

Abstract
The purpose of this study was to assess the prevalence of sagittal lumbar spine postural abnormalities and associated factors among students in the federal educational system in Florianópolis. Methods: 288 adolescents (156 males and 132 females), aged from 15 to 18 years, who were students in the federal educational system in Florianópolis, Santa Catarina, were evaluated. To gather data, photogrammetry was used following a specific protocol for postural assessment, and a questionnaire was used to identify the prevalence and frequency of pain, and the activities that triggered the problem. In the data analysis, descriptive statistics, Student's t-test for independent samples, chi-square test and Poisson's regression were used, with the significance level set at p<0.05 for all the tests. Results: The prevalence of low back pain was 49.3%, with weekly frequency in 43.1% of the sample. The prevalence of deviation was 53.8%, and 90.9% corresponded to rectification of lumbar curvature, and this affected males more frequently. A significant difference in lumbar angle was found between the sexes; higher prevalence ratios of postural deviations were found in the male group. Conclusions: The prevalences of low back pain and lumbar postural deviation were high, but the relationship between these variables did not present significance. The main causes of the lumbar pain were sports practice or vigorous activities and remaining in a seated position for extended periods of time.
Keywords: Spine, Low Back Pain, Posture, Adolescents
INTRODUCTION
Pain in the lumbar region or lumbalgia, as it is called, has been considered to be a frequent cause of morbidity and incapacity in the general population. However, its cause is not always specific(1). Independent of the causes, lumbar pain reaches epidemic levels, affecting 70 to 85% of all individuals at least once during their lives(2).
Very many circumstances contribute towards triggering lumbar pain, and some authors have considered it to be a multifactorial disease3, 4. The etiology of lumbar pain is difficult to identify because it is manifested under a variety of conditions. Among other causes, this pain has presented associations with factors such as: female sex1, 3, 5, 6, obesity1, 6, sedentarism(6), high levels of physical activity1, 3, 5, 7, reduced flexibility(4) and postural habits6, 8, 9.
Even though some studies have proven an association between postural deviations and lumbar pain10, 11, there is no consensus in the literature regarding this relationship(1). However, changes in postural patterns have been indicated as a risk factor for developing pain in the lumbar region(9), since abnormal posture causes tension in the ligaments and muscles, which indirectly affects the lumbar curvature, thus triggering pain.
The prevalence of lumbar pain during adolescence has been increasing considerably over recent decades(12), and this problem becomes even more significant when it is perpetuated into adulthood(2). In this respect, the review study by Balagué et al(1) on lumbar pain among adolescents indicated high prevalences, ranging from 30 to 51%.
Notwithstanding such problems, the number of cases of postural abnormalities of the spine during adolescence have been increasing considerably, because this is an age at which individuals are exposed to greater overloads, such as bearing the weight of school backpacks asymmetrically and inadequately(13) or remaining in a seated position and adopting inappropriate postures for long periods of time(14).
Thus, with the aim of contributing towards the literature in this field and, in particular, to be able to implement subsequent interventions, this study was devised with the objective of analyzing the prevalence of sagittal postural abnormalities in the lumbar spine and associated factors, among adolescent students in the federal educational system in Florianópolis.
METHODS
A descriptive cross-sectional study was conducted among adolescents between the ages of 15 and 18 years who were attending high school within the federal educational system in Florianópolis, SC. The population was estimated to be 850 students within this age range, enrolled in two schools.
To calculate the sample representativeness, the equation proposed by Rodrigues(15) was used. This establishes the sample size for quantitative variables, taking a sample error of 5% and a 95% confidence interval. In this manner, the number of individuals for the sample was calculated to be 265 adolescents. Since the schools were located in the same geographical region, there was no need to stratify according to locality. However, the sample was stratified according to gender, and a simple random draw was made within the strata.
The following were used as exclusion criteria: refusal of the student to participate in the study; failure to hand in the free and informed consent statement signed by the parents or guardians; age outside of the range specified for the study; failure to undergo any of the tests required for the analyses; and/or presentation of physical deficiencies that made it impossible to perform any of the procedures required for attaining the study objectives. Thus, a sample consisting of 288 students was formed, of whom 156 were male and 132 were female, with mean ages of 16 ± 1.06 years and 15.87 ± 1.05 years, respectively.
