

Abstract
Context:
Since Demirjian system of estimating dental maturity was first described, many researchers from different countries have tested its accuracy among diverse populations. Some of these studies have pointed out a need to determine population-specific standards.
Aim:
The aim of this study is to evaluate the suitability of the Demirjian's method for dental age assessment in Tunisian children.
Materials and Methods:
This is a prospective study previously approved by the Research Ethics Local Committee of the University Hospital Fattouma Bourguiba of Monastir (Tunisia). Panoramic radiographs of 280 healthy Tunisian children of age 2.8–16.5 years were examined with Demirjian method and scored by three trained observers.
Statistical Analysis Used:
Dental age was compared to chronological age by using the analysis of variance (ANOVA) test. Cohen's Kappa test was performed to calculate the intra- and inter-examiner agreements.
Results:
Underestimation was seen in children aged between 9 and 16 years and the range of accuracy varied from −0.02 to 3 years. The advancement in dental age as determined by Demirjian system when compared to chronological age ranged from 0.3 to 1.32 year for young males and from 0.26 to 1.37 year for young females (age ranged from 3 to 8 years).
Conclusions:
The standards provided by Demirjian for French-Canadian children may not be suitable for Tunisian children. Each population of children may need their own specific standard for an accurate estimation of chronological age.
Keywords: Demirjian method, dental age, forensic odontology, panoramic radiographs
Introduction
The age of juveniles and adolescents is estimated using skeletal and dental anthropological methods.[1] Dental development is a useful indicator of maturation because of its high reliability, low coefficient of variation, and resistance to environmental effects.[1]
Children's dental age estimation can be based on dental emergence or on tooth formation stages observed in radiographs.[2] The second method is superior to the first as the tooth emergence is a short period determined by the time of the tooth appearance in the mouth, altered by local factors such as lack of space and systemic factors like the nutritional status.[2] Several methods for the determination of dental development from radiographs have been described.[3,4] Most of these are based on a comparison of the tooth radiographic development with the standard charts compiled from a large number of persons, usually in a well-defined geographic region.[1] One method which has been widely applied is the Demirjian system, first described in 1973 and based on a sample of French-Canadian children.[5] This method is based on eight classification stages spanning from crown and root formation to apex closure of the seven left permanent mandibular teeth.[5] The score of each stage is allocated and a sum of scores gives an evaluation of the subject's dental maturity. The dental maturity score (DMS) can be converted into dental age by means of available tables and percentile curves from the original study.[5] The difference between the dental and chronological age (CA) indicates advancement or delay in dental maturity. Numerous researchers have applied this method to groups of children in various parts of the world and the significant differences between most groups and the reference have been interpreted as either a true population difference or a secular trend.[1,2,6,7,8,9,10,11,12,13,14,15] Many authors have used this to justify the need for population-specific DMS.[7] The aim of this study is to evaluate the suitability of the Demirjian method for dental age assessment in Tunisian children.
Materials and Methods
Samples
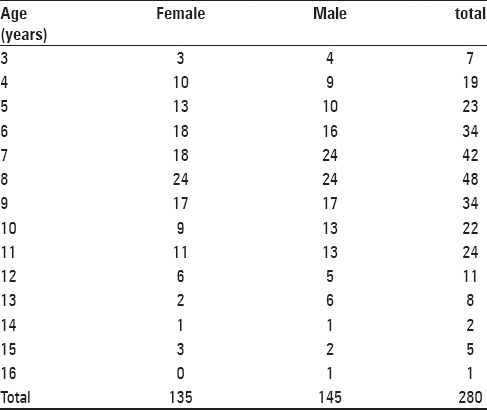
This is a prospective study previously approved by the Research Ethics Local Committee of the University Hospital Fattouma Bourguiba of Monastir (Tunisia). Orthopantomographs and clinical records of 280 Tunisian children of known CAs and gender were selected. In total, 145 boys and 135 girls aged between 2.8 and 16.5 years were included. The radiographs of healthy children were chosen from patients attending the dental clinic and nursery school. All the subjects were divided into 14 groups. Age group 4 involved patients aged 3.6–4.5 years and so on. The distribution by age and gender of digital panoramic radiographs is shown in Table 1.
