

Summary
Background
The safety and efficacy of continuous, multiday, automated glycaemic management has not been tested in outpatient studies of preadolescent children with type 1 diabetes. We aimed to compare the safety and efficacy of a bihormonal bionic pancreas versus conventional insulin pump therapy in this population of patients in an outpatient setting.
Methods
In this randomised, open-label, crossover study, we enrolled preadolescent children (aged 6–11 years) with type 1 diabetes (diagnosed for ≥1 year) who were on insulin pump therapy, from two diabetes camps in the USA. With the use of sealed envelopes, participants were randomly assigned in blocks of two to either 5 days with the bionic pancreas or conventional insulin pump therapy (control) as the first intervention, followed by a 3 day washout period and then 5 days with the other intervention. Study allocation was not masked. The autonomously adaptive algorithm of the bionic pancreas received data from a continuous glucose monitoring (CGM) device to control subcutaneous delivery of insulin and glucagon. Conventional insulin pump therapy was administered by the camp physicians and other clinical staff in accordance with their established protocols; participants also wore a CGM device during the control period. The coprimary outcomes, analysed by intention to treat, were mean CGM-measured glucose concentration and the proportion of time with a CGM-measured glucose concentration below 3·3 mmol/L, on days 2–5. This study is registered with ClinicalTrials.gov, number NCT02105324.
Findings
Between July 20, and Aug 19, 2014, 19 children with a mean age of 9·8 years (SD 1·6) participated in and completed the study. The bionic pancreas period was associated with a lower mean CGM-measured glucose concentration on days 2–5 than was the control period (7·6 mmol/L [SD 0·6] vs 9·3 mmol/L [1·7]; p=0·00037) and a lower proportion of time with a CGM-measured glucose concentration below 3·3 mmol/L on days 2–5 (1·2% [SD 1·1] vs 2·8% [1·2]; p<0·0001). The median number of carbohydrate interventions given per participant for hypoglycaemia on days 1–5 (ie, glucose <3·9 mmol/L) was lower during the bionic pancreas period than during the control period (three [range 0–8] vs five [0–14]; p=0·037). No episodes of severe hypoglycaemia were recorded. Medium-to-large concentrations of ketones (range 0·6–3·6 mmol/dL) were reported on seven occasions in five participants during the control period and on no occasion during the bionic pancreas period (p=0·063).
Interpretation
The improved mean glycaemia and reduced hypoglycaemia with the bionic pancreas relative to insulin pump therapy in preadolescent children with type 1 diabetes in a diabetes camp setting is a promising finding. Studies of a longer duration during which children use the bionic pancreas during their normal routines at home and school should be done to investigate the potential for use of the bionic pancreas in real-world settings.
Funding
The Leona M and Harry B Helmsley Charitable Trust and the US National Institute of Diabetes and Digestive and Kidney Diseases.
Introduction
Maintaining glycaemia near the normal range is effective in preventing long-term complications in individuals with type 1 diabetes,1–3 but is challenging to achieve4–6 and is associated with frequent hypoglycaemia, which can be life threatening.7–11 Safe glycaemic control is especially challenging in children who cannot take responsibility for their own care and might not communicate symptoms associated with hyperglycaemia and hypoglycaemia. Additionally, the effect of insulin dosing errors can be more serious in children than in adults because of their lower body mass. Parents are challenged by the management of their children’s diabetes and can have substantial anxiety, especially overnight and when their children are not under their care. Only 14% of children meet the glycaemic target set by the American Diabetes Association (HbA1c <7·5%), compared with 30% of adults (HbA1c <7·0%).5,6 Better methods are therefore needed to manage glycaemia in children with diabetes. One promising strategy is to automate glycaemic management with a bihormonal bionic pancreas that uses continuous glucose monitoring (CGM) and mathematical algorithms to measure blood glucose concentrations and administer required doses of insulin and glucagon.12,13
The results of our previous day-and-night studies13 showed that automated glycaemic regulation can significantly improve glycaemic control in real-world outpatient settings where no restrictions were placed on diet or exercise.13 In these studies, the bihormonal bionic pancreas significantly reduced mean blood glucose concentrations and hypoglycaemia or the need to treat hypoglycaemia in adults and adolescents older than 12 years.13 Subsequently, reports have been published of outpatient day-and-night studies assessing four other glucose control systems (three insulin-only and one bihormonal) in adults or adolescent children.14–17 No outpatient day-and-night studies in preadolescent children have previously been reported.
In this study, we aimed to compare the efficacy and safety of a bihormonal bionic pancreas with that of conventional insulin pump therapy in preadolescent children aged 6–11 years with type 1 diabetes in an outpatient diabetes camp setting where no limitations were placed on diet or exercise.
Methods
Study design and participants
In this randomised, open-label, outpatient crossover trial, we recruited participants aged 6–11 years who were attending two diabetes camps (Camp Joslin or the Clara Barton Camp) operated by the Barton Center for Diabetes Education in North Oxford, MA, USA. Children stayed overnight at the camps, and all participants had to be attending for at least two contiguous weeks. Eligible participants were those who had been diagnosed with type 1 diabetes for 1 year or longer and were on insulin pump therapy.
Key exclusion criteria were cystic fibrosis, seizure disorder, eating disorder or omission of insulin to manipulate weight, history of intentional inappropriate administration of insulin, heart disease, and end-stage renal or liver failure. A full list of exclusion criteria are included in the protocol (appendix). Participants received financial compensation for their participation.
The protocol (appendix) was approved by the Massachusetts General Hospital and Boston University Human Research Committees, and the trial was monitored by a data safety and monitoring board who were not masked to treatment allocation. All participants provided written assent, with informed consent also provided by a parent or guardian.
Randomisation
Participants were randomly assigned (1:1) to use the bihormonal bionic pancreas first, followed by conventional insulin pump therapy, or to use conventional insulin pump therapy first, followed by the bihormonal bionic pancreas. Randomisation was done in blocks of two using sealed envelopes produced by MAH that were shuffled (in pairs, by one person, then again by another) and opened in the same order by KLM once participants were found to be eligible. KLM and MAH were also involved in collating, and analysing the data. Participants, investigators, and camp staff were not masked to allocation assignment.
Procedures
All participants received insulin via the bionic pancreas for 5 days (bionic pancreas period) and via their own insulin pump under supervision of camp staff for 5 days (control period), in the order assigned at randomisation, with a 3 day washout period in between.
The processes by which insulin and glucagon were administered by the fully automated bihormonal bionic pancreas have been described previously.13 The device consisted of an iPhone 4S (Apple, Cupertino, CA, USA) that ran the control algorithm in an app, and was connected to a G4 Platinum CGM system (DexCom, San Diego, CA, USA) via a custom hardware interface. The control algorithm received CGM data and calculated the required doses of insulin and glucagon that were then automatically delivered subcutaneously through insulin infusion sets every 5 min by t:slim infusion pumps (Tandem Diabetes Care, San Diego, CA, USA). The user interface allowed the user to tell the device when a certain meal type, such as breakfast, lunch, or dinner, was about to be consumed, and what the meal size was going to be, such as typical, more than usual, less than typical, or a small bite. Parents specified what range of carbohydrate content constituted a typical amount of carbohydrates for their child for each meal type and size (eg, 50–80 g of carbohydrate might be typical for breakfast for a particular child). For all meal types other than snacks, camp staff selected the meal type and size category on the bionic pancreas user interface 5–15 min before each meal, which was the same time as when meal boluses were administered to participants during the control period. The first time the bionic pancreas was used in each participant, a partial meal-priming bolus based on the participant’s body mass (0·05 units/kg) was delivered. After the first use, the size of the meal-priming bolus was adapted by the bionic pancreas to 75% of the 4 h prandial insulin used for that meal type and size.
