

Abstract
Objective
Using a socio‐ecological model, this study examines the influence of facility characteristics on the transition of nursing home residents to the community after a short stay (within 90 days of admission) or long stay (365 days of admission) across states with different long‐term services and supports systems.
Data Source
Data were drawn from the Minimum Data Set, the federal Online Survey, Certification, and Reporting (OSCAR) database, the Area Health Resource File, and the LTCFocUs.org database for all free‐standing, certified nursing homes in California (n = 1,127) and Florida (n = 657) from July 2007 to June 2008.
Study Design
Hierarchical generalized linear models were used to examine the impact of facility characteristics on the probability of transitioning to the community.
Principal Findings
Facility characteristics, including size, occupancy, ownership, average length of stay, proportion of Medicare and Medicaid residents, and the proportion of residents admitted from acute care facilities are associated with discharge but differed by state and whether the discharge occurred after a short or long stay.
Conclusion
Short‐ and long‐stay nursing home discharge to the community is affected by resident, facility, and sometimes market characteristics, with Medicaid consistently influencing discharge in both states.
Keywords: Rebalancing, nursing home, long‐term services and supports, home‐ and community‐based care
Rebalancing the nation's long‐term services and supports (LTSS) from an institutional toward a home‐ and community‐based delivery system has been at the forefront of policy discussions for several decades. The success of these efforts depends largely on the ability of states to ensure that an initial nursing home rehabilitation admission remains short‐stay and to identify and support residents who can repatriate from nursing homes (NH) to the community. Although policy initiatives have been funded to develop and evaluate approaches that support NH residents who want to return to the community (e.g., Money Follows the Person, Real Choice System Grants) (Crisp et al. 2003; Reinhard 2010), many of these efforts have been only modestly successful. Further, although it is well documented that system factors such as state policies, payment incentives, market competition, and resource allocation affect the likelihood of hospitalizations among NH residents (Lewis et al. 1985; Weissert and Scanlon 1985; Intrator et al. 2007), little attention has been given to the effect that such factors have on the community discharge of NH residents.
Despite the emphasis on rebalancing, research on NH and market characteristics associated with community discharge has been sparse. A 2004 study examining system‐level and clinical predictors of discharge outcomes found that among Medicare beneficiaries, Medicare Prospective Payment policies reduced the relative risk for discharge to the community among stays up to 120 days (Wodchis, Hirth, and Fries 2004). Recently, a study by Arling et al. (2011) included facility characteristics in a comprehensive analysis of short‐stay discharges in Minnesota; they found that higher nurse staffing levels and higher occupancy were predictors of community discharge. Moreover, in their brief discussion on market‐level influences, they (Arling et al. 2011) noted that NHs with higher community discharge rates were located in areas with larger populations and had a greater ratio of home‐ and community‐based service (HCBS) recipients to NH residents (Arling et al. 2011).
As expected, most studies have focused on resident characteristics and have found that community discharge is influenced by demographics including gender, age, and marital status (Engle and Graney 1993; Murtaugh 1994; Mehr, Williams, and Fries 1997; Kasper 2005; Arling et al. 2010, 2011; Gassoumis et al. 2013), previous institutionalizations (Engle and Graney 1993; Mehr, Williams, and Fries 1997; Arling et al. 2010), preference or support for returning to the community (Nishita et al. 2008; Arling et al. 2010; Gassoumis et al. 2013), and the presence of physical, cognitive, or mental diseases or dependencies (Coughlin, McBride, and Liu 1990; Engle and Graney 1993; Murtaugh 1994; Mehr, Williams, and Fries 1997; Arling, Williams, and Kopp 2000; Arling et al. 2010, 2011; Gassoumis et al. 2013). These studies have focused primarily on short‐stay populations, with few examining discharge outcomes after 90 days (Wodchis, Hirth, and Fries 2004; Gassoumis et al. 2013). More recently, Gassoumis and colleagues (Gassoumis et al. 2013) compared predictors of transition among short‐stay and long‐stay residents and identified 17 admission characteristics that predicted short‐stay transitions to the community, but only two—severe cognitive impairment and cancer—were associated with a lower likelihood of community discharge after 90 days.
Conceptual Framework and Purpose
Using an ecological model of health behavior, this study investigates the facility and market characteristics that influence the transition of NH residents to the community. The ecological model posits that health behaviors are often influenced by factors at the personal, organizational, community, physical environment, and policy levels (Sallis, Owen, and Fisher 2008). As all levels of the ecological model are interdependent, the model argues that a combination of both personal and extrapersonal interventions (e.g., organizational, environment, or policy level) is needed to significantly change health behaviors (Sallis, Owen, and Fisher 2008). Because of this interdependency, variables at different levels work together to either facilitate or constrain health behavior (Sallis, Owen, and Fisher 2008).
Although research on the facility and market characteristics associated with the discharge of NH residents is limited, the ecological model posits that facility and market‐level factors influence discharge patterns. When considering the interdependency of various levels in the model, it follows that facility care planning decisions and resource availability as well as market‐level factors could influence the discharge status of NH residents. Acknowledging this interconnectedness, this study examines facility characteristics that influence the transition of NH residents to the community across two states with markedly different LTSS approaches: California and Florida. An examination of these two states allows for a discussion of how facility characteristics influence NH discharge among a sizeable proportion of the older adult population and serves as an initial investigation into whether community discharge is affected by interstate variations in facility characteristics.
This study also makes a more specific contribution because it is the first to investigate facility and market characteristics that influence the community discharge of short‐ and long‐stay NH residents in a multistate sample. To date, most studies examining NH transition have focused on resident characteristics within 90 days of admission. As a result, our understanding of the role that the broader environment plays in the community discharge of NH residents is limited. As characteristics of the residents immediate and community environments may differentially affect the short‐ and long‐stay NH population, this study serves as a preliminary investigation into the role that facility and market characteristics have on NH discharge.