All the protocols and procedures used in the study had been approved by the Ethics Committee for Research on Human Beings of the Federal University of Santa Catarina, under protocol no. 048/07, which was in line with resolution 196/96 of the National Health Board.
Data relating to postural assessments on the lumbar spine were obtained in accordance with the procedures described by Christie et al(10), who demonstrated that there was a high correlation with radiographic data, with a significance level of 0.01. The lumbar lordosis angle was quantified in an upright standing position, in the right sagittal plane, in which the spinous processes of the vertebrae T12 (twelfth thoracic vertebra) and L5 (fifth lumbar vertebra) were identified and marked out on the skin by means of palpation. To these points, rods of 7 cm in length, negligible weight (3.4 grams), slightly concave rounded base and radius of 1 cm were attached, to enable fixation onto the transverse processes using adhesive tape. These rods made it possible to project the anatomical points in the sagittal plane, so as to avoid difficulty in viewing the markers caused by muscle protuberances. The lumbar lordosis angle was defined by the intersection of the prolongation of the rods positioned over the spinous processes of the T12 and L5 vertebra.
To analyze the sagittal deviation of the lumbar spine, photographic images from a digital camera with resolution of 3.0 megapixels were used. These images could then be digitized using graphics software to enable identification of the angle generated by the intersection of the points. To take the photographs, a fixed point suspended on a standardized plumb line was firstly calibrated. The camera was positioned on a tripod at a height of 1.20 meters above floor level and three meters from the subjects. The postural alignment of the lumbar spine was classified as normal when the values were 30 to 45°, or as a diminished lumbar angle (rectification) or as an accentuated lumbar angle (hyperlordosis), through analyzing angular values generated.
Information relating to lumbar pain was obtained by means of a structured questionnaire composed of one closed and two open questions asking about the incidence and frequency of pain in the lumbar spine and the activities that generated this pain. The clarity of the questions was tested on 10 subjects with the same characteristics as the study sample, from which a rate of 96% was obtained. The content validity was tested on five specialists, obtaining a rate of 93%.
To process the data, the Statistical Package for the Social Sciences (SPSS) software for Windows, version 15.0, as used. Firstly, descriptive statistics were produced from the data, which were organized into tables showing the distribution of frequencies, percentages and measurements of central trend (means) and dispersion (standard deviations). The variables were cross-correlated by means of contingency tables (crosstabs) in order to investigate the proportion of the adolescents affected by postural deviations and lumbar pain.
Differences between the sexes were investigated using Student's t test (lumbar angle) and the chi-square test (χ2) (lumbar pain). Poisson's regression was used to investigate crude and adjusted prevalence ratios for postural deviations in relation to sex and lumbar pain. Significance values for the crude model were obtained using the chi-square test, since according to Hosmer and Lemeshow(16), for variables to be kept in the adjusted model, they would need to present p < 0.25 in this test. The significance values of the adjusted analysis were as furnished by the Poisson test.
RESULTS
From the students' responses, the prevalence of lumbar pain in the general group was 49.6% (n = 171). A higher proportion of the females presented lumbar pain, which affected 53% of them, while the prevalence among the males was 46.2%.
Regarding the frequency of lumbar pain, as shown in Table 1, 43.1% of the adolescents reported suffering from painful conditions at least once a week.
Table 1.
Frequency of lumbar pain among adolescents within the federal educational system in Florianópolis.
| Frequency |
Male |
Female |
General |
|---|---|---|---|
| % | % | % | |
| Every day | 13.2 | 29 | 21.2 |
| Once a week | 42.7 | 43.5 | 43.1 |
| Once a month | 30.9 | 24.6 | 27.7 |
| Rarely | 13.2 | 2.9 | 8 |
| Total | 100 | 100 | 100 |
Table 1 also shows that the females presented more than twice as many cases of daily pain in the lumbar spine, in comparison with the numbers of cases among the males. The main responses relating to the reasons why painful conditions in the lumbar spine had appeared, in the opinions of the students evaluated, are presented in Table 2.