The system was initialised using only the participant’s body mass; no information about the participant’s usual insulin regimen was provided to the algorithm. During operation of the device, the only external inputs were meal type, meal size, and CGM calibration, which was done twice daily before breakfast and dinner and as requested by the CGM system. The bionic pancreas automatically adapted insulin dosing to each individual’s needs. When CGM data were not available (because of sensor failure or during the warm-up time after sensor replacement), the bionic pancreas automatically delivered a dose of basal insulin based on the mean basal dosing it had calculated at that time on previous days. Automatic correction doses of insulin or glucagon were delivered in response to manually entered fingerstick plasma glucose concentrations, which were required once per h when sensor data were not available. If the CGM system went offline, the control algorithm would then respond to these plasma glucose values as if they were CGM values, calculating the required doses of insulin or glucagon as it would if the same CGM value had been received (appendix). The system automatically regulated any glycaemic excursion that resulted from failed sensors and infusion sets after their replacement. No insulin was given other than by the bionic pancreas. Patients were not allowed to take paracetamol because of the possible interference with CGM.18 Participants and study staff were not masked to CGM data while the bionic pancreas was in use, but a password was required to access the user interface and the CGM data. To prevent any inappropriate meal types being inputted, participants were not given the password to the device.
During the control period, participants used a CGM or device connected to an iPhone to allow remote monitoring of device functioning and severe biochemical hypoglycaemia by the study staff, and their own insulin pump. Participants who used CGM as part of their usual care were encouraged to use their personal CGM device during the control period in addition to the CGM device provided by the study for the control period. During the control period, the insulin regimens of participants were adjusted daily by a camp physician in accordance with standard camp guidelines and the judgment of the physician, without any interaction with study staff. The camp guidelines are included in the study protocol (appendix), but were not modified in any way during the study period.
Participants stayed in the same cabins, engaged in the same activities, and ate the same meals as non-participant campers. During both study periods, telemetric monitoring staff located on the camp grounds alerted clinical study staff by telephone when CGM-measured glucose concentrations dropped below 3·3 mmol/L for more than 15 min. By contrast with our previous camp study,13 staff responsible for remote monitoring were masked to specific CGM glucose concentrations (they could not see the CGM trace or values, only a flag indicating that CGM glucose was <3·3 mmol/L) and were masked to insulin and glucagon dosing by the bionic pancreas. Telemetric monitors also alerted study staff to when the CGM system or the insulin or glucagon pumps were disconnected for 15 min during bionic pancreas use.
During both the bionic pancreas and control periods, all CGM alarms were silenced, apart from a low-threshold alarm at a glucose concentration of 2·8 mmol/L (50 mg/dL) that could not be silenced. Fingerstick plasma glucose measurements were obtained (StatStrip Xpress, Nova Biomedical, Waltham, MA, USA) before meals, at bedtime, at midnight, and at about 0345 h (six scheduled measurements), before swimming or showering, and if a participant had symptoms of hypoglycaemia. In accordance with camp policy, participants were given 15 g of simple carbohydrates if their plasma glucose concentration dropped below 4·4 mmol/L. These simple carbohydrates were counted as interventions for study outcomes if the plasma glucose concentration was less than 3·9 mmol/L. A second intervention of 15 g of carbohydrate was given if a repeat measurement in 15–20 min was less than 3·9 mmol/L. Once the plasma glucose concentration was greater than 3·9 mmol/L, the participant was given a snack of 15 g of complex carbohydrates unless a meal was scheduled within 1 h. Real-time CGM traces were not monitored, and participants did not have access to CGM data on their devices, because they were locked with a password. Therefore, CGM data could not be used to predict hypoglycaemic events or to treat any events pre-emptively. Camp staff did not use study CGM data from participants using the bionic pancreas to make any treatment decisions, although they could use data from a participant’s personal CGM system to do so (during the control period) if the participant happened to be wearing their personal CGM system.
To assess safety, data for episodes of ketonaemia were collected from the camp medical charts of the participants. Data for infusion set changes during the control period were collected from the camp medical chart, and during the bionic pancreas period they were collected from the camp medical chart and documentation by study staff. Participants completed a questionnaire each evening that asked whether they had had any nausea that day, and if so, to report its intensity on a 10 cm visual analogue scale (appendix).
Outcomes
The coprimary outcomes were mean glucose con centration as measured by the CGM system on days 2–5 of each period, and the mean proportion of time that the CGM-measured glucose concentration was less than 3·3 mmol/L on days 2–5 of each period. Initial adaptation by the bionic pancreas to the insulin needs of the individual is typically completed by the end of day 1.19 Although the same process continues as part of normal operation, days 2–5 are expected to be more representative of long-term system performance than day 1.
Prespecified secondary outcomes included the proportion of time that CGM-measured glucose concentrations were in clinically relevant ranges, the mean of scheduled plasma glucose concentration measure ments, the proportion of scheduled plasma glucose concentration measurements that were below 3·3 mmol/L, the number of carbohydrate interventions for hypoglycaemia per day (irrespective of carbohydrate amount given), and the amount (in grams) of carbohydrate given for hypoglycaemia. For the purposes of this analysis, carbohydrates consumed when an individual had a plasma glucose concentration of 3·9–4·4 mmol/L were counted as unscheduled snacks. Additional prespecified secondary outcomes included the proportion of participants with a mean CGM-measured glucose concentration of 8·6 mmol/L or lower, 9·4 mmol/l or lower, and 10·2 mmol/L or lower (which correspond to HbA1c of about 7%, 7·5%, and 8%, respectively20–22). Outcome measures associated with mean CGM-measured glucose concentrations, the proportion of time in the aforementioned CGM-measured glucose ranges (≤8·6 mmol/L, ≤9·4 mmol/l, and ≤10·2 mmol/L), and the number of carbohydrate interventions were calculated for both the night-time period (2300 h to 0700 h) and the full 24 h day. To quantify adaptation by the bionic pancreas, we compared results from day 1 with days 2–5. The mean of daily differences was calculated as described in previously published studies.23,24 Two prespecified outcomes that we calculated on the basis of scheduled plasma glucose measure ments—the number of hypoglycaemic events captured by plasma glucose measurements and the number of participants with mean plasma glucose concentrations below the estimated average glucose-concentration thresholds—are not reported here because we thought that the CGM-measured data for these outcomes were more reliable in view of the low frequency of scheduled plasma glucose measurements (maximum of 20 possible measurements over 5 days). A full list of all secondary and other prespecified endpoints are listed in the protocol (appendix).
Statistical analysis
In our previous camp study in adolescents,13 the difference between the mean CGM-measured glucose concentrations during the bionic pancreas and control periods was 0·9 mmol/L (7·9 mmol/L [SD 0·7] with bionic pancreas vs 8·8 mmol/L [1·5] with control). Our power analysis predicted that, assuming the same variance in mean CGM-measured glucose concentration among participants, a sample size of 24 participants would be required to detect a 0·9 mmol/L difference in mean glycaemia between periods, with a power of 80% and a p value of 0·05, using a one-sided t test (superiority analysis). Therefore, we aimed to enrol 12 boys and 12 girls.