Data and Methods
Sample
Together, California and Florida have over 8 million adults aged 65 and older accounting for nearly one‐fifth (19 percent) of the older adult population in the United States. In 2007, when data for this study were collected, California accounted for 11 percent of the U.S. older adult population and Florida had the highest proportion of older adults nationwide with 17.6 percent of its residents aged 65 and older. Both states have a highly competitive market for LTSS with the number of certified beds in California totaling 113,527 across 1,189 NHs and Florida having 80,503 certified beds in 671 NHs (Harrington et al. 2011). Occupancy rates in both states were at or above the 2007 U.S. average of 85.2 percent, with 85.6 percent NH occupancy in California and 88.7 percent NH occupancy in Florida (Harrington et al. 2011). In addition, California and Florida differ significantly in the balance of their LTSS systems. As the fifth most balanced state in the United States, more than half (52 percent) of California's LTSS expenditures were directed toward HCBS (Mollica and Hendrickson 2009). In contrast, only 17.5 percent of Florida's LTSS budget went toward HCBS. Much of California's spending on HCBS can be attributed to the In‐Home Supportive Services program, the largest personal assistance service in the United States (Mollica and Hendrickson 2009). Moreover, California has a relatively low rate of NH reimbursement at only $139.70 per day compared to Florida's rate of $178.75 per day in 2007 (AHCA Florida Agency for Health Care Administration 2007; Mollica and Hendrickson 2009).
Source of the Data
This study used secondary data for all certified NHs in California and Florida from 2007 to 2009. The study dataset was developed using the Minimum Data Set (MDS, version 2.0), the federal Online Survey, Certification, and Reporting (OSCAR) database, the Area Health Resource File (AHRF), and the Brown University database LTCFocUS.org website.
The MDS is a federally mandated clinical assessment instrument administered to all residents in Medicare‐ or Medicaid‐certified NHs. The MDS includes over 400 data elements related to the physical, mental, and psychosocial health of the residents and is administered to all NH residents within 14 days of admission and at prescribed intervals thereafter (Morris et al. 1997). Many of these items have been previously validated and impart details on the case mix and acuity level of the residents. Although the MDS 2.0 includes 5‐day assessments, these assessments are incorporated into the full assessment if the resident stays for a minimum of 14 days.
OSCAR is an administrative database maintained by CMS that provides facility‐level information on the structure, patient census, staffing levels, and regulatory compliance of all Medicare‐ or Medicaid‐certified NHs. The data are derived from on‐site inspections conducted by state licensure agencies as part of the Medicare‐Medicaid certification process. Each inspection occurs within 15 months of the date of the facility's previous inspection.
The AHRF contains more than 6,000 county‐level variables on health care utilization, health professionals and facilities, resource scarcity, economic activity, and environmental and sociodemographic characteristics. In addition, the LTCFocUS.org website aggregates data from the MDS, OSCAR, AHRF, residential history files, and state policy data to characterize the policy environment and local forces affecting NH providers.
Study Design
This study was approved by the University of South Florida's Institutional Review Board. Data from the MDS 2.0 records were used to construct episodes of care for the cohort of residents aged 65 and older admitted between July 1, 2007, and July 30, 2008, to all free‐standing California (n = 1,127) and Florida (n = 657) NHs. The sample selection methodology followed that laid out by Thomas, Gassoumis, and Wilber (2010).
The unit of analysis was an episode of care, operationally defined as an aggregated NH stay without an intervening discharge period of more than 30 days (Thomas, Gassoumis, and Wilber 2009). An episode began when the resident was admitted to the NH as identified by an MDS full admission assessment and ended when the resident either died or was discharged from the NH and did not reenter the same NH within 30 days. Individual stays separated by less than 30 days were concatenated to create a single episode of care (Thomas, Gassoumis, and Wilber 2009). Thirty days of data prior to each baseline admission were checked to ensure that it represented a new stay; in addition, 395 days of data after the admission were examined to assess the resident's disposition for a full year while ensuring that reentry did not occur within 30 days.
Extremely short‐stay NH residents (defined as those without a full MDS admission assessment) were excluded from the study. Residents with an episode of care lasting for 90 days or less were considered short stay, whereas residents with an episode of care exceeding 90 days were considered long stay. Residents were then classified into mutually exclusive groups based on their discharge status (e.g., discharged to the community, transferred to another care facility, or died during the stay). The final study cohort was composed of 91,391 residents accounting for 93,308 episodes of care in California and 93,064 residents accounting for 98,046 episodes of care in Florida. Among short‐stay episodes: 77.7 percent were discharged to the community (e.g., home, assisted living, board‐and‐care), 14.9 percent were transferred to another care facility (e.g., NH, acute care hospital), and 7.4 percent died (Figure 1). In the long‐stay population, 23.2 percent were discharged to the community, 16.6 percent were transferred to another care setting, 41.5 percent remained in the facility for more than 365 days following admission, and 18.7 percent died (Figure 1). Discharge status was missing for less than 1 percent of the sample and those cases were excluded from the analysis.
Figure 1.
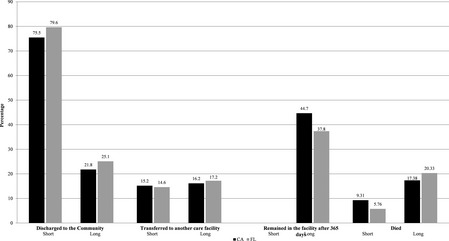
Discharge Disposition of Study Cohort
Measures
Dependent Variable
The primary outcome of interest was community discharge, defined as discharge to home, group home, board‐and‐care, or an assisted living facility (Arling et al. 2010, 2011; Gassoumis et al. 2013). Discharge was characterized by episode length and treated as a dichotomous variable (0 = remained in the facility; 1 = discharge to the community). Residents who were transferred to an acute care facility, another NH, or died were not examined in the multivariate analysis.
