

Abstract
While the renal complications of plasma cell dyscrasia have been well-described, most information in patients with chronic lymphocytic leukemia and monoclonal B-cell lymphocytosis is derived from case reports. This is a retrospective analysis of patients with chronic lymphocytic leukemia or monoclonal B-cell lymphocytosis who underwent kidney biopsy for renal insufficiency and/or nephrotic syndrome. Between January 1995 and June 2014, 49 of 4,024 (1.2%) patients with chronic lymphocytic leukemia (n=44) or monoclonal B-cell lymphocytosis (n=5) had a renal biopsy: 34 (69%) for renal insufficiency and 15 (31%) for nephrotic syndrome. The most common findings on biopsy were: membranoproliferative glomerulonephritis (n=10, 20%), chronic lymphocytic leukemia interstitial infiltration as primary etiology (n=6, 12%), thrombotic microangiopathy (n=6, 12%), and minimal change disease (n=5, 10%). All five membranoproliferative glomerulonephritis patients treated with rituximab, cyclophosphamide and prednisone-based regimens had recovery of renal function compared to 0/3 patients treated with rituximab with or without steroids. Chronic lymphocytic leukemia infiltration as the primary cause of renal abnormalities was typically observed in relapsed/refractory patients (4/6). Thrombotic microangiopathy primarily occurred as a treatment-related toxicity of pentostatin (4/6 cases), and resolved with drug discontinuation. All cases of minimal change disease resolved with immunosuppressive agents only. Renal biopsy plays an important role in the management of patients with chronic lymphocytic leukemia or monoclonal B-cell lymphocytosis who develop renal failure and/or nephrotic syndrome.
Introduction
Chronic lymphocytic leukemia (CLL) is a disease of neoplastic clonal B cells, primarily involving bone marrow, peripheral blood, lymph nodes and other hematopoietic organs such as liver and spleen. “Extramedullary/extranodal” manifestations of CLL are rare, with only 192 cases reported in the literature between 1975 and 2012.1 Such manifestations can occur with or without the presence of systemic CLL, and most often involve the skin (33%) and central nervous system (27%) but rarely the genitourinary and gynecological systems (10%), including the kidneys.1
These data do not take into account asymptomatic organ involvement. In fact, autopsy series indicate that CLL can involve the kidneys, adrenal glands, and pituitary gland without recognized clinical sequela. In particular, up to 90% of patients with CLL and no previous renal abnormalities have some degree of renal interstitial infiltration on autopsy.2–5 Although interstitial CLL infiltration of the kidney can have clinical manifestations, only ten cases of acute renal failure secondary to CLL infiltration have been reported in the literature.2,6–11
Collectively, 81 cases of biopsy-proven glomerular or interstitial renal abnormalities due to CLL have been reported in the literature to date, whereas no cases associated with monoclonal B-cell lymphocytosis (MBL) have been described. Most of these CLL-associated cases are single patient case reports or small case series, with the largest report to date including 15 patients.11–26 Here we report the pathological findings and outcomes of a series of 49 patients with CLL and MBL followed at a single institution, who underwent a kidney biopsy during the course of their disease to evaluate renal insufficiency and/or nephrotic syndrome.
Methods
Study population
The study was reviewed and approved by the Institutional Review Board of the Mayo Clinic and was conducted in accordance with the principles of the Declaration of Helsinki. Between January 1st, 1995 and June 30th 2014, 4,024 patients with CLL, small lymphocytic lymphoma (SLL) or MBL27 were cared for and monitored sequentially in the Division of Hematology at our institution and consented to participate in the Mayo Clinic database. Information regarding the baseline evaluation, medical history, laboratory findings, and prognostic factors were obtained from clinical records. Information on prognostic factors was based on fluorescent in situ hybridization for common CLL chromosome abnormalities, analysis of the mutation status of the IGHV gene, CD38, ZAP70, and CD49d expression determined by flow cytometry.