Table 2.
Distribution of the frequencies of activities that generated lumbar pain among adolescents within the federal educational system in Florianópolis.
| Activities |
Male |
Female |
General |
|---|---|---|---|
| % | % | % | |
| Domestic activities | 5 | 15 | 10 |
| Carrying weights | 19 | 12 | 15.5 |
| Carrying backpack | 10 | 13 | 11.5 |
| Remaining seated for long periods | 26 | 25 | 25.5 |
| Practicing sports or vigorous activities | 26 | 20 | 23 |
| Flexing the trunk | 9 | 9 | 9 |
| Extending the trunk | 5 | 6 | 5.5 |
| Total | 100 | 100 | 100 |
Table 2 shows that both the males and the females indicated that the main causes of pain in the lumbar spine were situations of remaining seated for long periods and sports practice or vigorous activities.
Regarding the lumbar angles generated from the postural assessment, the data in Table 3 indicate that the females presented greater angular values for lumbar curvature than shown by the males, although these were considered normal according to the classification used. On the other hand, the mean for the males (26°) was classified as a reduced angle (rectification).
Table 3.
Descriptive values for the lumbar angle among adolescents within the federal educational system in Florianópolis.
| Group |
Lumbar angle (°) |
|
|---|---|---|
| Mean | SD | |
| Male | 26 | 9.09 |
| Female | 34 | 8.62 |
| General | 30 | 9.60 |
The postural analysis made it possible to identify that the overall prevalence of deviation of the lumbar spine was 53.8% (n = 155), which consisted of 90.9% (n = 141) with rectification of the lumbar spine and 9.1%
(n = 14) with hyperlordosis. The postural patterns according to sex (Figure 1) indicated that the males presented higher percentages of postural abnormalities (64.7%), and that 62.8% of the subjects presented a rectified lumbar spine.
Figure 1.
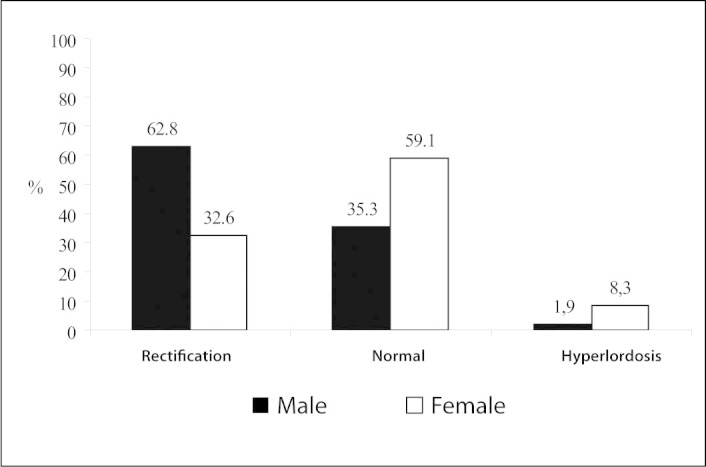
Distribution of postural patterns for the lumbar spine among the adolescents, according to sex.
From analysis on Figure 1, it was observed that the females presented a greater percentage of normal angles, such that the prevalence of deviations was 40,9%, and only 8.3% of the female subjects presented accentuated lumbar curvature (hyperlordosis).
The cross-correlation (crosstabs) on the classification data relating to postural deviation with lumbalgia indicated that pain was more associated with cases of hyperlordosis (Table 4).
Table 4.
Cross-correlation of percentage values (crosstabs) from postural evaluation with lumbar pain among adolescents within the federal educational system in Florianópolis.
| Lumbar pain | ||||||
|---|---|---|---|---|---|---|
| Angle |
Male (%) |
Female (%) |
General (%) |
|||
| Yes | No | Yes | No | Yes | No | |
| Normal | 54.5 | 45.5 | 48.7 | 51.3 | 51.1 | 48.9 |
| Rectified | 41.8 | 58.2 | 55.8 | 44.2 | 46.1 | 53.9 |
| Hyperlordosis | 33.3 | 66.7 | 72.7 | 27.3 | 64.3 | 35.7 |
The data presented in the contingency table (Table 4) show that painful conditions were more associated with angular deviations in the sagittal plane among the females (55.8% of the cases of rectification and 72.7% of the cases of hyperlordosis). It could also be seen that, in general, rectification of the lumbar angle had a lower percentage association with lumbar pain than did the other situations in which the spine was exposed.