Independent Variables
Selection of the independent variables for this study was directed by the ecological model. Person‐level variables including demographics and measures of biological and psychological functioning were derived from the MDS admission assessment. Further, MDS data elements that have been associated with risk for placement or conversion into long‐stay were included in this analysis to account for resident‐level effects (Thomas, Gassoumis, and Wilber 2009; Arling et al. 2010; Gassoumis et al. 2013). These variables included age at admission, gender, race, marital status, living alone prior to admission, diagnoses or problem conditions (depression, mental health diagnosis, cognitive impairment, behavioral health problems, functional dependency, cancer, congestive heart failure, COPD, diabetes, Parkinson's disease, renal failure, stroke, and urinary or fecal incontinence), recent falls, and recent fractures. Dependency in eating, locomotion, hygiene, and toileting was measured with the Activities of Daily Living long‐form index (Morris, Fries, and Morris 1999), ranging from 0 (independent) to 28 (totally dependent). Cognitive impairment was measured based on the Cognitive Performance Scale (Morris et al. 1994), with scores of 0–1 representing intact cognitive function, scores of 2–4 representing mild/moderate cognitive impairments, and scores of 5–6 indicating severe cognitive impairment.
To account for the extrapersonal environment, facility‐ and market‐level variables were included in the analysis. One facility‐level variable was constructed by aggregating resident‐level variables from the MDS: the average episode length. Other facility‐level data elements derived from the OSCAR and LTCfocUS.org databases included occupancy; profit status; chain membership; number of licensed beds; total deficiency score; the proportion of residents funded by Medicare and by Medicaid; the proportion of residents admitted from acute care facilities; and the numbers of nursing and social work staff, including full‐time, part‐time, and contract employees.
Facilities were grouped into NH markets within their county. Market‐level covariates were obtained from the LTCfocUS.org and AHRF databases and included the proportion of residents aged 65 years or older, population density per square mile, and median household income. Two additional market‐level covariates assessed the NH climate: market occupancy and the Herfinadahl–Hirschman index, a measure of NH concentration within the market. Further details of all personal and extrapersonal level (facility and market) variables are provided in Table 1.
Table 1.
Definition of Resident‐, Facility‐, and Market‐Level Variables
| Variable | Variable Construction | Data Source |
|---|---|---|
| Market‐level variables | ||
| Herfinadahl–Hirschman Index | Measure of county's nursing home concentration; ranges from 0 to 1 with 1 representing a monopoly over a market's nursing home beds | LTCFocUs |
| Market occupancy | Number of occupied nursing home beds divided by the total number of beds in the county | LTCFocUS |
| Median household income | Median household income for the county | AHRF |
| Population density | Number of people per square mile for the county based on 2010 census | AHRF |
| Proportion of residents 65 years and older | County's population aged 65 years or older divided by the total population of the county | AHRF |
| Facility‐level variables | ||
| Total deficiency score | A summary score that captures the scope and severity of all violations and reported deficiencies based on the CMS Star rating | OSCAR |
| For‐profit ownership |
0 = Nonprofit 1 = For‐profit |
OSCAR |
| Chain membership |
0 = Independent 1 = Member of a chain |
OSCAR |
| Occupancy | Total number of residents divide by total number of residential care beds | OSCAR |
| Number of beds | Total number of beds in the facility | OSCAR |
| FTE RN HPRD | Continuous; number of full‐time equivalent registered nurses hours per resident per day (HPRD) | OSCAR |
| FTE LPN HPRD | Continuous; number of full‐time equivalent licensed nurses hours per resident per day (HPRD) | OSCAR |
| FTE CNA HPRD | Continuous; number of full‐time equivalent certified nursing assisted hours per resident per day (HPRD) | OSCAR |
| Social workers per 100 residents | Continuous; number of full‐time equivalent social workers per 100 residents | OSCAR |
| Proportion of Medicaid residents | Number of Medicaid residents divided by the total number of residents | OSCAR |
| Proportion of Medicare residents | Number of Medicare residents divided by the total number of residents | OSCAR |
| Proportion of residents admitted from acute care | Proportion of all admissions to the facility in the calendar year that were from an acute care hospital | LTCFocUS |
| Average episode length | Facility‐level aggregate based on study cohort; average number of days for an episode of care | MDS |
| Resident‐level variables | ||
| Age at admission | Continuous; calculated from birth date and date of admission | MDS |
| Marital status |
0 = Not married (includes never married, widowed, separated, and divorced) 1 = Married |
MDS |
| Race/ethnicity |
0 = Hispanic; black, non‐Hispanic; other 1 = White, non‐Hispanic (reference) |
MDS |
| Gender |
0 = Male 1 = Female |
MDS |
| Depression |
0 = No signs of depression 1 = Major/nonmajor depression |
MDS |
| Cognitive performance scale |
Three dummy variables Cognitively intact: scores 0–1 (reference) Mild/moderate impairment: scores 2–4 Severe impairment: scores 5–6 |
MDS |
| Lived alone before entry |
0 = Lived in another facility prior to admission 1 = Lived alone prior to admission |
MDS |
| Behavioral problem(s) |
0 = No behavioral problems 1 = Exhibited at least one of the following within the last 7 days: wandering, resisting care, verbally abusive, physically abusive, or socially inappropriate/disruptive behavioral symptoms |
MDS |
| ADL impairment | Continuous; activities of daily living (ADL) self‐performance scale, range: 0–28 | MDS |
| Urinary incontinence | Displayed urinary incontinence at least twice per week (scores 2 and greater) | MDS |
| Fecal incontinence | Displayed fecal incontinence at least once per week (scores 2 and greater) | MDS |
| Recent fall |
0 = No fall 1 = Experienced a fall in the past 180 days |
MDS |
| Recent fracture |
0 = No fracture 1 = Experienced a fracture (hip or otherwise) in the past 180 days |
MDS |
| Mental health diagnosis |
0 = No mental health diagnosis 1 = Diagnosis of schizophrenia or bipolar disorder |
MDS |
| Diseases |
Dummy variable defined separately for each disease (cancer, congestive heart failure [CHF], chronic obstructive pulmonary disease [COPD]/emphysema, diabetes, Parkinson's disease, renal failure, stroke/cerebrovascular accident) 0 = No disease 1 = Yes, disease present |
MDS |
Data sources were the Minimum Data Set (MDS), the federal Online Survey, Certification, and Reporting (OSCAR) databases, the LTCfocUS.org website, and the Area Health Resource File (AHRF).ADL, activities of daily living; CNA, certified nurse aid; FTE, full‐time equivalent; LPN, licensed practice nurse; NH, nursing home; RN, registered nurse.
