

Abstract
Objectives: To determine the prevalence of complications in a series of consecutive cases of hip arthroscopy; to assess the progression of the sample through a learning curve; and to recognize the causes of complications in arthroscopic hip operations. Method: 150 consecutive cases that underwent hip arthroscopy between May 2004 and December 2008 were evaluated. The complications encountered were classified in three ways: organic system affected, severity and groups of 50 consecutive cases. The data were analyzed by means of descriptive statistics and Fisher's exact test. Results: We observed 15 complications in this study (10%): ten were neurological, two were osteoarticular, one was vascular-ischemic and two were cutaneous. In the classification of severity, three were classified as major, 12 as intermediate and none as minor. The incidence of complications over the course of the learning curve did not present any statistically significant difference (p = 0.16). Conclusions: Hip arthroscopy is a surgical procedure that involves low morbidity, but which presents complications in some cases. These complications are frequently neurological and transitory, and mainly occur because of joint traction. The complication rate did not decrease with progression of our sample.
Keywords: Arthroscopy, Hip joint, Complications
INTRODUCTION
Arthroscopy is a surgical method that makes it possible to approach different joints in a minimally invasive manner and thus to diminish the morbidity caused by major procedures and enable early hospital discharge and shorter rehabilitation periods. Today, arthroscopic surgery is the orthopedic surgical procedure most commonly performed in the United States(1). Hip arthroscopy is indicated as a diagnostic and therapeutic method, and its indications include labral lesion, removal of free bodies from inside the joint and femoral-acetabular impaction, among others2, 3, 4, 5.
Reviews in the literature have cited variable complication rates. Some authors have cited rates ranging from 0.5 to 5%(2), while others have mentioned a range from 0.5 to 6.4%(3). Most studies have attributed the complications mainly to joint traction4, 5.
The aims of the present study were to determine the prevalence of complications in different arthroscopic procedures that are performed by means of hip arthroscopy, through a retrospective case series study on consecutive cases; to assess the evolution of our sample through a learning curve; and to recognize the causes of these complications.
METHODS
This was a retrospective study on a series of consecutive cases that included 150 patients who underwent hip surgery by means of arthroscopy between May 2004 and December 2008, regardless of the indication for such surgery. Among these patients, 69 (46%) were male and 81 (54%) were female. The patients' mean age was 37.25 years (range: 12 to 58 years). Regarding the hip side that underwent the surgical procedure, the right hip was more prevalent, accounting for 84 cases (56%), while the left hip was operated in 63 cases (42%); three patients (2%) underwent bilateral hip arthroscopy.
All of the patients were evaluated before and after the operation by the same observer, who carried out the surgical procedure.
All of the patients underwent general anesthesia. The position used for our sample was dorsal decubitus, in which the perineal post was positioned against the medial region of the thigh corresponding to the hip that underwent the surgical procedure, in order to generate a force vector of lateral direction. The hip that was to be operated was positioned with internal rotation of 20° and flexion of 10°, and adduction force was applied. The contralateral limb was positioned and placed under sufficient traction for the patient to be in equilibrium on the surgical table.
After positioning the patient, the limb that was to undergo the surgical procedure was placed under traction, with the aim of obtaining an increase in the intra-articular space, until the vacuum sign was apparent on radioscopy. Following this, distension of the joint capsule was induced by means of injecting saline solution (around 10 to 20 ml), using needle puncture. Throughout the procedure, we used a saline solution infusion pump at an initial pressure of 60 mmHg and maximum flow, in order to maintain the distension of the intra-articular space.
The hip arthroscopic procedure commonly used by our team involves four access ports, as described by Byrd(6): anterior, anterolateral, posterolateral and intermediate. However, in most of these cases, we only used two ports (anterior and anterolateral).