Table 1.
Distribution of age and gender in the studied population
Exclusion criteria included image deformity affecting lower permanent tooth visualization, systemic diseases, congenital anomalies, dental agenesis and large caries, endodontic treatment of at least two bilaterally corresponding teeth in the mandible, and gross pathology in the mandible.
The CA of an individual was calculated by subtracting his or her birth date from the date on which the radiographs were obtained.
Dental age assessment method
The dental age was calculated using Demirjian method. All teeth of the lower left jaw (with the exception of the third molar) were assessed. Dental age was calculated according to the tables proposed by Demirjian et al.[5]
Assessment of the study sample
The measurements were carried out by three trained observers. To avoid the observers’ bias, each orthopantomograph was coded with a numerical ID. The subjects’ age and gender were thus unknown to the three observers.
For each gender and age group in the study, the mean differences between the dental ages and the CAs of the children as well as mean DMS were calculated. Analysis of variance (ANOVA) test was used to compare quantitative variables.
Reproducibility
Intra- and inter-observer reproducibility was calculated by re-examining 31 orthopantomographs 1 month after the initial assessment by the three observers. Cohen's Kappa test was performed to calculate the intra- and inter-examiner agreements.
Results
The percentage of the intra-observer agreement at the second reading of stage assessments in a total of 217 teeth was 81.56%, with 26 being one stage ahead and 14 being one stage behind. The Kappa coefficient varied from 0.944 to 0.985. The difference between both scores did not exceed one stage for any tooth [Table 1].
Inter-observer reproducibility is given in Table 2. Table 3 compares the estimated dental age (EDA) and the CA, using the Demirjian method in boys and girls. The mean age difference was 0.36 (SD = 1.23) in boys and 0.19 (SD = 1.20) in girls.
Table 2.
Inter-observer reproducibility

Table 3.
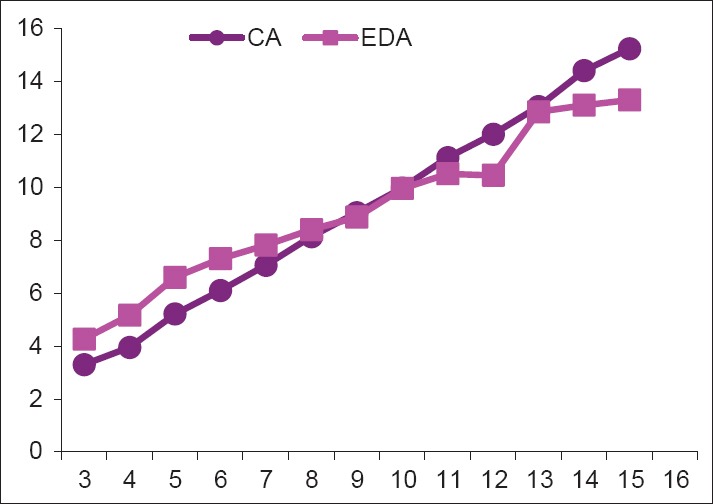
Comparison between the estimated dental age (EDA) using the Demirjian method and the chronological age (CA) (in years) among the studied children

The difference between EDA and CA (EDA – CA) is plotted against CA for boys [Figure 1] and girls [Figure 2]. Each dot represents a child. The smallest values (of around 0) represent children whose EDAs were close to their CAs. The values above 0 refer to children whose dental systems were advanced. The Demirjian method was found to overestimate the age, with a mean accuracy of 5 months for girls and 3 months for boys.
Figure 1.
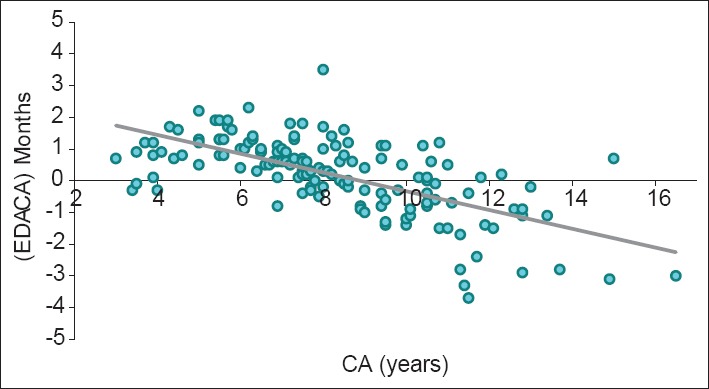
Scatterplot of the difference between estimated dental age and chronological age (EDA - CA) against the chronological (CA) with regression line for boys
Figure 2.