Renal biopsy and classification
All renal biopsies were reviewed by Mayo Clinic pathologists specializing in evaluation of renal pathology. Collaborative review by Mayo Clinic hematopathologists specializing in review of lymphoid malignancy was also performed in all cases in which co-existent interstitial lymphocytic infiltration was observed. Standard processing of kidney biopsies evaluated at the Mayo Clinic included light microscopy, immunofluorescence, and electron microscopy. For light microscopy, biopsy specimens were stained with hematoxylin-eosin, periodic acid Schiff, Masson trichrome, and Jones methenamine silver. For immunofluorescence, 3-micron cryostat sections were stained with polyclonal fluorescein isothiocyanate-conjugated antibodies to IgG, IgM, IgA, C3, C1q, kappa and lambda light chains, fibrinogen, and albumin (Dako), as per routine clinical testing. Electron microscopy was performed as per clinical routine. Immunohistochemical stains for CD3, CD5, CD20, and CD23 were done in cases of interstitial lymphocytic infiltration (and for PAX5 and CD19 in selected cases) to help assess CLL/SLL involvement.
Renal biopsy findings were further classified according to a potential causal relationship with CLL. Cases of membranoproliferative glomerulonephritis (MPGN), CLL infiltrate as primary etiology, minimal change disease (MCD), acute interstitial nephritis, amyloidosis, light chain cast nephropathy, membranous glomerulonephritis, and unclassified mesangial proliferative glomerulonephritis were considered directly related to CLL. Cases secondary to CLL-associated conditions, such as infections, autoimmune disease, and other cancers, or CLL treatment were considered potentially indirectly related to CLL. Cases secondary to non-CLL associated comorbidities or non-CLL treatment, such as diabetes, hypertension or obesity, were considered unrelated to CLL.