Since the behavior of the variables of pain and lumbar angle differed between the genders, the differences between them were tested. The lumbar angle was shown to be significantly different between the sexes (p < 0.001), while the variable of pain did not present any significant difference (p = 0.330).
With the aim of analyzing the associations shown by postural deviations in the lumbar spine, while controlling for possible confounding factors, Poisson regression was used because the outcome under analysis (presence of deviation) presented high prevalence, which might have caused overestimation of the magnitude of the effect measurement, i.e. odds ratios(17). Crude and adjusted prevalence rations (PR) were calculated along with their respective 95% confidence intervals. The dependent variable for this analysis was dichotomized as no deviation (normal) and deviation present (Table 5).
Table 5.
Prevalences and crude and adjusted prevalence ratios (PR) for postural deviation in the lumbar column according to sex and pain, among adolescents within the federal educational system in Florianópolis.
| Variables | Prevalences | Crude PR (95% CI) | p-value* | Adjusted PR (95% CI) | p-value** |
|---|---|---|---|---|---|
| Postural deviation | 53.8 | - | - | - | - |
| Sex | |||||
| Female | 45.8 | 0.63 (0.53-0.74) | 0.69 (0.58-0.83) | ||
| < 0.001 | < 0.001 | ||||
| Male | 54.2 | 1 | 1 | ||
| Pain | |||||
| Yes | 49.3 | 0.93 (0.80-1.09) | |||
| 0.418 | Excluded from the model | ||||
| No | 50.7 | 1 | (crude p > 0.25) |
unadjusted p value (p from chi-square test)
p value for adjusted trend.
The data in Table 5 show that in the crude analysis, the females presented a prevalence ratio that was 37% lower for lumbar column deviation. However, the prevalence ratios for lumbar pain were not significant (p = 0.418), and were excluded from the model.
DISCUSSION
There is a consensus in the literature regarding the high prevalence of lumbar pain among adolescents2, 12, 18, 19. The review study by Balagué et al(1) showed prevalences ranging from 30 to 51%, which is in line with the results from the present study (Figure 1), thus indicating that lumbalgia affected almost half of these adolescents. Also according to this author(1), lumbalgia is more frequent among females, and this result was confirmed by the findings from the present study and is line with some others2, 5, 6 that showed this relationship.
The frequency of lumbalgia is an important point to emphasize, since more than half of the adolescents with this problem said that they felt pain in the lumbar spine at least once a week (Table 1). This proportion is greater than what was found by Alpalhão and Roballo(20) in a study on 124 adolescents, which was 32.6%. Considering that on average 21% of the adolescents in the present study had painful conditions every day, it can be seen that early diagnosis of the factors involved in this problem is very important, since this pain may diminish these individuals' quality of life.
In the reports on pain, the main activities that were indicated to be harmful were remaining seated for long periods and practicing sports or vigorous activities (Table 2), which confirms the findings in the literature, in which these factors have been shown to cause lumbalgia among adolescents1, 2, 5.
The prevalence of sagittal postural deviations in the lumbar spine was high, affecting 53.8% of the subjects. In this regard, Detsch et al(21) analyzed the sagittal plane among female adolescents and found prevalences that were even higher than in the present study, corresponding to 66% of the subjects.
The difference in angular values of the lumbar spine between the sexes was significant (p < 0.05), with lower values among the males (26°), thus corroborating the study by Damasceno et al(22), in which significant differences were found in the lumbar angles and other components of the spine, between the sexes. According to this author(22), the differences seemed to be related to differences in the measurements of components of the lumbar curvature.
Among other factors, these differences also may be related to the different structural constitution of the male and female skeletons, in which the male pelvic bone is narrower and the sacrum and ilia have a more vertical position, which diminishes the lumbar angle in relation to females(23).