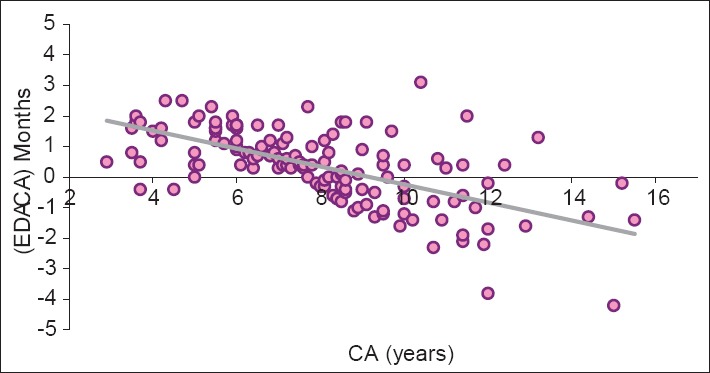
Scatterplot of the difference between estimated dental age and chronological age (EDA - CA) against the chronological (CA) with regression line for girls
Linear correlation between EDA and CA is represented in Figure 3 for boys and in Figure 4 for girls. Each dot represents a child. The line plotted joint points on which EDA corresponds to CA. R2 value is 0.807 for boys and 0.785 for girls.
Figure 3.
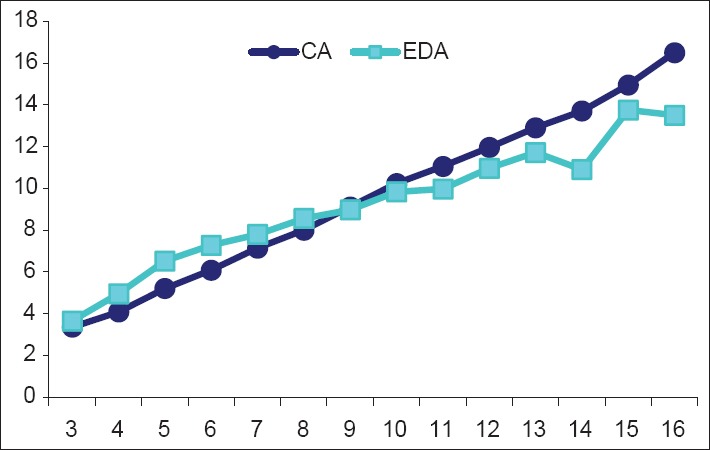
Linear correlation between EDA and CA for boys
Figure 4.
Linear correlation between EDA and CA for girls
Discussion
Age assessment is frequently required for medical and odontologic purposes.[12] Ideally, the estimated age should be as accurate as possible. Accuracy can be defined as how close to 0 is the difference between the estimated age and CA.[3] Dental estimation is widely accepted as it closely correlates with CA than other maturity indicators in children's development and it is the least variable method compared to other methods.[4,5] One of the most commonly used methods which has become the benchmark by which other methods are compared to for dental age assessment is the method reported by Demirjian et al., whereby they proposed a standard based on a large sample of 1446 males and 1482 females of French-Canadian origin.[5] The authors reported then that the possibility that the standards they obtained may not be valid in other population and that perhaps adaptations should be made for other samples.[16] In the present study, the age underestimation was seen in children aged between 9 and 16 years old and the range of accuracy varied from -0.02 to 3 years. The advancement in DA as determined by Demirjian system when compared to CA ranged from 0.3 to 1.32 year for young males and from 0.26 to 1.37 year for young females (age ranged from 3 to 8 years). The statistical analysis showed a significant difference between CA and EDA for age groups 5, 6, and 7, but not for age groups 3 and 4 in males. For females, it was a significant difference between CA and EDA for age groups 3, 4, 5, and 6, but not for age groups 7 and 8. Dental age advances in other populations were found by authors applying the Demirjian system: South Indians (3.04 years in males and 2.82 in females),[12] Somalis and White Caucasians (1.01 in Somali boys and 0.9 in Caucasian boys; 1.22 in Somali girls and 0.52 in Caucasian girls),[15] British (0.73 in boys and 0.51 in girls),[14] Dutch (0.4 in boys and 0.6 in girls),[17] and Turkish (0.36 to 1.43 in boys and 0.50 to 1.44 in girls).[2] Cultural and ethnic differences between populations may explain these increases in dental age.[12] Other probable causes include socioeconomic status, nutrition, and dietary habits, which vary among different population groups.[16] Ethnic differences between populations require new scoring and grading criteria for individual populations.[13] Liversidge[7] believed that the overestimation in dental age in recent findings using the Demirjian method in different populations may be partly explained by a positive secular trend in growth and development during the last 25 years. Compared to the previous French-Canadian sample, contemporary children generally have earlier sexual maturation, greater height and body weight due to the differences in the economical status and nutrition availability.[18] Demirjian method involved the cumbersome step of adding up a score for each stage of each tooth in order to obtain the maturity score, followed by a conversion of the maturity score to the EDA.[5] Due to this complicated method, the possibility of error could not be eliminated.[16]