We included all data from each participant in the efficacy and safety analyses, according to the intention-to-treat principle. We calculated mean CGM-measured glucose concentrations as the mean of all CGM-measured concentrations (measured every 5 min) over the study period. We assessed the normality of the paired difference for each outcome with the Shapiro–Wilk test. The prespecified analysis plan was to use the paired-sample Student’s t test to compare study groups for outcomes with normally distributed data, and the Wilcoxon signed rank test to compare study groups for outcomes with non-normally distributed data. For normally distributed outcomes, we have reported means and SDs, and for non-normally distributed outcomes we have reported medians and ranges.
For the two coprimary outcomes, we additionally used a repeated-measurements model to analyse the period effects (ie, differences between the first 5 days of study treatment compared with the second 5 days of treatment) and treatment effects (ie, differences between the bionic pancreas and control periods), and used the interaction between them to test for a carryover effect. We also used multivariable models to analyse the effect of baseline HbA1c on the coprimary outcomes. We analysed prespecified secondary outcomes with univariate analysis only. We used the exact McNemar’s test to assess the significance of the difference in the incidence of ketosis between the two study groups. We report nominal p values for all outcomes, and we did not do adjustment for multiple comparisons. We analysed data using Microsoft Excel for Mac 2011, version 14.6.0, and SAS, version 9.4.
This study is registered with ClinicalTrials.gov, number NCT02105324.
Role of the funding source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. FHE-K, ERD, and SJR had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
Between July 20, 2014, and Aug 19, 2014, we enrolled and assessed 19 children who were planning to attend the Joslin (boys) or Clara Barton (girls) diabetes camps, all of whom completed the study protocol (figure 1).
Figure 1.
Trial profile
Fewer than the target number of boys were enrolled in the study as a result the low enrolment of boys aged 6–11 years in the camp session during which the study took place (table 1).
Table 1.
Baseline characteristics
| N (%) or mean (SD) | Range | |
|---|---|---|
| Sex | ||
| Boys | 6 (32%) | NA |
| Girls | 13 (68%) | NA |
|
| ||
| Age, years | 9·8 (1·6) | 6·5 to 11·9 |
|
| ||
| Body mass, kg | 35 (7·6) | 21·0 to 53·0 |
|
| ||
| BMI (kg/m²) | 17·8 (2·1) | 14·2 to 24·0 |
|
| ||
| BMI Z score | 0·4 (0·6) | −0·5 to 1·6 |
|
| ||
| Diabetes duration, years | 5·0 (2·2) | 1·8 to 9·1 |
|
| ||
| Daily insulin dose, units/kg | 0·74 (0·15) | 0·50 to 1·02 |
|
| ||
| HbA1c, % | 7·8 (0·8) | 6·5 to 9·2 |
|
| ||
| Estimated average glucose concentration*, mmol/L | 9·8 (1·3) | 7·8 to 12·1 |
During the bionic pancreas period, participants had a lower mean CGM-measured glucose concentration on days 2–5 than during the control period (7·6 mmol/L [SD 0·6] vs 9·3 mmol/L [1·7]; p=0·00037) in the prespecified univariate analysis (table 2; figure 2A). After adjustment for period effect in a multivariable model, mean CGM-measured glucose concentrations were 1·7 mmol/L (SD 0·3; 95% CI 1·1–2·4) lower during the bionic pancreas period than during the control period (p<0·0001). We noted a significant period effect, with the mean CGM-measured glucose concentration higher, by 0·9 mmol/L (95% CI 0·2–1·5; p=0·018), in the second period relative to the first period, with no interaction between period and treatment effect (pinteraction=0·44). Baseline HbA1c had no effect (pinteraction=0·18). During the bionic pancreas period, participants spent a lower mean proportion of time with a glucose concentration below 3·3 mmol/L on days 2–5 than did the control group, in the prespecified univariate analysis (1·2% [SD 1·1] vs 2·8% [1·2]; p<0·0001; table 2, figure 2A). Analysis of the mean proportion of time that glucose concentrations were less than 3·3 mmol/L (ie, hypoglycaemia) with a multivariable model revealed a carryover effect (p=0·016). Therefore, we did a comparison of hypoglycaemia in the first period only and identified a mean reduction in the mean proportion of time spent with glucose concentrations less than 3·3 mmol/L in the bionic pancreas period versus the control period of 2·6% (SD 0·35; 95% CI 1·9–3·3; p<0·0001).
Table 2.
Glucose concentrations measured by CGM and fingerstick testing during 24 h day and night only
| Bionic pancreas (n=19) | Control (n=19) | Unadjusted p value | |
|---|---|---|---|
|
Day and night
| |||
| Glucose concentration measured by CGM device on days 2–5 | |||
| Mean, mmol/L* | 7·6 (0·6) | 9·3 (1·7) | 0·00037 |
| <3·3 mmol/L, % of time | 1·2% (1·1) | 2·8% (1·2) | <0·0001 |
| 3·9–10 mmol/L, % of time | 80·6% (7·4) | 57·6% (14·0) | <0·0001 |
| >10 mmol/L, % of time | 16·5% (6·4) | 36·3% (15·7) | <0·0001 |
| SD, mmol/L† | 2·8 (0·9) | 4·2 (1·0) | <0·0001 |
| Coefficient of variation, % | 37% (9) | 45% (8) | 0·0017 |
| Mean of daily differences, mmol/L/day | 0·8 (0·5) | 2·1 (1·3) | 0·00083 |
| Plasma glucose concentration measured by fingerstick testing on days 1–5 | |||
| Mean, mmol/L | 7·6 (0·4) | 9·8 (1·4) | <0·0001 |
| <3·3 mmol/L, % of time | 0% (0–6·7) | 3·3% (0–6·7) | 0·065‡ |
| Number of carbohydrate interventions per participant on days 1–5§ | 3 (0–8) | 5 (0–14) | 0·037‡ |
|
| |||
|
Night only
| |||
| Glucose concentration measured by CGM device on nights 2–5 | |||
| Median, mmol/L¶ | 6·8 (5·7–7·6) | 9·4 (6·6–14·6) | <0·0001‡ |
| <3·3 mmol/L, % of time | 0·6% (0·8) | 2·8% (2·7) | 0·0027 |
| 3·9–10 mmol/L, % of time | 91·9% (7·3) | 58·8% (17·4) | <0·0001 |
| >10 mmol/L, % of time | 6·4% (6·4) | 36·5% (18·3) | <0·0001 |
| SD, mmol/L† | 1·7 (0·5) | 3·5 (1·3) | <0·0001 |
| Coefficient of variation, % | 25% (6) | 35% (9) | 0·00024 |
| Plasma glucose concentration measured by fingerstick testing on days 1–5 | |||
| Mean, mmol/L | 7·6 (0·7) | 9·8 (1·8) | <0·0001 |
| <3·3 mmol/L, % of time | 0% (0–0) | 0% (0–10·0) | 0·031‡ |
| Number of carbohydrate interventions per participant on days 1–5§ | 0 (0–1) | 1 (0–4) | 0·0020‡ |
Data are mean (SD) for normally distributed date and median (range) for non-normally distributed data, unless otherwise specified. CGM=continuous glucose monitoring.