Rectification was the lumbar spine deviation most often found (Figure 1), which goes against several studies on children and adolescents14, 15, 18, 21, 24, 25, 26. In these studies, analysis on the lumbar spine in the sagittal plane showed high prevalences of hyperlordosis, which was not identified in the present study. These differences may be related to the different methods used and the specificity of these methods, since certain evaluation protocols do not allow assessment of decreases in spinal curvature but only increases in curvature. Moreover, a lack of consensus regarding the lumbar angle values that should be considered normal has been observed, thus generating controversy regarding the limits that are considered normal in the sagittal plane(27). This makes it difficult to compare between studies because of the different methodologies and cutoff points used.
Another factor that should be taken into consideration is the gluteal volume. In some cases, this may be visually confounded with increased lumbar curvature, and even more so when the lumbar evaluation is done using subjective instruments.
Few studies have presented percentage prevalences of rectification among the general population. Within this context, in a study conducted among Spanish adolescents, Blanco et al(19) found prevalences of rectification that were much lower (7%) than what we found among adolescents in Florianópolis (47.7%). Likewise, in a study on children in the city of João Pessoa, State of Paraíba, Correia et al(28) found that the prevalence of rectification was 6.8%. However, Giglio and Volpon(26) stated that the curvature of the spine increased significantly with age, and that this did not allow data from children and adolescents to be compared with each other.
In relation to the prevalence of hyperlordosis, the data from the present study were lower than those of all other studies encountered. The results that were closest to the present study were those of Blanco et al(19), with a percentage of 14% for this deviation, and Politano(14), among adolescents in Cacoal, State of Rondônia, with a prevalence of 10.1%. Among adolescents in a city in Santa Catarina, Martelli and Traebert(25) found that the prevalence of hyperlordosis was around twice (20.1%) the prevalence identified in the present study. In a study conducted in the city of Sobral, State of Ceará, Mangueira(29) found that the percentage of hyperlordosis among adolescents was 17.5%.
By testing the relationships between the variables, it could be seen that the prevalence ratio for deviations was greater among the males, which may be associated with structural differences in physical composition. The high prevalence of rectification in adolescents' spines may have been associated with harmful factors to which they might have been exposed.
Considering that the subjects of the present study were of school age, certain factors relating to day-to-day postural habits may have had an influence on the appearance of deviations. Thus, the rectification of the lumbar spine may have been associated with, among other causes, the resting position adopted by the students while seated. In such situations, the resting posture is often a relaxed posture in which the body is supported on the chair through the ischial tuberosity and posterior face of the sacrum and coccyx, thereby leaving the pelvis in retroversion and the lumbar spine rectified(23). This may lead to development of muscle shortening, compensatory mechanisms and lumbalgia, in situations of long-term exposure(30). The importance of habits in the seated posture needs to be emphasized, given that 25.5% of the adolescents evaluated declared that they felt pain when they remained in this position for a long time (Table 2).
In view of the use of seated postures for long period of time, Braccialli and Vilarta(31) can be cited: these authors explained that both the deviations and the painful conditions occur because neither the body's constitution nor the functional biomechanical model was designed for remaining seated for long periods, and that this incompatibility leads to high prevalences of postural problems. In addition, the school environment favors the appearance of lumbar problems, since the ergonomics of the furniture is often inadequate, with deficiencies in layout and proportions; and the weight of school materials carried in backpacks is excessive and transported in an erroneous manner, thereby aggravating inappropriate postural habits(31).
The use of incorrect postures makes the entire locomotor system participate in and adapt to the imposed new mechanical conditions(30), and thus, among other factors, greater energy expenditure is developed to maintain body balance and carry out daily activities. This predisposes individuals to early fatigue, which may have direct repercussions on painful states and quality of life among these individuals.
The results obtained from this study not only contribute towards the literature in this field, but also indicate the need for screening for postural problems among schoolchildren, which might identify these problems at an early stage, along with the daily postural habits that result in establishing permanent problems in the lumbar spine of adolescents.