The comparison of mean CA and EDA for the sample and different age groups in the present study showed a greater accuracy for females than males. Until the 11-year age group, almost all the observed developmental stages were earlier in females as compared to their male counterparts, thus indicating that females showed an earlier maturation in the dental development than males. This is in accordance with earlier maturation of other parameters of development in females such as height, sexual maturation, and skeletal development.[5,19,20] Hormonal factors may influence the sex differences in dental development.[21] However, the actual effect of hormones on tooth development is still largely unknown.[7]
One limitation of this study is that instead of the population being selected at random, it may not represent the general Tunisian population. Furthermore, the regression analysis itself may not be the ideal statistical approach for evaluating Demirjian method.[20] The Bayesian prediction has been advocated as a better alternative for assessing categorical data.[4] Logistic regression analysis may also be useful when the need is to allocate an individual as having reached a specific age.[14] We will consider these solutions in future studies in the application and adaptation of Demirjian method on Tunisian children. Multiethnic population data will be needed to assess the international applicability of the Demirjian method.[20]
Conclusion
The standards provided by Demirjian for French-Canadian children may be not suitable for Tunisian children. In order to calculate the dental age of this population, scoring can be carried out according to Demirjian system for the maturity score definition. Appropriate conversion Tables for transforming the maturity score into dental age for each gender must be carried out for Tunisian children. The same procedure should be encouraged for other populations.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Lee SS, Kim D, Lee S, Lee UY, Seo JS, Ahn YW, et al. Validity of Demirjian's and modified Demirjian's methods in age estimation for Korean juveniles and adolescents. Forensic Sci Int. 2011;211:41–6. doi: 10.1016/j.forsciint.2011.04.011. [DOI] [PubMed] [Google Scholar]
- 2.Tunc ES, Koyuturk AE. Dental age assessment using Demirjian's method on northern Turkish children. Forensic Sci Int. 2008;175:23–6. doi: 10.1016/j.forsciint.2007.04.228. [DOI] [PubMed] [Google Scholar]
- 3.Maber M, Liversidge HM, Hector MP. Accuracy of age estimation of radiographic methods using developing teeth. Forensic Sci Int. 2006;159:S68–73. doi: 10.1016/j.forsciint.2006.02.019. [DOI] [PubMed] [Google Scholar]
- 4.Lewis AB, Garn SM. The relationship between tooth formation and other maturational factors. Angle Orthod. 1960;30:70–7. [Google Scholar]
- 5.Demirjian A, Buschang PH, Tanguay R, Patterson DP. Interrelationships among measures of somatic, skeletal, dental and sexual maturity. Am J Orthod. 1985;88:433–8. doi: 10.1016/0002-9416(85)90070-3. [DOI] [PubMed] [Google Scholar]