Mean (SD) of each participant’s mean of all their 5 min CGM-measured concentrations during the study period.
Mean (SD) of each participant’s SD of all their 5 min CGM-measured concentrations during the study period.
Non-normally distributed data; p value from Wilcoxon signed rank test.
Given when glucose concentrations were below 3·9 mmol/L.
Median (range) of each participant’s mean of all their 5 min CGM-measured concentrations during the study period.
Figure 2. Mean and cumulative CGM-measured glucose concentrations during the bionic pancreas and control periods, and by time of day.
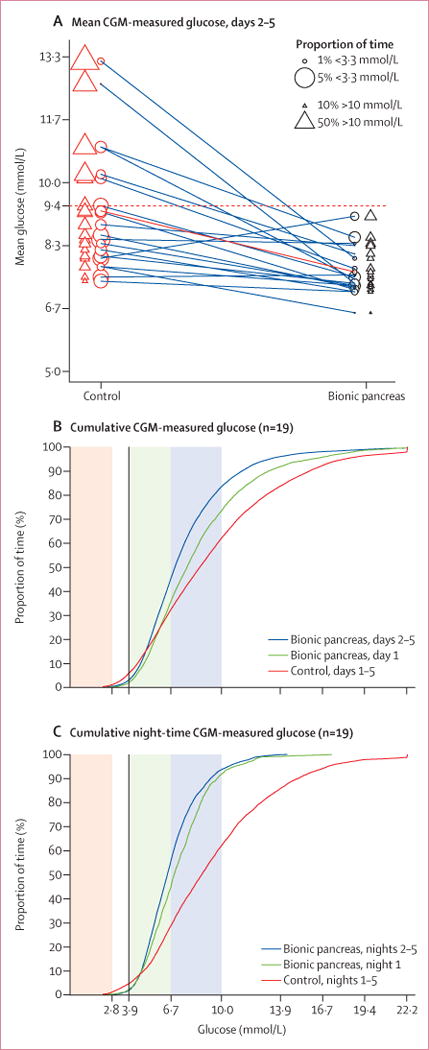
(A) Mean glucose concentration in each participant on days 2–5 of the control period (red circles and triangles), connected by a line to the corresponding mean glucose concentration during the bionic pancreas period (black circles and triangles); the area of each circle and triangle is proportional to the proportion of time that the participant spent with a low glucose concentration (<3·3 mmol/L; circle) and a high glucose concentration (>10 mmol/L; triangle), respectively, on days 2–5. The dashed red line is the mean glucose threshold of 9·4 mmol/L, which corresponds to a predicted HbA1c of 7·5% (the upper limit of the therapeutic goal for children as outlined by the American Diabetes Association); the solid red line is the mean for all patients in that study group and connects red (control) and black (bionic pancreas) circles and triangles that correspond to the mean proportion of time the participants spent with a glucose concentration of less than 3·3 mmol/L and greater than 10 mmol/L, respectively. (B) Cumulative glucose concentrations during the bionic pancreas period (day 1 and days 2–5) and during the 5-day control period. (C) Cumulative night-time glucose concentrations. In (B) and (C), the region shaded red corresponds to glucose concentrations of less than 2·8 mmol/L, green to 3·9–6·7 mmol/L, and blue to 6·7–10 mmol/L. The vertical black line at 3·9 mmol/L is the bottom of the normal glucose range, by convention. To convert the values for glucose to mg/dL, multiply by 18. CGM=continuous glucose monitoring.
During the bionic pancreas period, participants spent more time within the 3·9–10 mmol/L glucose range on days 2–5 than during the control period, and less time with a glucose concentration of greater than 10 mmol/L or less than 3·3 mmol/L (table 2, figure 2B). During the night, the differences between the bionic pancreas and control periods were nominally larger than during the 24 h period for CGM-measured glucose concentrations, and proportions of time spent with a glucose concentration of less than 3·3 mmol/L or within the 3·9–10 mmol/L glucose range (table 2; figure 2C). The aggregate mean and SD of CGM-measured glucose concentrations had nominally lower variability during the bionic pancreas period than during the control period for both the full day and at night (table 2; figure 3).
Figure 3. Variation in the CGM-measured mean glucose concentration during the bionic pancreas and control periods over the course of the study.
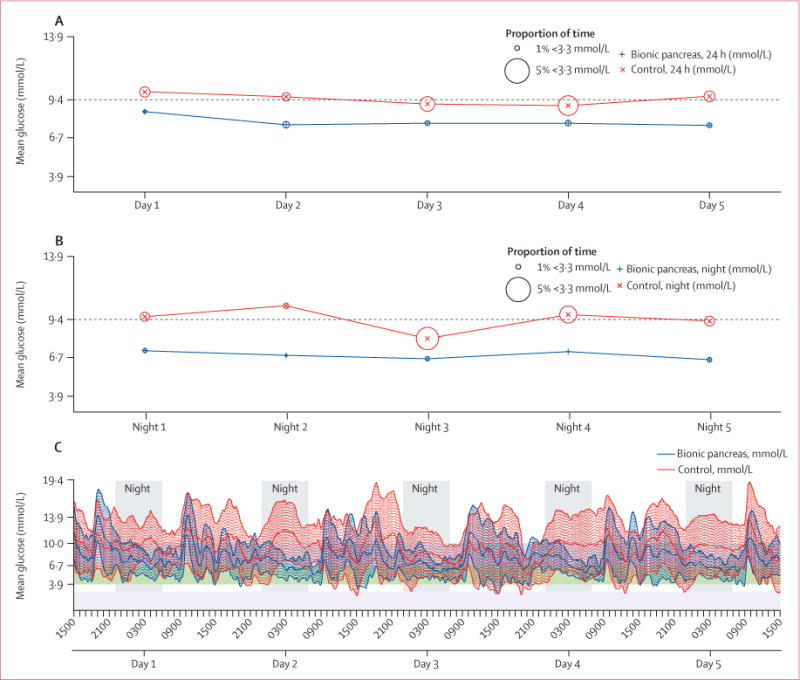
Mean daily (A) and night-time (B) CGM-measured glucose concentrations and proportion of time spent with a glucose concentration lower than 3·3 mmol/L on days (or nights) 1–5 during the bionic pancreas period (blue) and the control period (red). (C) Superposition of tracings of mean glucose concentrations at all 5 min intervals during the bionic pancreas (blue) and control (red) periods. Each tracing is surrounded by an area of shading of the same colour that spans 1 SD in both directions from the mean. The horizontal region shaded in purple corresponds to glucose concentrations of less than 2·8 mmol/L, green to 3·9–6·7 mmol/L, and blue to 6·7–10 mmol/L. To convert the values for glucose to mg/dL, multiply by 18. CGM=continuous glucose monitoring.