Statistical Analysis
Descriptive statistics were examined at the facility and market levels for the California and Florida sample. Study outcomes were community discharge from a NH within 90 days (short stay) and between 91 and 365 days (long stay) following admission. In keeping with the ecological model, resident‐ and market‐level covariates were included in the model to provide a thorough context for the facility characteristics. Deviations from normality were examined for all predictor variables and appropriate transformations were applied. All predictor variables were grand mean centered. Given the hierarchical structure of the data with residents nested in facilities and facilities in markets, we estimated a three‐level hierarchical generalized linear model (HGLM) with facility characteristics treated as random effects and resident and market characteristics entered as covariates. As the dependent variable is binary, the HGLM used a logit link function and assumed a Bernoulli distribution. Separate models were constructed for community discharge for short‐ and long stays in both Florida and California. Several models were tested before arriving at a final set of variables that were theoretically relevant and not collinear. For each model, the area under the receiver operating characteristics (ROC) curve was calculated as an indicator of the predictive accuracy. All analyses were performed with StataIC Version 13 (StataCorp 2013).
Results
Baseline descriptive characteristics of the 1,127 California and 657 Florida NHs are reported in Table 2 (resident‐level characteristics are summarized in the Supplemental Digital Content 1). In 2007, California NHs had an average of 98 beds with an average occupancy rate of 86 percent, while Florida facilities averaged 121 beds with an occupancy rate of 88 percent. For‐profit NHs accounted for 86 percent of California facilities and 71 percent of Florida facilities. In both California (54 percent) and Florida (57 percent), more than half of the facilities were affiliated with a chain. On average, California NHs had 63 percent of residents funded by Medicaid, whereas an average of 56 percent of residents in Florida NHs were funded by Medicaid. The average episode of care during the study period was 184 days in California compared to 134 days in Florida.
Table 2.
Characteristics of the Nursing Homes and Markets
| M (SD) or % | χ2 or t | ||
|---|---|---|---|
| California | Florida | ||
| Facility characteristics | n = 1,127 | n = 657 | |
| Total deficiency score | 87.9 (96.0) | 62.7 (66.5) | 6.51*** |
| For‐profit ownership | 86.4 | 71.4 | 60.72*** |
| Chain membership | 53.7 | 57.1 | 1.93 |
| Occupancy | 86.4 | 87.7 | −2.34* |
| Number of beds (in 100s) | 98 (49) | 121 (45) | −10.09*** |
| Staffing measures | |||
| FTE RN HPRD | 0.36 (0.39) | 0.31 (0.20) | 3.63*** |
| FTE LPN HPRD | 0.90 (0.69) | 1.12 (0.37) | −8.69*** |
| FTE CNA HPRD | 2.78 (1.86) | 3.48 (1.36) | −9.03*** |
| Qualified social workers per 100 residents | 0.91 (1.47) | 1.31 (0.95) | −6.93*** |
| Proportion of Medicaid residents | 63.2 | 55.7 | 6.70*** |
| Proportion of Medicare residents | 13 | 19.8 | −10.74*** |
| Proportion of residents admitted from acute care | 0.802 (0.216) | 0.852 (0.145) | −5.55*** |
| Episode length (days) | 184.0 (101.4) | 133.8 (66.8) | 12.00*** |
| Market characteristics | n = 55 | n = 63 | |
| Herfinadahl index | 0.327 (0.350) | 0.379 (0.355) | −0.81 |
| Market occupancy | 84.6 | 88.4 | −3.09** |
| Median household income | $53,085 ($13,513) | $43,939 ($7,895) | 4.41*** |
| Population density | 699 (2,373) | 358 (534) | 1.04 |
| Proportion of residents 65 years and older | 0.109 (0.037) | 0.179 (0.077) | −4.66*** |
*p < .05; **p < .01; ***p < .001.
CNA, certified nurse aid; FTE, full‐time equivalent; HPRD, hours per resident day; LPN, licensed practice nurse; M, mean; SD, standard deviation; RN, registered nurse.
The 55 NH markets in California had an average market occupancy of approximately 85 percent and a Herfinadahl–Hirschman index of 0.33, while the 63 identified markets in Florida had an average NH occupancy of 88 percent and a Herfinadahl–Hirschman index of 0.38. In California, the markets had an average population density of 699 persons per square mile, while Florida had an average population density of 358 persons per square mile. The proportion of residents aged 65 and older in California was 11 and 18 percent in Florida.
Facility and Market Effects
Table 3 summarizes the results from the HGLM analyses for short‐ and long‐stay episodes in California and Florida. For the Florida models, the area under the ROC curve was 0.75 (95 percent CI: 0.69–0.81) for the short‐stay model and 0.63 (95 percent CI: 0.56–0.69) for the long‐stay model. Similarly, for the short‐ and long‐stay California models, the area under the ROC curve was 0.76 (95 percent CI: 0.71–0.83) and 0.61 (95 percent CI: 0.51–0.71), respectively.
Table 3.