Statistical analysis
Descriptive statistics of baseline characteristics were calculated. The Mann-Whitney test was used for comparisons of medians. Overall survival was defined as time from diagnosis to death or last follow up. Survival curves were calculated using the Kaplan-Meier method, and comparisons were made using the log-rank test. All P-values were two-sided and considered statistically significant if ≤0.05. Statistical analyses were completed using SPSS 21.
Results
Baseline characteristics
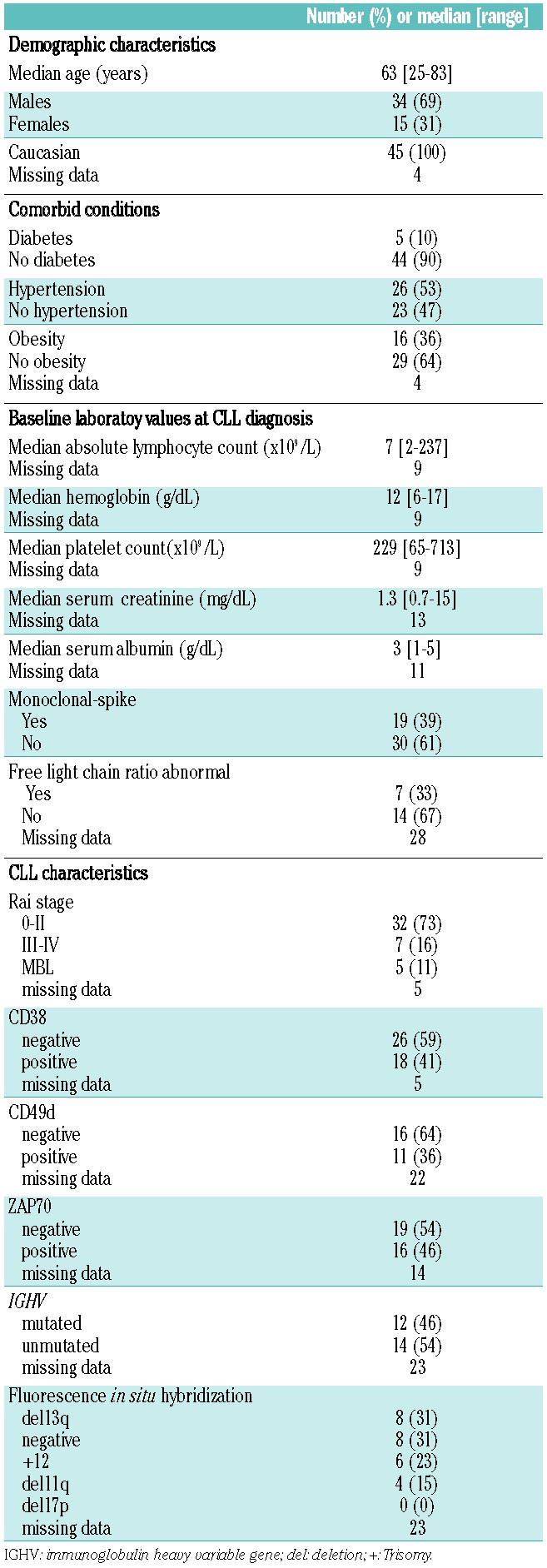
Between January 1st, 1995 and June 30th, 2014, 4,024 patients with CLL, SLL or MBL were followed at our institution. Of these patients, 49 (1.2%) had an ultrasound-guided kidney biopsy during follow-up to evaluate renal failure and/or nephrotic syndrome. Of these biopsies, 10% were performed before 2005, 49% between 2005 and 2010, and 41% after 2010. The indication for renal biopsy was renal insufficiency (without evidence of post-renal compression or tumor lysis) in 34 patients (69%; median creatinine 3.2 mg/dL, range 1.7–15) and nephrotic syndrome in 15 (31%; median proteinuria 11.3 g/24 hours, range 4–54.9). The pertinent baseline characteristics of these 49 patients at the time of CLL diagnosis are shown in Table 1.
Table 1.
Baseline characteristics of 49 CLL cases.
Kidney biopsy results are shown in Table 2. The distribution of renal pathology based on the indication for biopsy is shown in Figure 1. Of interest, among the five patients with MBL the pathologic diagnoses were the following: granulomatous interstitial nephritis, focal segmental glomerulosclerosis, thrombotic microangiopathy (TMA), unclassified mesangial proliferative glomerulonephritis and MPGN.
Table 2.
Pathologic features of 49 CLL cases on renal biopsy.
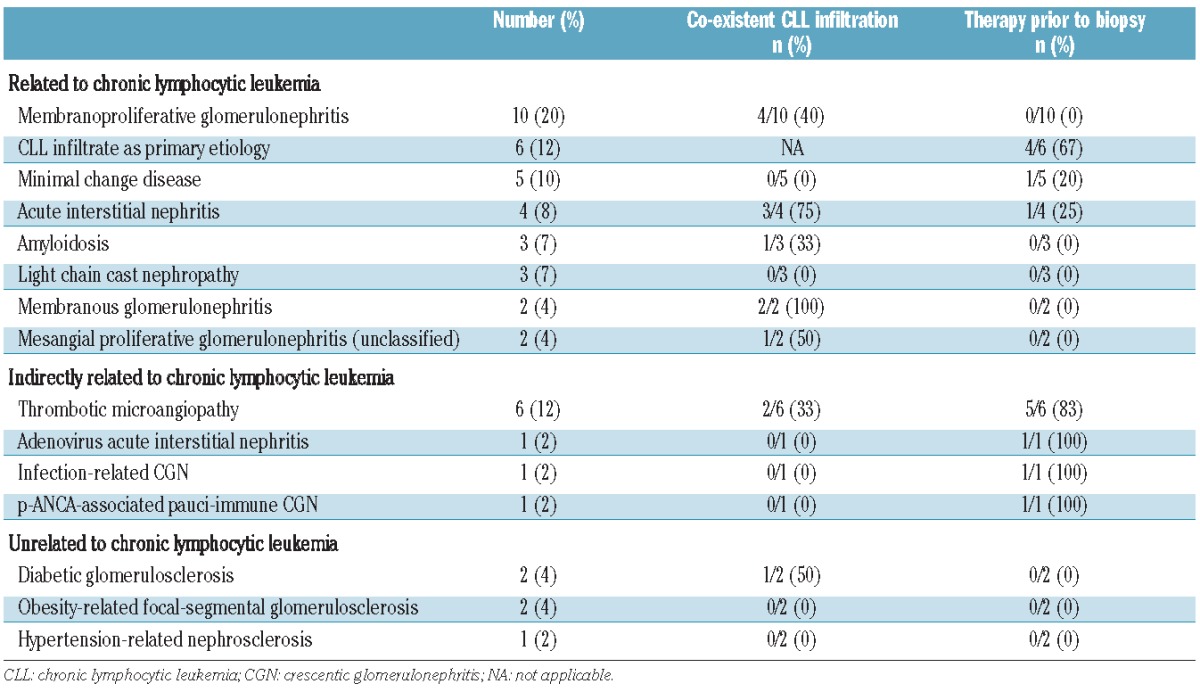
Figure 1.