The bionic pancreas period was associated with a mean CGM-measured glucose concentration on days 2–5 below the American Diabetes Association’s threshold for glycaemic control in children (HbA1c ≤7·5%,20 corresponding to a mean glucose concentration of ≤9·4 mmol/L21,22) in all 19 participants, compared with 12 of 19 participants during the control period (figures 2A, 4A). Although the lower HbA1c target of 7·0% or lower (corresponding to a mean glucose concentration of ≤8·6 mmol/L21,22) is only recommended for adults,20 the bionic pancreas was associated with a mean CGM-measured glucose concentration below this threshold on days 2–5 in 18 of 19 participants, compared with eight of 19 during the control period. A higher target of HbA1c of 8·0% or lower (corresponding to a mean glucose concentration of ≤10·2 mmol/L) is sometimes used when hypoglycaemia is of particular concern. The bionic pancreas was associated with a mean CGM-measured glucose concentration below this threshold during days 2–5 in 19 of 19 participants, compared with 14 of 19 participants during the control period.
Figure 4. Distributions of mean glucose concentrations and insulin doses.
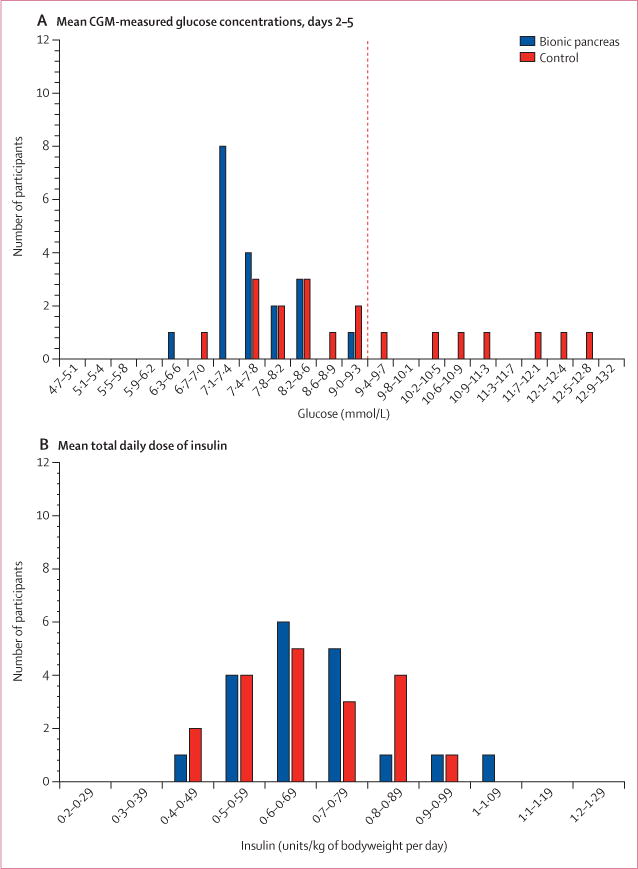
(A) Histogram distribution of mean CGM-measured glucose concentrations per participant on days 2–5 during the bionic pancreas and control periods, with mean glucose concentrations divided into intervals of 0·39 mmol/L. The dashed red line shows the mean glucose concentration of 9·4 mmol/L, which corresponds to a predicted HbA1c of 7·5%. (B) Histogram distribution of mean total daily doses of insulin on days 2–5, divided into intervals of 0·1 units/kg of bodyweight per day. To convert the values for glucose to mg/dL, multiply by 18. CGM=continuous glucose monitoring.
During the bionic pancreas period, mean CGM-measured glucose concentrations were lower on days 2–5 (7·6 mmol/L [SD 0·6]) than on day 1 (8·5 mmol/L [1·1]; p=0·00012); no such difference in mean CGM-measured glucose concentrations was noted during the control period (9·3 mmol/L [SD 1·7] on days 2–5 vs 10·0 mmol/L [2·1] on day 1; p=0·20).
Outcomes based on scheduled plasma glucose measurements were similar to those based on CGM-measured glucose concentrations. The mean of all scheduled plasma glucose measurements on days 1–5 (we used data from all days because plasma glucose sampling was less frequent than CGM) was lower during the bionic pancreas period than during the control period (table 2). The median proportion of scheduled plasma glucose concentrations below 3·3 mmol/L on days 2–5 did not differ significantly between the bionic pancreas and control periods (table 2).
During 95 participant-days (days 1–5 of each intervention), 54 carbohydrate interventions were given for hypoglycaemia to participants during the bionic pancreas period compared with 92 during the control period (table 2; appendix). At night, fewer median carbohydrate interventions occurred during the bionic pancreas period than during the control period (table 2). Fewer median grams of carbohydrate were given per day per participant to treat hypoglycaemia during the bionic pancreas period (7·3 g [range 0–19·2]) than during the control period (12·7 g [0–40]; p=0·026).
The mean number of scheduled plasma glucose checks per participant (out of 20 possible checks over 5 days) was 19·9 (SD 0·3) with the bionic pancreas and 19·9 (0·3) during the control period. The mean total number of plasma glucose checks (scheduled and unscheduled) per participant was 50·7 (SD 12·3) with the bionic pancreas and 52·5 (8·7) during the control period.
The mean total daily dose of insulin delivered by the bionic pancreas varied widely between participants (range 0·43–1·08 units/kg of bodyweight per day), but the mean total daily dose did not differ during the bionic pancreas and control periods (0·68 units/kg of bodyweight per day [SD 0·15] vs 0·68 units/kg of bodyweight per day [0·13], respectively; p=0·90; figure 4B). The mean proportion of insulin given on days 2–5 as adaptive meal-priming boluses by the bionic pancreas in response to meal information being inputted before eating was 26% [SD 7·9] of the total dose and 43% [12·4] of non-basal insulin (separate subalgorithms automatically determined basal delivery and boluses that were delivered in response to glucose excursions). The total daily dose of insulin during the bionic pancreas period did not significantly differ between day 1 and days 2–5 (0·66 units/kg of bodyweight per day [SD 0·15] vs 0·68 units/kg of bodyweight per day [0·15], respectively; p=0·42). The mean total daily dose of glucagon on days 2–5 during the bionic pancreas period was 0·36 mg/day (SD 0·12; range 0·16–0·58), or 10·9 μg/kg of bodyweight per day (SD 4·0). The total daily dose of glucagon during the bionic pancreas period did not significantly differ between day 1 and days 2–5 (6·8 μg/kg of bodyweight per day [SD 2·4] vs 7·8 μg/kg of bodyweight per day [3·8], respectively; p=0·096).
Participants chose their own meals without influence by study staff. The mean daily meal and snack carbohydrate consumption, not including rescue carbohydrates for hypoglycaemia, was higher during the control period than with the bionic pancreas (6·7 g/kg of bodyweight per day during control period [SD 1·7] vs 6·1 g/kg of bodyweight per day [1·5] with the bionic pancreas; p=0·016). When analysed by meal, the difference between the control and bionic pancreas periods was statistically significant only for breakfast (1·8 g/kg of bodyweight per day [SD 0·7] vs 1·5 g/kg of bodyweight per day [0·6], respectively; p=0·0049; appendix). Breakfast follows the night-time, which is when the largest difference was noted between the control and the bionic pancreas periods in terms of the proportions of time that the CGM-measured glucose concentration was above 10 mmol/L (table 2) and above 13·9 mmol/L (median 9·1% [range 0–56] vs 0% [0−1·3], respectively; p<0·0001). The median body mass change from day 1 to day 5 did not differ significantly between the control and bionic pancreas periods (0 kg [range −1·9 to 1·1] vs 0·2 kg [−1·3 to 2·7], respectively; p=0·12; appendix).