The data obtained in relation to complications from hip arthroscopy were analyzed in three ways: 1) type of complication (neurological, osteoarticular, vascular-ischemic and cutaneous); 2) severity, as described by Souza et al(7), who subdivided the complications into three categories of severity: major, i.e. complications that were definitive or necessitated surgical treatment for their correction; intermediate, i.e. transitory complications with complete recovery after clinical treatment; and lastly, minor, i.e. complications that were resolved during the surgical procedure; 3) incidence of complications over the course of building up the sample in a learning curve, subdividing the cases into groups of 50 patients, in order of occurrence of the surgical procedure.
We used descriptive statistics and Fisher's exact test to analyze the data. We considered the results to be statistically significant when p < 0.05.
This study was approved by the Research Ethics Committee of Hospital Governor Celso Ramos, at a meeting held on March 12, 2009, under no. 2008/0038.
RESULTS
We observed a total of 15 cases of complications (10%) in our series (Table 1). Among these, 10 were neurological, two were osteoarticular, one was vascular-ischemic and two were cutaneous. Grouping these complications according to their severity showed that three were major, 12 were intermediate and none of them were minor.
Table 1.
List of patients, their complications and other data gathered
| Case | Sex | Age | Side | Complication | Type | Severity |
|---|---|---|---|---|---|---|
| 9 | F | 41 | L | Pudendal neuropraxia | Neurological | Intermediate |
| 14 | F | 35 | R | Vulval edema | Vascular-ischemic | Intermediate |
| 35 | F | 46 | R | Dehiscence of suture | Cutaneous | Intermediate |
| 36 | F | 36 | R | Neuropraxia of pudendum | Neurological | Intermediate |
| 57 | M | 30 | R | Pudendal neuropraxia | Neurological | Intermediate |
| 79 | F | 50 | R | Instability | Osteoarticular | Severe |
| 80 | F | 24 | L | Sciatic neuropraxia | Neurological | Intermediate |
| 81 | F | 26 | R | Pudendal neuropraxia | Neurological | Intermediate |
| 87 | F | 35 | L | Permanent paresthesia of lower limbs | Neurological | Severe |
| 92 | M | 24 | L | Sciatic neuropraxia | Neurological | Intermediate |
| 98 | F | 49 | R | Instability | Osteoarticular | Severe |
| 107 | F | 26 | L | Sciatic neuropraxia | Neurological | Intermediate |
| 112 | F | 31 | L | Sciatic neuropraxia | Neurological | Intermediate |
| 122 | F | 31 | L | Sciatic neuropraxia | Neurological | Intermediate |
| 123 | F | 25 | R | Dehiscence of suture | Cutaneous | Intermediate |
Among the major complications, there were two cases of dysplastic hips that progressed to instability and were then treated by means of total hip arthroplasty (osteoarticular complications) and another case that presented permanent paresthesia of the lower limbs, without any improvement after two years of follow-up (neurological complication). Among the intermediate complications, the most common were neurological, among which perineal neuropraxia occurred most frequently, with eight cases (5.33% of our sample). Also in relation to the intermediate neurological complications, one patient (0.6% of our series) presented neuropraxia of the sciatic nerve, with motor improvement after three days and sensory improvement after four months. There was one case (0.6% of our patients) of vascular-ischemic complication among the intermediate-severity cases, consisting of transitory edema of the vulva. The group of intermediate-severity complications included two cases (1.33% of our cases) of cutaneous complications, consisting of dehiscence of the suture, and these presented improvement after clinical treatment (Figure 1).
Figure 1.