- 6.Chen JW, Guo J, Zhou J, Liu RK, Chen TT, Zou SJ. Assessment of dental maturity of western Chinese children using Demirjian's method. Forensic Sci Int. 2010;197:1–4. doi: 10.1016/j.forsciint.2009.12.009. [DOI] [PubMed] [Google Scholar]
- 7.Liversidg HM. Interpreting group differences using Demirjian's dental maturity method. Forensic Sci Int. 2010;201:95–101. doi: 10.1016/j.forsciint.2010.02.032. [DOI] [PubMed] [Google Scholar]
- 8.Germano Maia MC, Almeida Martins MG, Germano FA, Branda Neto J, Bruno da Silva CA. Demirjian's system for estimating the dental age of northeastern Brazilian children. Forensic Sci Int. 2010;200:1–4. doi: 10.1016/j.forsciint.2010.03.030. [DOI] [PubMed] [Google Scholar]
- 9.Nik-Hussein N, Kee KM, Gan P. Validity of Demirjian and Willems methods for dental age estimation for Malaysian children aged 5–15 years old. Forensic Sci. Int. 2011;204:1–6. doi: 10.1016/j.forsciint.2010.08.020. [DOI] [PubMed] [Google Scholar]
- 10.Acharaya AB. Age estimation in Indian Using Demirjian's 8-teeth Method. J Forensic Sci. 2011;56:124–7. doi: 10.1111/j.1556-4029.2010.01566.x. [DOI] [PubMed] [Google Scholar]
- 11.Bagherpour A, Imanimoghaddam M, Bagherpour MR, Einolghozati M. Dental age assessment among Iranian children aged 6–13 years using the Demirjian method. Forensic Sci Int. 2010;197:121–4. doi: 10.1016/j.forsciint.2009.12.051. [DOI] [PubMed] [Google Scholar]
- 12.Koshy S, Tandon S. Dental age assessment: The applicability of Demirjian's method in South Indian children. Forensic Sci Int. 1998;94:73–85. doi: 10.1016/s0379-0738(98)00034-6. [DOI] [PubMed] [Google Scholar]
- 13.Bhat VJ, Kamath GP. Age estimation from root development of mandibular third molars in comparison with skeletal age of wrist joint. Am J Forensic Med Pathol. 2007;28:238–41. doi: 10.1097/PAF.0b013e31805f67c0. [DOI] [PubMed] [Google Scholar]
- 14.Liversidge HM, Speechly T, Hector MP. Dental maturation in British children: Are Demirjian's standards applicable? Int J Paediatric Dent. 1999;9:263–9. doi: 10.1111/j.1365-263x.1999.00144.x. [DOI] [PubMed] [Google Scholar]
- 15.Willems G, Van Olmen A, Spiessens B, Carels C. Dental age estimation in Belgian children: Demirjian's technique revisited. J Forensic Sci. 2001;46:893–5. [PubMed] [Google Scholar]
- 16.Chaillet N, Nystrom M, Demirjian A. Comparison of dental maturity in children of different ethnic origins: International maturity curves for clinicians. J. Forensic Sci. 2005;50:1164–74. [PubMed] [Google Scholar]
- 17.Leurs IH, Wattel E, Aartman IH, Etty E, Prahl-Andersen B. Dental age in Dutch children. Eur J Orthod. 2005;27:309–14. doi: 10.1093/ejo/cji010. [DOI] [PubMed] [Google Scholar]
- 18.Kalinowska IR, Raczkowska EK, Kalinowski P. Dental age in Central Poland. Forensic Sci Int. 2008;174:207–16. doi: 10.1016/j.forsciint.2007.04.219. [DOI] [PubMed] [Google Scholar]
- 19.Al-Emran S. Dental age assessment of 8.5 to 17 year-old Saudi children using Demirjian's method. J Contemp Dent Pract. 2008;9:64–71. [PubMed] [Google Scholar]
- 20.Hagg U, Matson L. Dental maturity as an indicator of chronological age: the accuracy and precision of three methods. Eur J Orthodont. 1985;7:25–34. doi: 10.1093/ejo/7.1.25. [DOI] [PubMed] [Google Scholar]
- 21.Hilgers KK, Akridge M, Scheetz JP, Kinane DE. Childhood obesity and dental development. Pediatr Dent. 2001;28:18–22. [PubMed] [Google Scholar]