No episodes of severe hypoglycaemia were recorded during the study. Medium-to-large concentrations of ketones (range 0·6–3·6 mmol/dL) were reported on seven occasions in five participants during the control period, and on no occasion during the bionic pancreas period (p=0·063). The ketone concentrations returned to normal ranges after the infusion set was changed or insulin was given, in accordance with camp policy (appendix). We noted no difference in self-reported nausea between the bionic pancreas and the control periods. Participants reported some nausea a mean of 22·8% (SD 24·9) of the days during the bionic pancreas period versus 24·6% (26·8) of the days during the control period (p=0·77; appendix), and the mean daily visual analogue score for nausea (scale of 0–10) was 1·3 points (SD 2·0) with the bionic pancreas versus 1·4 points (1·8) during the control period (p=0·81). Two episodes of vomiting occurred, one with the bionic pancreas and one with control. Headache and stomach discomfort without nausea were each reported once during the bionic pancreas period and were not reported during the control period. Eight unscheduled insulin infusion site changes occurred during the bionic pancreas period (two for suspected failure, two for pain, and four because they fell out) and six unscheduled changes occurred during the control period (five for suspected failure, none for pain, and one because it fell out). There were four unscheduled glucagon infusion site changes during the bionic pancreas period (none for suspected failure, one for pain, and three because they fell out; appendix).
The overall mean absolute relative difference, expressed as a percentage, between plasma glucose concentrations and the closest CGM-measured glucose concentration within 2·5 min of each plasma glucose concentration (n=1479) was 19·2% (SD 16·5), with a mean negative bias (ie, proportion of CGM-measured glucose concentrations lower than plasma glucose concentrations) of 5·3% (ie, CGM underestimated plasma glucose by a mean of 5·3%). The mean absolute relative differences between plasma glucose concentrations and the closest CGM-measured glucose concentration within 2·5 min of each plasma glucose concentration during the bionic pancreas period was 19·4% (SD 4·1), compared with 19·6% (3·2) during the control period (p=0·85). During the control period, two participants used their own CGM devices (appendix). Although we did not exclude participants who used non-insulin injectable diabetes drugs, no participant used any drug other than insulin for diabetes management.
The insulin and glucagon pumps lost wireless connectivity to the bionic pancreas 4·9% (SD 2·5) and 6·1% (3·1) of the time on days 1–5, respectively. Reconnection was usually spontaneous. No CGM signal could be detected a mean of 4·2% (SD 1·9) of the time on days 1–5 with the bionic pancreas and 5·1% (1·9) of the time during the control period. Much of the CGM downtime was due to the need to replace CGM sensors. After replacement, a 2 h warm-up period was needed before the CGM system came back online. The bionic pancreas administered a dose of basal insulin during these times that was based on the mean of previous insulin doses at that time of the day, the CGM-measured glucose concentration, and the trend in glucose concentrations before the offline period, and any entered plasma glucose concentrations. The bionic pancreas responded with bolus insulin on three occasions and bolus glucagon on no occasions in response to plasma glucose values that were entered on 14 occasions when the CGM signal was unavailable (mean of 0·7 [SD 1·4] occasions per participant). No malfunction of iPhones, algorithms, or pumps occurred, other than the losses of wireless connectivity. Results for additional prespecified secondary outcomes are reported in the appendix
Discussion
We tested the bihormonal bionic pancreas in preadolescents (6–11 years old) with type 1 diabetes in the same diabetes camps as our previous study in adolescents (12–20 years old) were based.13 As in our previous outpatient studies in adults and adolescents,13 and one camp study in older children,17 no restrictions were placed on diet or physical activity, by contrast with studies done by other investigators.14–16 The bionic pancreas was associated with reduced mean CGM-measured and plasma glucose concentrations, reduced hypoglycaemia, and a reduced frequency of carbohydrates given to treat hypoglycaemia relative to the control period, despite extremely close monitoring in the control period and rapid intervention for hypoglycaemia in the camp setting. Inputting of meal data into the bionic pancreas user interface before eating required only a rough estimate of meal carbohydrate content, a design feature of the bionic pancreas that eliminates carbohydrate counting and reduces patient burden.
The study had some limitations. We did not meet our enrolment target of 24 participants, although all 19 participants that were screened were eligible and were enrolled. However, robust differences in the primary outcomes between the bionic pancreas and control periods were nevertheless shown by both the prespecified univariate analysis and by multivariable analysis done to assess the effect of baseline HbA1c, and possible period and carryover effects. Multivariable analysis detected a period effect for the difference in the mean CGM-measured glucose concentration, with the average concentration in the second period higher than the first, mainly driven by a higher mean glucose concentration in the control group in the second period. A possible explanation is that the aggressiveness of glycaemic regulation by the camp physicians and staff was reduced in the second week of the 2 week camp session. Multivariable analysis of the proportion of time spent with a glucose concentration below 3·3 mmol/L showed a carryover effect, suggesting that the lower proportion of time spent with hypoglycaemia during the bionic pancreas period reduced the amount of hypoglycaemia during the subsequent control period, and likewise that the larger amount of hypoglycaemia during the control period increased the amount of hypoglycaemia in the subsequent bionic pancreas period, leading to a smaller difference between the two types of treatment in the second period despite the 3 day washout stage.25,26 Baseline glycaemic regulation, as represented by baseline HbA1c, had no significant effect on either of the coprimary outcomes.
Carbohydrate interventions for hypoglycaemia may have been given more frequently or earlier in both the bionic pancreas and control periods than they would have been without telemetric monitoring, but the monitoring was identical between the two groups (ie, similar CGM devices were used in both intervention periods, data was transmitted in an identical way to the remote monitoring station, and study staff were informed in the same way if glucose concentrations fell below a specified threshold). Participants ate fewer carbohydrates during the bionic pancreas period than during the control period, mainly because participants had a lower carbohydrate intake at breakfast during the bionic pancreas period. This lower consumption of carbohydrates at breakfast during the bionic pancreas period might have been related to spending less time above the glycosuric threshold during the night-time hours than during the control period. Another possibility is that glucagon reduced the appetite of the children, even though no difference in self-reported nausea was noted between the study periods. In our previous inpatient studies,19,27,28 frequent measurements showed that mean plasma glucagon concentrations remained in the normal fasted range most of the time. Frequent measurement of glucagon concentrations was not possible in the current study, but glucagon dosing was higher than dosing in our previous inpatient studies.19,27,28 On the basis of the relation between dosing and mean plasma glucagon concentrations in our previous inpatient studies,19,27,28 we estimate that mean plasma glucagon concentrations in this study would have been about 73 pmol/L (256 pg/mL), which is above the normal range of 14–43 pmol/L (50–150 pg/mL) in the fasted state for healthy individuals without diabetes. What plasma glucagon concentrations would be if glucagon were secreted normally in the setting of exercise and threatened and actual hypoglycaemia in patients with diabetes is unknown. Future studies will be done to investigate the long-term safety of chronic, intermittent, microdose administration of glucagon.