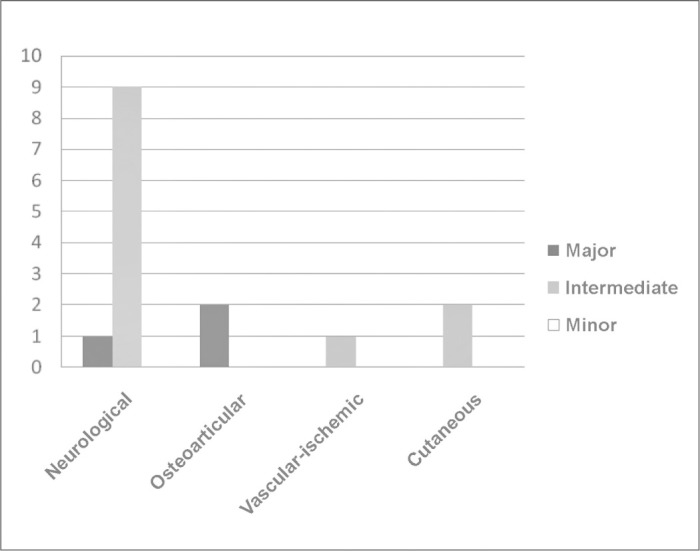
Frequency of complications, classified according to organic system affected and severity
We did not observe any cases of deep vein thrombosis, deep infection, labral lesion, chondral lesion or joint capsule injury. Nor were there any cases of breakage of surgical instruments.
Regarding the organic systems affected in each of the groups, we observed that group 1 presented two cases of neurological complications, one of vascular-ischemic complication and one of cutaneous complication. In group 2, there were five cases of neurological complications and two of osteoarticular complications. In group 3, there were three cases of neurological complications and one of cutaneous complication (Figure 2)
Figure 2.
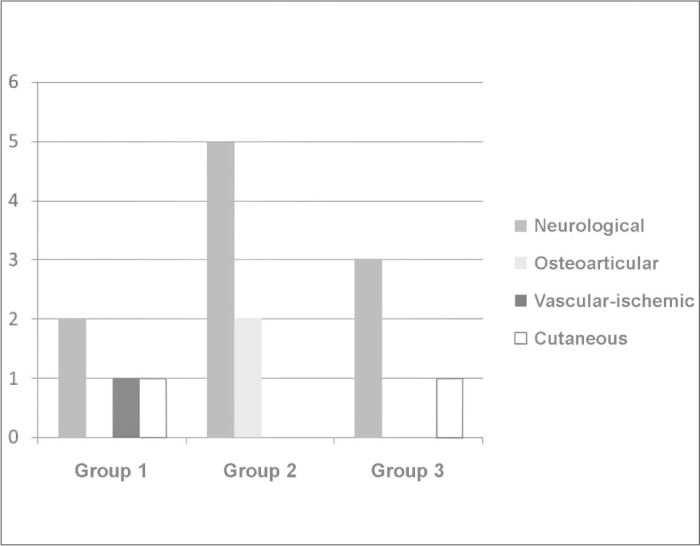
Frequency of complications, according to organic system affected during the learning curve
STATISTICAL ANALYSIS
We divided our series into three groups of 50 patients, according to the order in which the surgical procedure was performed. There were four intermediate complications in each of the groups and three major complications in group 2. We did not find any statistically significant differences between the numbers of complications in groups 1 and 2 (p = 0.16) or between groups 2 and 3 (p = 0.16). Thus, there were no statistically significant differences in the numbers of complications over the course of our learning curve, even though group 2 had an absolute number of complications (seven) that was greater than in the other two groups (Figure 3).
Figure 3.
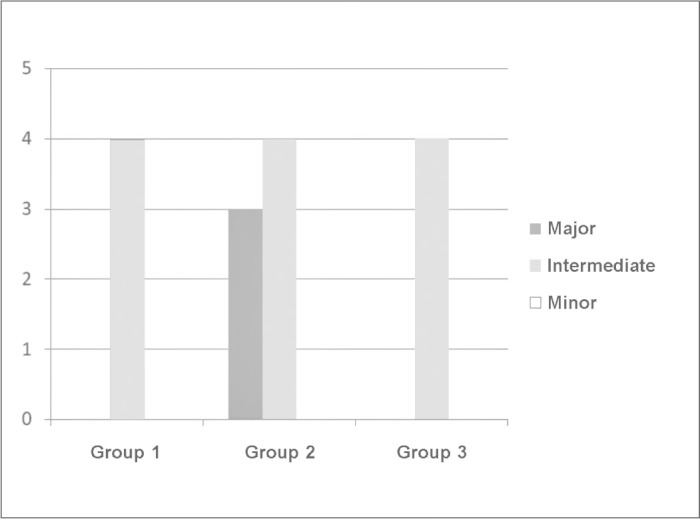
Frequency of complications, according to the learning curve.