CONCLUSIONS
Based on these results, it can be concluded that: a) the prevalence of pain and postural deviations in the lumbar spine of these adolescents was high; b) rectification of the lumbar spine was the postural deviation most often present, with greater prevalence among male adolescents; c) there was a significant difference in the lumbar angle between the sexes, such that it was greater among females; d) lumbalgia was more prevalent among females; e) independent of sex, lumbalgia affected a large proportion of these adolescents at least once a week; f) the main causes of lumbar pain were sports practice or vigorous activities and remaining seated for long periods of time; g) the prevalence ratios indicated that decreased lumbar angle was associated with male sex; and h) lumbar pain did not present any association with sagittal deviation in the lumbar spine.
ACKNOWLEDGEMENTS
Our thanks to CAPES and CNPq for their support in carrying out this work.
Footnotes
Work performed in the Biomechanics Laboratory, Federal University of Santa Catarina, Florianópolis, SC.
Declaramos inexistência de conflito de interesses neste artigo
REFERENCES
- 1.Balagué F, Troussier B, Salminen JJ. Non-specific low back pain in children and adolescents: risk factors. Eur Spine J. 1999;8(6):429–438. doi: 10.1007/s005860050201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Andersson GB. Epidemiological features of chronic low-back pain. Lancet. 1999;354(9178):581–585. doi: 10.1016/S0140-6736(99)01312-4. [DOI] [PubMed] [Google Scholar]
- 3.Harreby M, Nygaard B, Jessen T, Larsen E, Storr-Paulsen A, Lindahl A, Fisker I, Laegaard E. Risk factors for low back pain in a cohort of 1389 Danish school children: an epidemiologic study. Eur Spine J. 1999;8(6):444–450. doi: 10.1007/s005860050203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jones MA, Stratton G, Reilly T, Unnithan VB. Biological risk indicators for recurrent non-specific low back pain in adolescents. Br J Sports Med. 2005;39(3):137–140. doi: 10.1136/bjsm.2003.009951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Phélip X. Why the back of the child? Eur Spine J. 1999;8(6):426–428. doi: 10.1007/s005860050200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marras WS. Occupational low back disorder causation and control. Ergonomics. 2000;43(7):880–902. doi: 10.1080/001401300409080. [DOI] [PubMed] [Google Scholar]
- 7.McMeeken J, Tully E, Stillman B, Nattrass C, Bygott IL, Story I. The experience of back pain in young Australians. Man Ther. 2001;6(4):213–220. doi: 10.1054/math.2001.0410. [DOI] [PubMed] [Google Scholar]
- 8.McGorry RW, Hsiang SM, Snook SH, Clancy EA, Young SL. Meteorological conditions and self-report of low back pain. Spine (Phila Pa 1976) 1998;23(19):2096–2102. doi: 10.1097/00007632-199810010-00011. [DOI] [PubMed] [Google Scholar]
- 9.Evcik D, Yücel A. Lumbar lordosis in acute and chronic low back pain patients. Rheumatol Int. 2003;23(4):163–165. doi: 10.1007/s00296-002-0268-x. [DOI] [PubMed] [Google Scholar]
- 10.Christie HJ, Kumar S, Warren SA. Postural aberrations in low back pain. Arch Phys Med Rehabil. 1995;76(3):218–224. doi: 10.1016/s0003-9993(95)80604-0. [DOI] [PubMed] [Google Scholar]
- 11.Jesus GT, Marinho ISF. Causas de lombalgia em grupos de pessoas sedentárias e praticantes de atividades físicas. Revista Digital [periódico na internet], 2006; 10(92). [Acesso em: 20/06/2007]. Disponível em: www.efdeportes.com/efd92/lombal.htm