Predictors of Community Discharge among Short‐ and Long‐Stay Episodes
| Short‐Stay Episodes | Long‐Stay Episodes | |||
|---|---|---|---|---|
| California (N = 93,308) | Florida (N = 98,046) | California (N = 42,605) | Florida (N = 36,571) | |
| Odds Ratio (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | |
| Market characteristics | ||||
| Herfinadahl index | 0.81 (0.60–1.08) | 0.97 (0.81–1.16) | 1.16 (0.70–1.92) | 1.88 (1.24–2.85) |
| Market occupancy | 1.00 (0.99–1.01) | 0.99 (0.98–1.00) | 1.00 (0.99–1.02) | 1.00 (0.99–1.01) |
| Median income | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) |
| Population density (log) | 0.99 (0.96–1.02) | 0.96 (0.89–1.04) | 1.04 (1.00–1.08) | 1.09 (1.02–1.16) |
| Proportion of residents 65+ | 1.24 (0.98–2.10) | 0.99 (0.99–1.00) | 1.15 (0.99–2.75) | 1.29 (0.64–2.61) |
| Facility characteristics | ||||
| Total deficiency score | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) |
| For‐profit ownership | 0.97 (0.90–1.05) | 0.96 (0.91–1.02) | 1.09 (1.05–1.26) | 1.17 (1.06–1.30) |
| Chain membership | 1.08 (0.96–1.12) | 0.98 (0.94–1.02) | 1.03 (0.95–1.12) | 1.06 (0.98–1.15) |
| Occupancy | 1.39 (1.10–1.74) | 1.61 (1.24–2.09) | 1.41 (0.92–2.17) | 1.25 (0.76–2.06) |
| Number of beds (in 100s) | 1.03 (1.05–1.12) | 1.04 (1.01–1.11) | 0.93 (0.85–1.01) | 1.05 (0.94–1.17) |
| Staffing | ||||
| FTE RN HPRD | 0.96 (0.89–1.05) | 1.04 (0.94–1.16) | 0.85 (0.73–1.00) | 0.98 (0.79–1.22) |
| FTE LPN HPRD | 0.99 (0.95–1.02) | 0.99 (0.91–1.07) | 0.94 (0.88–1.00) | 0.88 (0.76–1.03) |
| FTE CNA HPRD | 1.01 (0.99–1.02) | 1.00 (0.99–1.01) | 1.00 (0.98–1.03) | 1.01 (0.99–1.03) |
| SW per 100 residents | 1.02 (1.00–1.04) | 1.00 (0.99–1.02) | 1.01 (0.98–1.06) | 1.02 (0.98–1.06) |
| Proportion of Medicaid residents | 0.77 (0.67–0.89) | 0.68 (0.56–0.82) | 0.91 (0.87–0.94) | 0.79 (0.55–0.98) |
| Proportion of Medicare residents | 1.22 (0.98–1.52) | 1.27 (0.96–1.29) | 3.14 (2.11–4.68) | 2.30 (1.47–3.60) |
| Proportion of residents admitted from acute care | 1.58 (1.24–2.02) | 1.06 (0.69–1.63) | 1.10 (0.74–1.63) | 0.88 (0.50–1.55) |
| Average episode length | 0.98 (0.97–0.99) | 0.99 (0.98–0.99) | 0.99 (0.98–0.99) | 0.99 (0.97–0.99) |
| Resident characteristics | ||||
| Age at admission | 0.99 (0.99–0.99) | 0.98 (0.98–0.99) | 0.97 (0.96–0.97) | 0.97 (0.97–0.98) |
| Married | 1.29 (1.25–1.34) | 1.34 (1.29–1.39) | 1.06 (0.98–1.14) | 1.01 (0.93–1.09) |
| Caucasian | 1.05 (1.00–1.09) | 1.00 (0.96–1.05) | 0.91 (0.84–1.00) | 0.92 (0.84–1.01) |
| Female | 1.23 (1.19–1.27) | 1.12 (1.08–1.15) | 1.12 (1.05–1.20) | 1.08 (1.01–1.16) |
| Depression | 0.76 (0.70–0.82) | 0.78 (0.73–0.84) | 0.90 (0.76–1.04) | 0.89 (0.77–1.04) |
| CPS score | ||||
| Intact (0–1) | Reference | Reference | Reference | Reference |
| Mild (2–4) | 0.46 (0.45–0.48) | 0.49 (0.47–0.50) | 0.61 (0.57–0.65) | 0.59 (0.54–0.67) |
| Severe (5–6) | 0.20 (0.19–0.22) | 0.29 (0.27–0.31) | 0.27 (0.23–0.31) | 0.22 (0.19–0.39) |
| Lived alone | 1.08 (1.04–1.12) | 1.14 (1.10–1.18) | 1.20 (1.10–1.28) | 1.18 (1.10–1.27) |
| Behavioral problems | 0.70 (0.66–0.74) | 0.69 (0.65–0.73) | 0.70 (0.60–0.78) | 0.70 (0.62–0.80) |
| ADL impairment | 0.90 (0.90–0.91) | 0.93 (0.92–0.93) | 1.00 (0.99–1.02) | 1.02 (1.01–1.04) |
| Urinary incontinence | 0.75 (0.73–0.77) | 0.91 (0.88–0.95) | 0.88 (0.82–0.94) | 0.98 (0.91–1.04) |
| Fecal incontinence | 0.46 (0.43–0.49) | 0.50 (0.48–0.52) | 0.79 (0.73–0.92) | 0.83 (0.71–0.97) |
| Recent fall | 1.08 (1.04–1.11) | 0.98 (0.94–1.01) | 1.23 (1.15–1.32) | 1.06 (0.99–1.14) |
| Recent fracture | 1.47 (1.41–1.53) | 1.32 (1.27–1.38) | 1.49 (1.37–1.63) | 1.85 (1.70–2.01) |
| Mental health diagnosis | 0.79 (0.71–0.87) | 0.92 (0.82–1.03) | 1.42 (1.20–1.68) | 0.87 (0.69–1.11) |
| Diabetes | 0.89 (0.87–0.92) | 0.89 (0.86–0.92) | 1.03 (0.96–1.10) | 1.09 (1.02–1.17) |
| Stroke | 0.92 (0.89–0.96) | 0.90 (0.86–0.93) | 1.11 (1.03–1.21) | 1.24 (1.14–1.34) |
| CHF | 0.85 (0.82–0.88) | 0.82 (0.79–0.85) | 0.88 (0.81–0.95) | 0.86 (0.79–0.93) |
| Parkinson | 0.96 (0.89–1.03) | 0.93 (0.87–0.99) | 1.12 (0.98–1.28) | 1.05 (0.92–1.21) |
| Renal failure | 0.79 (0.75–0.83) | 0.79 (0.75–0.83) | 0.82 (0.74–0.91) | 0.92 (0.83–1.03) |
| Cancer | 0.68 (0.65–0.72) | 0.68 (0.65–0.71) | 0.60 (0.54–0.67) | 0.63 (0.57–0.70) |
| COPD | 0.84 (0.80–0.87) | 0.81 (0.78–0.84) | 0.80 (0.74–0.87) | 0.88 (0.81–0.94) |
Bold represents significant findings (p < .05). ADL, activities of daily living; CHF, congestive heart failure; CNA, certified nurse aid; COPD, chronic obstructive pulmonary disease; CPS, Cognitive Performance Scale; FTE, full‐time equivalent; HPRD, hours per resident day; LPN, licensed practice nurse; RN, registered nurse.