DISCUSSION
In a review of the literature, McCarthy and Lee(2) cited a complication rate ranging from 0.5 to 5% in hip arthroscopic procedures, while Smart et al(3) presented a rate ranging from 0.5 to 6.4%. Both of these authors stated that neuropraxia was the most common complication. The complications that occur during hip arthroscopy relate mainly to joint traction and construction of ports(4). Rodeo et al(5) showed that neurological lesions occurred through direct injury caused by incorrect location of the ports, excessive traction force or compression from the perineal post.
We noted that 11 of the complications in our series (73.33% of our total) were attributable to traction. One of the cases was considered severe because of the persistence of paresthesia of the lower limbs throughout the follow-up period (two years), even though this patient presented normal electromyography findings. Kim et al(8) reported one case of reflex sympathetic dystrophy following hip arthroscopy that did not present resolution after two years of follow-up.
Another nine patients presented transitory neuropraxia and were considered intermediate in the severity classification because their condition improved with clinical treatment. Funke and Munzinger(9) observed one case of transitory neuropraxia; Sampson(10), in a study on 1,001 patients, presented 20 cases of transitory neuropraxia; Griffin and Villar(11), in an analysis on 640 consecutive cases, presented four episodes of transitory neuropraxia; Clarke et al(4), among 1,054 consecutive cases, reported four cases of neuropraxia; Souza et al(7) presented five cases of transitory neuropraxia; Byrd and Jones(12) observed one case of transitory neuropraxia in a study involving 38 arthroscopic procedures on a sample of 35 patients; Kim et al(8) reported four cases presenting transitory neuropraxia; and Dienst et al(13), in a series of hip arthroscopies in the peripheral compartment without using traction, presented one case of transitory neuropraxia. It is important to emphasize that McCarthy and Lee(2), in their review of the literature signaled that the most important preventive measures for avoiding neurological lesions are correct positioning of the patient and adequate traction.
Another case of complication related to traction that we observed was one of vulval edema, which was our only case of vascular-ischemic complication; this was considered to be of intermediate severity. This event occurred when we had a shortage of the perineal protection foam that we routinely use and therefore used another type of foam for perineal protection. Funke and Munzinger(9) reported a case of hematoma in the labia majora; Clarke et al(4) observed a case of vaginal lesion; Griffin and Villar(11) presented a case of lesion in the vaginal region; Souza et al(7) described an episode of vulval edema that they considered to be an intermediate complication, and a case of partial necrosis of the scrotal skin, which they considered to be a severe complication and corrected by means of plastic surgery.
In our series, we noted that two cases of complications (13.33% of the complications) were related to the surgical ports. These were classified as cutaneous. Both of them presented in the form of dehiscence of the suture, and we classified them as intermediate complications because of their benign evolution after clinical treatment. We did not find any reports of superficial infection in the literature. This may have been because this complication might not be attributed solely to the hip arthroscopy but, rather, to surgical procedures in general. Several authors have reported other intercurrences relating to access ports. Clarke et al(4) observed two cases of bleeding and two cases of hematoma in access ports; Griffin and Villar(11) reported one case of bleeding in an access port and one case of hematoma in the operative wound.
In our study, we did not have any cases of deep infection. Clarke et al(4) reported one case of septic arthritis, in which clindamycin-sensitive Staphylococcus aureus was the etiological agent, 26 days after performing hip arthroscopy to treat osteochondromatosis.
We observed two cases of osteoarticular complications (13.33% of our cases) in our study. Both of these were in patients who underwent the arthroscopic procedure because of hip dysplasia. These two patients progressed to instability and then underwent total hip arthroplasty to correct the problem. We believe that neither of these case had an appropriate indication for arthroscopy. Some researchers might consider this to be a poor result and not a complication, and for this reason, such cases may not have been reported in other series.