- 12.Hakala P, Rimpelä A, Salminen JJ, Virtanen SM, Rimpelä M. Back, neck, and shoulder pain in Finnish adolescents: national cross sectional surveys. BMJ. 2002;325(7367):743. doi: 10.1136/bmj.325.7367.743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Grimmer K, Dansie B, Milanese S, Pirunsan U, Trott P. Adolescent standing postural response to backpack loads: a randomised controlled experimental study. BMC Musculoskelet Disord. 2002;3:1–10. doi: 10.1186/1471-2474-3-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Politano RC. Levantamento dos desvios posturais em adolescentes de 11 a 15 anos em escola estadual do município de Cacoal-RO [dissertação]. Brasília: Universidade de Brasília, UnB; 2006
- 15.Rodrigues PC. Bioestatística. 3a ed. EduFF; Niterói: 2002. [Google Scholar]
- 16.Hosmer DW, Leneshow S. Applied logistic regression. Wiley; New York: 1989. [Google Scholar]
- 17.Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3:21. doi: 10.1186/1471-2288-3-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Widhe T. Spine: posture, mobility and pain. A longitudinal study from childhood to adolescence. Eur Spine J. 2001;10(2):118–123. doi: 10.1007/s005860000230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Blanco CR, Murillo RA, Velasco RV, Ramirez EM, Sotelo S, Fernández AS. Prevalencia de desviaciones del raquis en escolares del municipio de Talavera de la Reina y sus factores asociados. 2007. [Acesso em: 22/11/2007] http://sescam.jccm.es/web/gaptalavera/prof-investigacion/desviacionesRaquis.pdf
- 20.Alpalhão V, Robalo L. Algias vertebrais nos adolescentes: associação com as actividades de tempos livres auto-reportadas. Rev Essfisionline. 2005;2(1):3–15. [Google Scholar]
- 21.Detsch C, Luz AM, Candotti CT, Scotto de Oliveira D, Lazaron F, Guimarães LK, Schinanoski P. Prevalência de alterações posturais em escolares do ensino médio em uma cidade no Sul do Brasil. Rev Panam Salud Publica. 2007;21(4):231–238. doi: 10.1590/s1020-49892007000300006. [DOI] [PubMed] [Google Scholar]
- 22.Damasceno LH, Catarin SR, Campos AD, Defino HL. Lordose lombar: estudo dos valores angulares e da participação dos corpos vertebrais e discos inter-vertebrais. Acta Ortop Bras. 2006;14(4):193–198. [Google Scholar]
- 23.Kapandji AI. Fisiologia articular: tronco e coluna vertebral. 5a. ed. Guanabara Koogan; Rio de Janeiro: 2000. [Google Scholar]
- 24.Penha PJ, João SM, Casarotto RA, Amino CJ, Penteado DC. Postural assessment of girls between 7 and 10 years of age. Clinic (São Paulo) 2005;60(1):9–16. doi: 10.1590/s1807-59322005000100004. [DOI] [PubMed] [Google Scholar]
- 25.Martelli RC, Traebert J. Estudo descritivo das alterações posturais de coluna vertebral em escolares de 10 a 16 anos de idade. Tangará-SC, 2004. Rev Bras Epidemiol. 2006;9(1):87–93. [Google Scholar]
- 26.Giglio CA, Volpon JB. Development and evaluation of thoracic kyphosis and lumbar lordosis during growth. J Child Orthop. 2007;1(3):187–193. doi: 10.1007/s11832-007-0033-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Defino HL, Rodrigues-Fluentes E, Piola FP. Tratamento cirúrgico da cifose patológica. Acta Ortop Bras. 2002;10(1):10–16. [Google Scholar]
- 28.Correia PP, Silva GC, Nascimento JF, Lima NM, Sousa MS. Prevalência de desvios posturais em escolares da rede municipal de ensino na cidade de João Pessoa – PB, 2005. [Acesso em 12/04/2007] www.fef.unicamp.br/ccd/cd/trabalhos/temalivre/P%E9ricles%20Paes%20Barreto%20Correia.pdf
- 29.Mangueira JO. Prevalência de desvios na coluna vertebral ao exame físico em estudantes de 11 a 16 anos em uma escola do bairro Sinhá Sabóia – Sobral – CE/2004 [monografia]. Sobral: Universidade Estadual do Vale do Acaraú, Sobral/ CE; 2004
- 30.Bruschini S, Nery CA. Aspectos ortopédicos da obesidade na infância e adolescência. In: Fisberg M. Obesidade na infância e adolescência. São Paulo: Fundação Editorial BYK; 1995
- 31.Braccialli LMP, Vilarta R. Aspectos a serem considerados na elaboração de programas de prevenção e orientação de problemas posturais. Rev Paul Educ Física. 2000;14(2):159–171. [Google Scholar]