Short‐Stay Discharges (<90 days)
Facilities having greater odds of discharging residents to the community within 90 days of admission were large facilities with a greater total number of beds (CA: OR = 1.03; FL: OR = 1.04) and higher occupancy rates (CA: OR = 1.39; FL: OR = 1.61). Those facilities with a large proportion of Medicaid residents (CA: OR = 0.77; FL: OR = 0.68) were 23 and 32 percent, respectively, less likely to discharge residents and those with a longer length of stay (CA: OR = 0.98; FL: OR = 0.99) had lower odds of discharging residents to the community within 90 days of admission. Unique to California, facilities that admitted a higher proportion of residents directly from acute care facilities (OR = 1.58) were 58 percent more likely to discharge short‐stay residents to the community. In both California and Florida, market‐level characteristics were not associated with the discharge of short‐stay residents.
Long‐Stay Discharges (91–365 days)
As expected, several facility characteristics influenced the community discharge of long‐stay residents. Greater odds of community discharge were seen in for‐profit facilities (CA: OR = 1.09; FL: OR = 1.17) and those with a higher proportion of residents with Medicare funding (CA: OR = 3.14; FL: OR = 2.30), whereas facilities that predominately served Medicaid populations (CA: OR = 0.91; FL: OR = 0.79) had lower odds of discharging long‐stay residents to the community. In both California and Florida, facilities with a longer average length of stay had lower odds of discharging long‐stay residents (CA: OR = 0.99; FL: OR = 0.99).
In Florida, market‐level characteristics were also associated with the community discharge of long‐stay residents, with facilities located in more densely populated markets having a 9 percent likelihood of discharge (OR = 1.09) and markets with a greater NH concentration have an 88 percent greater likelihood (OR = 1.88) of discharging long‐stay residents.
Discussion
Although the community discharge of NH residents is important to policy makers, no research has addressed the effect that facility‐ and market‐level characteristics have on NH discharge in a large, multistate sample. As a result, the findings discussed here serve as a preliminary guide for examining the factors influencing NH discharge and should serve as a catalyst for further innovation and research into NH discharge.
In the study examples, community discharge of NH residents after both short and long stays was influenced by facility characteristics, including size, occupancy, for‐profit ownership, average length of stay, proportion of Medicare and Medicaid residents, and the proportion of residents admitted from acute care settings. Consistent with Arling et al. (2011), facility characteristics were more strongly related to community discharge than the characteristics of the markets in which they were located; market concentration and population density were associated with discharge, but only for long‐stay NH residents in Florida. Moreover, although facility characteristics served as important determinants of community discharge, resident characteristics were also strong drivers of community discharge and were largely consistent across the two states.
By comparing two states with different LTSS structures, we have gained insight into the role that facility characteristics have on the discharge disposition of residents in contrasting policy environments. Notably, among short‐stay episodes in both California and Florida, size and occupancy were associated with community discharge. Higher NH occupancy has consistently been linked to quality outcomes (Weech‐Maldonado, Neff, and Mor 2003). We speculate that the larger facilities with higher occupancy are likely to have more resources and better systems to develop care plans and more capacity to implement discharge planning. Conversely, facilities with a higher proportion of Medicaid residents and longer average lengths of stay are likely to have lower average reimbursement than facilities with higher Medicare reimbursement (Rahman et al. 2014), which decreases overall resources and, consequently, the odds of community discharge. Interestingly, in California, facilities that admitted a higher proportion of residents from an acute care facility as opposed to the community had much greater odds of discharging short‐stay residents to the community. As this finding was limited to the short‐stay population in California, it is possible that HCBS is more widely available in California compared to Florida. It is also possible that California facilities may have developed protocols for providing short, intensive rehabilitation services to residents from acute care facilities and expedited discharge back to the community to avoid long‐stay conversions.
In the long‐stay population, several facility characteristics were also associated with the community discharge of residents. The proportion of Medicaid residents and the facility's average length of stay were again inversely associated with the community discharge of residents, but unlike short‐stay episodes, both states were affected by facility ownership, with for‐profit facilities having greater odds of community discharge. Also unique to long‐stay episodes, in both California and Florida, facilities with a greater proportion of Medicare‐funded residents had two and three times greater odds of discharging long‐stay residents. Again, we speculate that facilities with a higher proportion of Medicare residents are both more likely to have more robust rehabilitation services and potentially more resources available to all residents (Rahman et al. 2014).
The proportion of Medicaid residents in a facility clearly affects the ability to discharge residents to the community, for both short‐stay and long‐stay episodes. Across both California and Florida, a higher proportion of Medicaid residents decreases the probability of community discharge. Consistent with earlier findings (Chapin et al. 1998), reliance on Medicaid to pay for LTSS greatly decreased the odds that the facility would transition its residents to the community, regardless of the state and length of stay. High‐Medicaid facilities have been shown to have fewer resources and create “tiers” of quality (Mor 2004), creating important concerns about the adequate level of reimbursement needed to restore function in long‐stay residents versus recognition that some admissions are likely to be appropriate placement (Mor 2011). As previous research has shown that Medicaid reimbursement policy has been associated with differing NH hospitalization rates (Intrator et al. 2007), NH hospice use (Miller et al. 2011), and resident outcomes (Mor et al. 2011), this finding has important implications, as it is possible that current rebalancing policies fail to adequately address the availability of and access to HCBS, thereby discouraging NHs from discharging their residents to the community with HCBS support.
Interestingly, market competition was only associated with community discharge in the long‐stay, Florida population. Often, market competition is viewed as a motivation for an individual nursing facility to innovate. From a facility's perspective, promoting community discharge could be an essential step toward innovation as it attempts to maximize efficiency by managing bed capacity.