With regard to osteoarticular complications, Sampson(10) reported three cases of iatrogenic lesions in joint cartilage that were attributed to inappropriate traction: one of avascular necrosis of the femoral head, resulting from a disorder of the medial circumflex femoralartery; one of fracture of the femoral neck caused by major resection of the femoral neck; and, later on, one case of heterotopic ossification. In a study on cadavers, Sussmann et al(14) showed that the medial circumflex femoral artery was protected by the greater trochanter when a posterolateral port was used; Griffin and Villar(11) presented a case of trochanteric bursitis that responded to treatment with corticoid injection. Clarke et al(4) also reported a case of trochanteric bursitis that presented resolution after local corticoid therapy was used. Souza et al(7) reported two cases of complications relating to the osteoarticular system: one patients who underwent hip arthroscopy because of femoral-acetabular impaction and progressed to hip instability, which necessitated total hip arthroplasty to resolve the situation (which the authors considered to be a major complication); and another patient who underwent an arthroscopic procedure because of femoral-acetabular impaction and suffered a fracture due to stress on the femoral neck, without deviation, which was treated conservatively and evolved to consolidation after eight weeks (which the authors classified as an intermediate complication). In a study on hip arthroscopy in the peripheral compartment without using traction, Dienst et al(13) presented three cases of joint cartilage lesion, one case of osteophyte release (resolved during the procedure) and ten cases of partial lesions of the joint capsule.
In our series, we did not observe any cases of extravasation of fluid into the retroperitoneal or abdominal space. Sampson(10) observed ten cases of extravasation of fluid into the abdominal cavity; Barlett et al(15) reported one case of extravasation of fluid into the abdominal cavity in large quantity, which was attributed to fracturing of the acetabulum and resulted in cardiorespiratory arrest. This patient only became hemodynamically stabilized after extraction of some of the liquid from the cavity.
We did not recognize any cases of deep vein thrombosis among our sample. Souza et al(7) observed one case of deep vein thrombosis that presented full recovery without sequelae, after clinical treatment. McCarthy and Lee(2) reported a case of deep vein thrombosis one month after the operation in a patient with factor V Leiden deficiency. In a review that included more than 5,500 cases, Bushnell et al(16) did not find any cases of deep vein thrombosis and did not find any specific recommendations for prophylaxis against this event.
We did not observe any cases of breakage of surgical instruments in our series. Sampson(10) reported three occurrences of instrument breakage; Griffin and Villar(11) reported two such cases; Clarke et al(4) presented two such cases; and Souza et al(7) observed two cases of breakage of surgical materials, which they considered to be minor complications because they were resolved during the procedure.
Contrary to what Sampson(10) reported, but corroborating what Souza et al(7) observed, we did not recognize any decrease in the complication rate as our sample inclusion continued. This may have been due to the increasing complexity of the arthroscopic procedures performed by our team, despite the evolution of hip arthroscopy techniques and the equipment used for the surgical procedure. Although there were no statistically significant differences in the numbers of complications during our learning curve, the period between cases 51 and 100 presented the greatest absolute number of complications (seven), and three of these were major complications. It seems that the surgeon became more daring and may have inappropriately indicated the technique for some cases, in an attempt to take greater steps towards improving the technique.
Furthermore, few series have included each author's first cases. In our review, only three papers did so: Sampson(10), Clarke et al(4) and Souza et al(7). In the other series, there is no mention of whether or not the initial cases were included.
Hip arthroscopy is a new surgical tool that has been shown to be safe and effective. With correct indication, well-selected patients and greater experience on the part of the surgeon, the tendency will be for the complication rate to diminish further, thus making this method the best option for treating intra-articular pathological conditions of the hip.
CONCLUSIONS
Hip arthroscopy is a surgical procedure that makes it possible to approach this joint in a minimally invasive manner, but it proceeds with certain complications. These complications are frequently neurological and transitory. They occur mainly because of joint traction that is performed with the aim of increasing the intra-articular space.
Our complication rate did not present any decrease with the evolution of our sample, and is in line with findings in the literature.