The current version of the bionic pancreas device has several limitations. Paracetamol has to be avoided because it can lead to an overestimation of blood glucose concentrations by the Dexcom G4 sensor.18 Future generations of the sensor will be resistant to interfering substances. Because the device requires wireless communication between the iPhone and the pumps, transient losses of communication with the pumps caused doses of insulin and glucagon to be delayed. Losses of pump communication and periods without a CGM signal might have negatively affected glycaemic regulation. The next version of the bionic pancreas will integrate both pumps with the control unit, eliminating the need for wireless communication for dosing. The limited stability of currently available glucagon formulations necessitated daily glucagon reservoir changes; a stable glucagon formation, which would not require daily reservoir changes has been developed29 and is in clinical testing.
The results of the present study, taken together with the results of our previous outpatient studies in adults and adolescents,13 collectively show that, with no information about the participant other than body mass and only qualitative estimates of meal carbohydrate content, the bionic pancreas has consistently been associated with better glycaemic regulation than conventional insulin pump therapy in volunteers with type 1 diabetes aged between 6 and 76 years, diagnosed with diabetes for 1–45 years, with a body mass of 21–128 kg, and an average total daily dose of insulin between 15 and 145 units per day. In the diabetes camp setting, children are supervised by counsellors with type 1 diabetes, are monitored by a nurse assigned to each cabin, have their insulin regimens adjusted daily by a health-care provider, are provided with carbohydrate counts for all food items, and are supported by the staff so that they never miss a meal bolus. In this trial, additional telemetric monitoring for hypoglycaemia was also done, which supplemented the usual camp safety monitoring regimen. Despite all this support for the participants during the control period, the bihormonal bionic pancreas still was associated with better glycaemic regulation without the need for precise carbohydrate counting or input from health-care providers or other adults. The bionic pancreas thus provided better glycaemic regulation with less effort devoted to diabetes decision making and management than is possible with the current standard of care in diabetes management. Such technology might be particularly useful in children who are not able to manage their own diabetes treatment.
Supplementary Material
Research in context.
Evidence before this study
We searched Ovid Medline for articles published in English up to July 10, 2015, using the search terms [“artificial pancreas” OR “bionic pancreas” OR “closed-loop”] AND [“diabetes mellitus” OR “diabetes”] AND “children” OR “pediatric/s” OR “pre-adolescent”] AND [“randomized” OR “randomized controlled trial”], and identified two randomised trials in which automated glucose control was tested in outpatient settings during the day and night. One of these was our crossover study comparing the bihormonal bionic pancreas in 36 adolescent children (aged 12–20 years) at a diabetes camp for 5 days with camp-managed insulin pump therapy for 5 days, in random order. The other was a study by Ly and colleagues comparing an insulin-only artificial pancreas system in 21 adolescents and adults (aged 15–31 years) for 6 days with sensor-augmented pump therapy for 6 days. Our previous study showed a reduction in mean glucose concentration, increased time in target range (3·9–10 mmol/L [70–180 mg/dL]), and a reduced need for carbohydrate interventions for hypoglycaemia during the bionic pancreas period. Results of Ly and colleagues’ study showed no difference in time in target range (3·9–10 mmol/L [70–180 mg/dL]) between the two groups or any other improvement in glucose control with their insulin-only artificial pancreas.
Added value of this study
To our knowledge, this is the first outpatient study of automated glycaemic control in preadolescent children. We show that the bionic pancreas reduced mean glucose concentration, increased the time in the target glucose range (3·9–10 mmol/L [70–180 mg/dL]), reduced the time spent with hypoglycaemia, and reduced the need for carbohydrate interventions for hypoglycaemia versus insulin pump therapy managed by the camp medical staff. This is the first time, to our knowledge, that an automated glucose control system has been shown to be effective in young children, who are often unable to take care of themselves without the assistance of adult caregivers and are therefore likely to particularly benefit from automated glycaemic control.
Implications of all the available evidence
A bihormonal bionic pancreas can improve glycaemic regulation in children compared with standard insulin pump therapy in a highly supervised diabetes camp environment that is designed to provide optimum management of diabetes. Longer outpatient trials in the less supervised home and school environments of preadolescent children are warranted.
Acknowledgments
This study was supported by grants from the Leona M and Harry B Helmsley Charitable Trust (2014PG-T1D006, to ERD) and the National Institute of Diabetes and Digestive and Kidney Diseases (R01DK097657, to ERD and SJR). We thank the volunteers and their families for their participation and enthusiasm. We thank the Barton Center for Diabetes Education and the administration, medical staff, counsellors, and support staff of the Clara Barton and Elliot P Joslin Diabetes Camps for their assistance with the study. We thank Lilly, USA, for donating the glucagon used in this study. We thank Kari Galuski, Raquel Kochis, and Hannah Tupper for their dedicated effort and careful execution of the experimental protocol; John Jiang for technical assistance; Mary Lee and Mark Bissell for their input and contributions to the study design and assistance in the implementation and execution of the experimental protocol; Paige Coles, Mariah Chang, Angela Voss, Rebecca Emmetts, Mark O’Brien, and Alexander O’Donovan for their tireless dedication and careful attention to telemetric monitoring and equipment maintenance at camp; Mary Larkin, Nancy Kingori, Khadija Tlaiti, and Irene Orzechowski for organisational and logistical support; Adam Greene, George Zamanakos, Justin Schumacher, Tom Peyser, Liam Pender, Sean Saint, Vance Swanson, and James Sidwell for hardware and software support, technical advice, and support in kind; Niall Kavanagh, Hilary Orenberg, and Trevor Macdowell for user interface software support; Fyodor Wolf, Inderpreet Singh, and Murugesh Vyravanadan for remote monitoring software support; Sheila Ramerman for software and hardware documentation support; Nicole Sherry, Geoffrey Walford, and Nancy Wei for serving on the data safety and monitoring board; the members of the Partners Human Research Committee and the Boston University Charles River Campus Institutional Review Board for their oversight of the study; and Stayce Beck and Patricia Beaston for their assistance during the process of obtaining the investigational device exemption approval for these studies.
Footnotes
See Online for appendix
Contributors
FHE-K, ERD, and SJR designed the study, wrote the report, and decided to submit it for publication. FHE-K and ERD designed and built the closed-loop control algorithm and the bionic pancreas device. SJR supervised the clinical study. FHE-K, SJR, ERD, MAH, CB, KLM, RS, and MS collated, analysed, and interpreted the data. HZ did additional statistical analyses. All of the authors critically reviewed the draft report for content. FHE-K, ERD, and SJR had full access to the study data and vouch for the data and analysis.
Declaration of interests
FHE-K, ERD, and SJR have received loaned equipment, support in kind, and technical assistance from Dexcom and Tandem Diabetes Care. FHE-K and ERD hold a patent related to a fully automated control system for type 1 diabetes (US 7 806 854) and pending patent applications related to a blood glucose control system (PCT/US 11/058 688 and PCT/US 13/870 634), all assigned to Boston University. ERD has received lecture fees from Dexcom, Tandem Diabetes Care, and Eli Lilly. SJR has received lecture fees from Tandem Diabetes Care, Sanofi-Aventis, Eli Lilly, and Abbott Diabetes Care, serves on the scientific advisory boards for Tandem Diabetes Care and Companion Medical, and holds a pending patent application for a blood glucose control system (PCT/US 13/870 634), assigned to Partners HealthCare and Massachusetts General Hospital. All other authors declare no competing interests.