Although a thorough examination of the resident‐level factors affecting community discharge falls outside the scope of the study, it is important to acknowledge the role that resident characteristics play in NH discharge. Consistent results from both states indicate that many resident characteristics are strong drivers of community discharge, even when accounting for facility and market characteristics. In addition, the findings from this study were strikingly consistent with prior studies (e.g., Engle and Graney 1993; Murtaugh 1994; Mehr, Williams, and Fries 1997; Arling, Williams, and Kopp 2000; Kasper 2005; Arling et al. 2010, 2011; Gassoumis et al. 2013) and suggest that community discharge is influence by demographics and the presence of physical, cognitive, or mental disease and dependencies. Given the current interests in LTSS rebalancing, transition programs should target those who have the potential for community discharge while recognizing the NH is the appropriate site of care for some long‐stay NH residents.
As suggested by the ecological model, facility and market characteristics influence the community discharge of NH residents. At the most macro‐level, differences between the two states are minimal. Although both states have markedly different approaches to LTSS and vary in their delivery of HCBS with California using a statewide in‐home supportive services program and Florida relying on county‐based HCBS waivers, the consistency across the extrapersonal levels suggests that resident characteristics play the largest role in determining community discharge.
It should be noted that this study only addresses community discharge from NHs and does not attempt to equate NH discharge with HCBS use. Second, we were unable to link our episodes to mortality data, at the time of the study, preventing us from assessing potential differences in mortality outcomes post community discharge. Third, the lack of statistical significance of market‐level variables may be due to the limitation of county‐level market definition. It is possible that states with more successful NH diversion after discharge from an acute care episode have different expectations for NH resident discharge outcomes, resulting in different dynamics between facility characteristics and discharge outcomes. Specifically, we speculate that states with higher rates of NH diversion would have residents with higher levels of acuity and less chance of eventual community discharge. With the introduction of the federal Community First Choices Option under the Affordable Care Act, it is possible that states will become more similar in NH diversion following acute care episodes, and that the impact of facility characteristics on discharge outcomes will become more consistent from state to state.
The current study design has several strengths, including its comparison across two varied LTSS landscapes, its inclusion of long‐stay NH residents, its inclusion of the population of residents and facilities in two states with the highest number of elders in the country, and its ability to longitudinally follow discharge dispositions for NH residents using episodes of care. However, limitations must be considered. First, this study only examined the discharge disposition of residents, not the success or duration of their discharge to the community; given the available data, we were unable to track hospitalizations following community entry. Second, although individual NH readmissions were followed using episodes of care, it was not possible to follow the trajectory of residents that were discharged from one NH but readmitted to a different NH; however, this limitation is mitigated by our focus on facility‐level variables. Finally, consistent with other studies (Arling et al. 2010, 2011), all resident‐level independent variables were based on the MDS admission assessments. Although, changes in a resident's status were not examined in this study, the use of the admission assessment is important because it allows researchers to make predictions regarding the long‐term prognosis for a resident based on admission characteristics. Despite these limitations, this study serves as an important step for understanding the role of facility characteristics in community discharge of NH residents.
As NH discharge is understudied, future studies should examine how changes in resident acuity and more detailed resident‐level payer information would differentially affect discharge outcomes and community transition by acquiring and linking more nuanced data. Additional studies should account for variations in length of stay and consider modeling days to discharge with respect to facility characteristics. Studies should also examine the effect of resident‐level data on the relationship between payer status and NH discharge as this represents an important area for future work. Finally, more research is needed to understand difference in NH utilization and HCBS expenditures among young disabled individual and the elderly and whether such differences affect community discharge rates.
Policy makers and advocates should be cognizant that the community discharge of NH residents is affected by resident, facility, and sometimes market characteristics. A facility's proportion of patients funded by Medicaid is a consistently important factor in community discharge across states and remains an important determinant in successful community transitions for short‐ and long‐stay NH residents. As long as Medicaid remains the primary funder for LTSS, Medicaid reimbursement schedules will continue to affect rebalancing efforts across the country. Ultimately, rebalancing initiatives should continue to work to develop approaches for delivering LTSS in the community, particularly for Medicaid‐eligible populations who might be able to transition home.
Supporting information
Appendix SA1: Author Matrix.
Appendix SA2: Characteristics of Nursing Home Resident Sample.
Acknowledgments
Joint Acknowledgment/Disclosure Statement: Funding for this project was made possible in part by contract MED103 with Florida's Agency for Health Care Administration.
Disclosures: None.
Disclaimers: None.
References
- AHCA Florida Agency for Health Care Administration . 2007. “Nursing Home Rates” [accessed on March 10, 2013]. Available at http://ahca.myflorida.com/medicaid/cost_reim/pdf/2007_07_initial_rates.pdf
- Arling, G. , Williams A. R., and Kopp D.. 2000. “Therapy Use and Discharge Outcomes for Elderly Nursing Home Residents.” The Gerontologist 40 (5): 587–95. [DOI] [PubMed] [Google Scholar]