Footnotes
Work performed at Hospital Governor Celso Ramos, Florianópolis, SC
REFERENCES
- 1.Villar RN. Arthroscopy. BMJ. 1994;308(6920):51–53. doi: 10.1136/bmj.308.6920.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.McCarthy JC, Lee JA. Hip arthroscopy: indications, outcomes, and complications. Bone Joint Surg Am. 2005;87:1138–1145. [Google Scholar]
- 3.Smart LR, Oetgen M, Noonan B, Medvecky M. Beginning hip arthroscopy: indications, positioning, portals, basic techniques, and complications. Arthroscopy. 2007;23(12):1348–1353. doi: 10.1016/j.arthro.2007.06.020. [DOI] [PubMed] [Google Scholar]
- 4.Clarke MT, Arora A, Villar RN. Hip arthroscopy: complications in 1054 cases. Clin Orthop Relat Res. 2003;(406):406–408. doi: 10.1097/01.blo.0000043048.84315.af. [DOI] [PubMed] [Google Scholar]
- 5.Rodeo SA, Forster RA, Weiland AJ. Neurological complications due to arthroscopy. J Bone Joint Surg Am. 1993;75(6):917–926. doi: 10.2106/00004623-199306000-00015. [DOI] [PubMed] [Google Scholar]
- 6.Byrd JW. Operative hip arthroscopy. 2nd ed. Springer; New York: 2004. [Google Scholar]
- 7.Souza BGS, Polesello G, Honda E, Ono NK, Guimaraes RP, Ricioli W. Complications in hip arthroscopy. In: Annual Meeting Podium Presentations; 2009, Fevereiro 25-27; Las Vegas, EUA: American Association of Orthopaedic Surgeons.
- 8.Kim SJ, Choi NH, Kim HJ. Operative hip arthroscopy. Clin Orthop Relat Res. 1998;(353):353–365. doi: 10.1097/00003086-199808000-00018. [DOI] [PubMed] [Google Scholar]
- 9.Funke EL, Munzinger U. Complications in hip arthroscopy. Arthroscopy. 1996;12(2):156–159. doi: 10.1016/s0749-8063(96)90004-3. [DOI] [PubMed] [Google Scholar]
- 10.Sampson TG. Complications of hip arthroscopy. Tech Orthop. 2005;20(1):63–66. [Google Scholar]
- 11.Griffin DR, Villar RN. Complications of arthroscopy of the hip. J Bone Joint Surg Br. 1999;81(4):604–606. doi: 10.1302/0301-620x.81b4.9102. [DOI] [PubMed] [Google Scholar]
- 12.Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy. 2000;16(6):578–587. doi: 10.1053/jars.2000.7683. [DOI] [PubMed] [Google Scholar]
- 13.Dienst M, Gödde S, Seil R, Hammer D, Kohn D. Hip arthroscopy without traction: in vivo anatomy of the peripheral hip joint cavity. Arthroscopy. 2001;17(9):92431. doi: 10.1053/jars.2001.25342. [DOI] [PubMed] [Google Scholar]
- 14.Sussmann PS, Zumstein M, Hahn F, Dora C. The risk of vascular injury to the femoral head when using the posterolateral arthroscopy portal: cadaveric investigation. Arthroscopy. 2007;23(10):1112–1115. doi: 10.1016/j.arthro.2007.05.014. [DOI] [PubMed] [Google Scholar]
- 15.Barlett CS, DiFelice GS, Buly RL, Quinn TJ, Green DST, Helfet DL. Cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopy removal of a loose body from the hip joint of a patient with an acetabular fracture. J Orthop Trauma. 1998;12(4):294–299. doi: 10.1097/00005131-199805000-00014. [DOI] [PubMed] [Google Scholar]
- 16.Bushnell BD, Anz AW, Bert JM. Venous thromboembolism in lower extremity arthroscopy. Arthroscopy. 2008;24(5):604–611. doi: 10.1016/j.arthro.2007.11.010. [DOI] [PubMed] [Google Scholar]