References
- 1.The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. doi: 10.1056/NEJM199309303291401. [DOI] [PubMed] [Google Scholar]
- 2.Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Effect of intensive therapy on the microvascular complications of type 1 diabetes mellitus. JAMA. 2002;287:2563–94. doi: 10.1001/jama.287.19.2563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353:2643–53. doi: 10.1056/NEJMoa052187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Petitti DB, Klingensmith J, Bell RA, et al. for the SEARCH for Diabetes in Youth Study Group Glycemic control in youth with diabetes: the SEARCH for Diabetes in Youth Study. J Pediatr. 2009;155:668–72. doi: 10.1016/j.jpeds.2009.05.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tamborlane RW, Bergenstal RM, Miller KM, DuBose SN, Hall CA, for the T1D Exchange Clinic Network The T1D Exchange clinic registry. J Clin Endocrinol Metab. 2012;97:4383–89. doi: 10.1210/jc.2012-1561. [DOI] [PubMed] [Google Scholar]
- 6.Wood JR, Miller KM, Maahs DM, et al. for the T1D Exchange Clinic Network Most youth with type 1 diabetes in the T1D Exchange clinic registry do not meet American Diabetes Association or International Society for Pediatric and Adolescent Diabetes clinical guidelines. Diabetes Care. 2013;36:2035–37. doi: 10.2337/dc12-1959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.The Diabetes Control and Complications Trial Research Group. Hypoglycemia in the diabetes control and complications trial. Diabetes. 1997;46:271–86. [PubMed] [Google Scholar]
- 8.Leese GP, Wang J, Broomhall J. Frequency of severe hypoglycemia requiring emergency treatment in type 1 and type 2 diabetes: a population-based study of health service resource use. Diabetes Care. 2003;26:1176–80. doi: 10.2337/diacare.26.4.1176. [DOI] [PubMed] [Google Scholar]
- 9.Cengiz E, Xing D, Wong JC, et al. for the T1D Exchange Clinic Network Severe hypoglycemia and diabetic ketoacidosis among youth with type 1 diabetes in the T1D Exchange clinic registry. Pediatr Diabetes. 2013;14:447–54. doi: 10.1111/pedi.12030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Weinstock RS, Xing D, Maahs DM, et al. for the T1D Exchange Clinic Network Severe hypoglycemia and diabetic ketoacidosis in adults with type 1 diabetes: results from the T1D Exchange clinic registry. J Clin Endocrinol Metab. 2013;98:3411–19. doi: 10.1210/jc.2013-1589. [DOI] [PubMed] [Google Scholar]
- 11.Cryer PE, Davis SN, Shamoon H. Hypoglycemia in diabetes. Diabetes Care. 2003;26:1902–12. doi: 10.2337/diacare.26.6.1902. [DOI] [PubMed] [Google Scholar]
- 12.Russell SJ. Progress of artificial pancreas devices towards clinical use: the first outpatient studies. Curr Opin Endocrinol Diabetes Obes. 2015;22:106–11. doi: 10.1097/MED.0000000000000142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Russell SJ, El-Khatib FH, Sinha M, et al. Outpatient glycemic control with a bionic pancreas in type 1 diabetes. N Engl J Med. 2014;371:313–25. doi: 10.1056/NEJMoa1314474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kovatchev BP, Renard E, Cobelli C, et al. Safety of outpatient closed-loop control: first randomized crossover trials of a wearable artificial pancreas. Diabetes Care. 2014;37:1789–96. doi: 10.2337/dc13-2076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Leelarathna L, Dellweg S, Mader JK, et al. Day and night home closed-loop insulin delivery in adults with type 1 diabetes: three-center randomized crossover study. Diabetes Care. 2014;37:1931–37. doi: 10.2337/dc13-2911. [DOI] [PubMed] [Google Scholar]
- 16.van Bon AC, Luijf YM, Koebrugge R, et al. Feasibility of a portable bihormonal closed-loop system to control glucose excursions at home under free-living conditions for 48 hours. Diabetes Technol Ther. 2014;16:131–36. doi: 10.1089/dia.2013.0166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ly TT, Roy A, Grosman B, et al. Day and night closed-loop control using the integrated Medtronic hybrid closed-loop system in type 1 diabetes at diabetes camp. Diabetes Care. 2015;38:1–8. doi: 10.2337/dc14-3073. [DOI] [PubMed] [Google Scholar]
- 18.Dexcom. Dexcom G4 Platinum user’s guide. http://www.dexcom.com/sites/dexcom.com/files/dexcom-g4-platinum/ifu/dexcom-g4-platinum-ifu.pdf (accessed April 1, 2014)
- 19.El-Khatib FH, Russell SJ, Magyar KL, et al. Autonomous and continuous adaptation of a bihormonal bionic pancreas in adults and adolescents with type 1 diabetes. J Clin Endocrinol Metab. 2014;99:1701–11. doi: 10.1210/jc.2013-4151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.American Diabetes Association. Standard of medical care in diabetes. Diabetes Care. 2013;36(suppl 1):S11–66. doi: 10.2337/dc13-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ, for the A1c-Derived Average Glucose Study Group Translating the A1C assay into estimated average glucose values. Diabetes Care. 2008;31:1473–78. doi: 10.2337/dc08-0545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.O’Riordan SM, Danne T, Hanas R, Peters CJ, Hindmarsh P. Paediatric estimated average glucose in children with type 1 diabetes. Diabet Med. 2014;31:36–39. doi: 10.1111/dme.12285. [DOI] [PubMed] [Google Scholar]
- 23.Molnar GD, Taylor WF, Ho MM. Day-to-day variation of continuously monitored glycaemia: a further measure of diabetic instability. Diabetologia. 1972;8:342–48. doi: 10.1007/BF01218495. [DOI] [PubMed] [Google Scholar]
- 24.Service FJ, Nelson RL. Characteristics of glycemic stability. Diabetes Care. 1980;3:58–62. doi: 10.2337/diacare.3.1.58. [DOI] [PubMed] [Google Scholar]
- 25.Cryer PE. Hypoglycemia begets hypoglycemia in IDDM. Diabetes. 1993;42:1691–93. doi: 10.2337/diab.42.12.1691. [DOI] [PubMed] [Google Scholar]
- 26.Garg SK, Brazg RL, Bailey TS, et al. Hypoglycemia begets hypoglycemia: the order effect in the ASPIRE in-clinic study. Diabetes Technol Ther. 2014;16:125–30. doi: 10.1089/dia.2013.0219. [DOI] [PubMed] [Google Scholar]
- 27.El-Khatib FH, Russell SJ, Nathan DM, Sutherlin RG, Damiano ER. A bihormonal closed-loop artificial pancreas for type 1 diabetes. Sci Transl Med. 2010;2:27ra27. doi: 10.1126/scitranslmed.3000619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Russell SJ, El-Khatib FH, Nathan DM, Magyar KL, Jiang J, Damiano ER. Blood glucose control in type 1 diabetes with a bihormonal bionic endocrine pancreas. Diabetes Care. 2012;11:2148–55. doi: 10.2337/dc12-0071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cersosima E, Cummins MJ, Kinzell JH, et al. A phase 2 comparative safety PK/PD study of stable non-aqueous glucagon (g-Pen) vs Lilly glucagon for treatment of severe hypoglycemia. Diabetes. 2014;63(suppl 1A):1–LB. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.