- Arling, G. , Kane R. L., Cooke V., and Lewis T.. 2010. “Targeting Residents for Transitions from Nursing Home to Community.” Health Services Research 45 (3): 691–711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arling, G. , Abrahamson K. A., Cooke V., Kane R. L., and Lewis T.. 2011. “Facility and Market Factors Affecting Transitions from Nursing Home to Community.” Medical Care 49 (9): 790–6. [DOI] [PubMed] [Google Scholar]
- Chapin, R. , Wilkinson D. S., Rachlin R., Levy M., and Lindbloom R.. 1998. “Going Home: Community Reentry in Light Care Nursing Facility Residents Age 65 and Older.” Journal of Health Care Finance 25 (2): 35–48. [PubMed] [Google Scholar]
- Coughlin, T. A. , McBride T. D., and Liu K.. 1990. “Determinants of Transitory and Permanent Nursing Home Admission.” Medical Care 28 (7): 616–31. [DOI] [PubMed] [Google Scholar]
- Crisp, S. , Eiken S., Gerst K., and Justice D.. 2003. Money Follows Person and Balancing Long‐Term Care System: State Examples. Washington, DC: U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, and Disabled and Elderly Health Programs Division. [Google Scholar]
- Engle, V. F. , and Graney M. J.. 1993. “Predicting Outcomes of Nursing Home Residents: Death and Discharge Home.” Journal of Gerontology: Social Sciences 48 (5): S269–75. [DOI] [PubMed] [Google Scholar]
- Gassoumis, Z. D. , Fike K. T., Rahman A. N., Enguidanos S. M., and Wilber K. H.. 2013. “Who Transitions to the Community from Nursing Homes? Comparing Patterns and Predictors for Short‐Stay and Long‐Stay Residents.” Home Health Care Services Quarterly 32: 75–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrington, C. , Carrillo H., Dowdell M., Tang P. P., and Blank B. W.. 2011. Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2005 through 2010. San Francisco, CA: Department of Social and Behavioral Sciences, University of California San Francisco. [Google Scholar]
- Intrator, O. , Grabowski D., Zinn J., Schleintz Z., Feng Z., Miller S. C., and Mor V.. 2007. “Hospitalizations of Nursing Home Residents: The Effects of States’ Medicaid Payment and Bed‐Hold Policies.” Health Services Research 42: 1651–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasper, J. 2005. Who Stays and Who Goes Home: Using National Data on Nursing Home Discharges and Long Stay Residents to Draw Implications for Nursing Home Transition Programs. Washington, DC: Kaiser Family Foundation. [Google Scholar]
- Lewis, M. , Kane R. L., Cretin S., and Clark V.. 1985. “The Immediate and Subsequent Outcomes of Nursing Home Care.” American Journal of Public Health 75 (7): 758–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehr, D. R. , Williams B. C., and Fries B.. 1997. “Predicting Discharge Outcomes of VA Nursing Home Residents.” Journal of Aging and Health 9 (2): 244–65. [DOI] [PubMed] [Google Scholar]
- Miller, S. C. , Gozalo P., Lima J., and Mor V.. 2011. “The Effects of Medicaid Nursing Home Reimbursement Policy on Medicare Hospital Use in Nursing Homes.” Medical Care 49: 797–802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mollica, R. , and Hendrickson L.. 2009. Home and Community Based Long‐Term Care: Recommendations to Improve Access for Californians. Sacramento, CA: California Health and Human Services Agency. [Google Scholar]
- Mor, V. 2004. “A Comprehensive Clinical Assessment Tool to Inform Policy and Practice: Applications of the Minimum Data Set.” Medical Care 42 (4): 50–9. [DOI] [PubMed] [Google Scholar]
- Mor, V. 2011. “System Factors Affecting Long‐Term Care Outcomes.” Medical Care 49 (9): 787–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mor, V. , Gruneir A., Feng Z., Grabowski D., Intrator O., and Zinn J.. 2011. “The Effect of State Policies on Nursing Home Resident Outcomes.” Journal of the American Geriatrics Society 59: 3–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris, J. N. , Fries B., and Morris S. A.. 1999. “Scaling ADLs within the MDS.” Journals of Gerontology, Series A: Biological Sciences and Medical Sciences 54A (11): M546–53. [DOI] [PubMed] [Google Scholar]
- Morris, J. N. , Fries B., Mehr D. R., Hawes C., Philips C. D., Mor V., and Lipsitz L. A.. 1994. “MDS Cognitive Performance Scale.” Journal of Gerontology 49 (4): M174–82. [DOI] [PubMed] [Google Scholar]
- Morris, J. N. , Fries B., Steel K., Ikegami N., Bernabei R., Carpenter G. I., Gilgen R., Hirdes J. P., and Topinkova E.. 1997. “Comprehensive Clinical Assessment in Communtiy Setting: Applicability of the MDS‐HC.” Journal of the American Geriatrics Society 45 (8): 1017–24. [DOI] [PubMed] [Google Scholar]
- Murtaugh, C. M. 1994. “Discharge Planning in Nursing Homes.” Health Services Research 28 (6): 751–69. [PMC free article] [PubMed] [Google Scholar]
- Nishita, C. M. , Wilber K. H., Matsumoto S., and Schnelle J. F.. 2008. “Transitioning Residents from Nursing Facilities to Community Living: Who Wants to Leave?” Journal of the American Geriatrics Society 56 (1): 1–7. [DOI] [PubMed] [Google Scholar]
- Rahman, M. , Tyler D., Thomas K. S., Grabowski D., and Mor V.. 2014. “Higher Medicare SNF Care Utilization by Dual‐Eligible Beneficiaries: Can Medicaid Long‐Term Care Policies be the Answer?” Health Services Research 50 (1): 161–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinhard, S. C. 2010. “Diversion, Transition Programs Target Nursing Homes’ Status Quo.” Health Affairs 29 (1): 44–8. [DOI] [PubMed] [Google Scholar]
- Sallis, J. F. , Owen N., and Fisher E. B.. 2008. “Ecological Models of Health Behavior” In Health Behavior and Health Education, edited by Glanz Karen, Rimer Barbara K., Viswanath K., pp. 403–24. San Francisco, CA: John Wiley & Sons Inc. [Google Scholar]
- StataCorp . 2013. Stata Statistical Software: Release 13 (Release). College State, TX: StataCorp LP. [Google Scholar]
- Thomas, K. E. , Gassoumis Z. D., and Wilber K. H.. 2009. “Episodes of Care: An Important Framework for Investigating Nursing Home Outcomes.” The Gerontologist 29 (Suppl 2): 506–7. [Google Scholar]
- Thomas, K. E. , Gassoumis Z. D., and Wilber K. H.. 2010. “Conversion Diversion: Participation in a Social HMO Reduces the Likelihood of Converting from Short‐Stay to Long‐Stay Nursing Facility Placement.” Journal of American Medical Directors Association 11: 333–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weech‐Maldonado, R. , Neff G., and Mor V.. 2003. “Does Quality of Care Lead to Better Financial Performance?: The Case of the Nursing Home Industry.” Health Care Management Review 28 (3): 201–16. [DOI] [PubMed] [Google Scholar]
- Weissert, W. G. , and Scanlon W. J.. 1985. “Determinants of Nursing Home Discharge Status.” Medical Care 23: 333–43. [DOI] [PubMed] [Google Scholar]
- Wodchis, W. P. , Hirth R. A., and Fries B.. 2004. “The Effect of Medicare's Prospective Payment System on Resident Discharge Outcomes of Skilled Nursing Facilities.” Inquiry 41 (4): 418–34. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix SA1: Author Matrix.
Appendix SA2: Characteristics of Nursing Home Resident Sample.