA, Telles RB, Fujiki EN, Porto LCK. Acrmio em forma de gancho: uma variação anatmica ou um processo degenerativo? Rev Bras Ortop. 2005;40(8):454–463. [Google Scholar]
- 6.Zuckerman JD, Kummer FJ, Cuomo F, Simon J, Rosenblum S, Katz N. The influence of coracoacromial arc anatomy on rotator cuff tears. J Shoulder Elbow Surg. 1992;1(1):4–14. doi: 10.1016/S1058-2746(09)80010-4. [DOI] [PubMed] [Google Scholar]
- 7.Banas MP, Miller RJ, Totterman S. Relationship between the lateral acromion angle and rotator cuff disease. J Shoulder Elbow Surg. 1995;4(6):454–461. doi: 10.1016/s1058-2746(05)80038-2. [DOI] [PubMed] [Google Scholar]
- 8.Torrens C, Lopez JM, Puente I, Cáceres E. The influence of the acromial coverage index in rotator cuff tears. J Shoulder Elbow Surg. 2007;16(3):347–351. doi: 10.1016/j.jse.2006.07.006. [DOI] [PubMed] [Google Scholar]
- 9.Van Nuffel M, Nijs S. Acromial morphology, acromial index and rotator cuff problems: is there a correlation? The Pellenberg Orthopaedic Yearbook. 2006-2007:37–44. [Google Scholar]
- 10.Neer CS., 2nd Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41–50. [PubMed] [Google Scholar]
- 11.Jerosch J, Müller T, Castro WH. The incidence of rotator cuff rupture. An anatomic study. Acta Orthop Belg. 1991;57(2):124–129. [PubMed] [Google Scholar]
- 12.Neer CS., 2nd Impingement lesions. Clin Orthop Relat Res. 1983;(173):173–177. [PubMed] [Google Scholar]