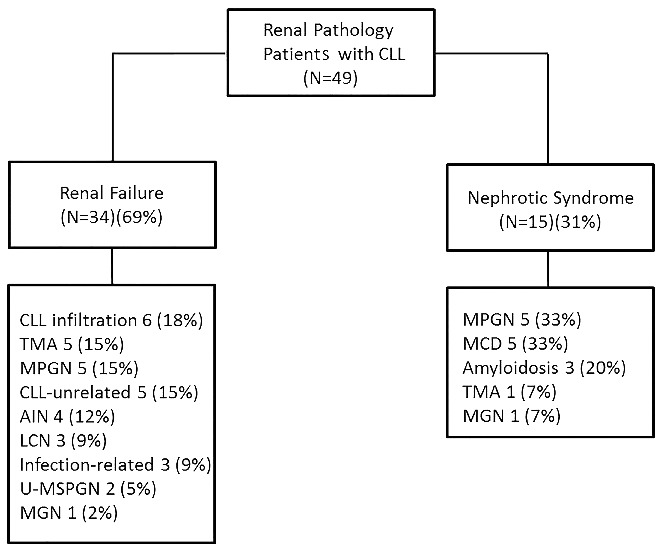
Renal pathology findings by indication for renal biopsy. CLL: chronic lymphocytic leukemia; TMA: thrombotic microangiopathy; MPGN: membranoproliferative glomerulonephritis; AIN: acute interstitial nephritis; LCN: light-chain nephropathy; U-MPGN: unclassified mesangial proliferative glomerulonephritis; MGN: membranous glomerulonephritis; MCD: minimal change disease.
Specific chronic lymphocytic leukemia-related causes of renal pathology
Membranoproliferative glomerulonephritis
Ten patients had an MPGN pattern of glomerular injury on light microscopy (Figure 2A). The characteristics of these patients at the time of CLL diagnosis are shown in Table 3. Based on the findings on light microscopy, immunofluorescence, and electron microscopy and the clinical parameters, the clinicopathological diagnoses in these patients were: (i) proliferative glomerulonephritis with monoclonal IgG deposits in three patients (IgG1 lambda in 2 and IgG kappa in 1), confirmed in two of them also by serum immunofixation; (ii) cryoglobulinemic glomerulonephritis in two patients, only one of whom had a positive serum cryoglobulin test and both with negative hepatitis serological tests; (iii) immunotactoid glomerulonephritis with monoclonal IgG lambda deposits in one patient, who had a depressed serum free kappa to lambda ratio; (iv) fibrillary glomerulonephritis with polyclonal IgG deposits in one patient, who did not have clinical evidence of a paraproteinemia; (v) C3 glomerulonephritis in one patient, who had reduced serum C3 and C4 and negative serum immunofixation; and (vi) unclassified MPGN in two patients (1 due to lack of glomeruli in the immunofluorescence sample and one due to lack of results of immunofluorescence, both with monoclonal protein on serum immunofixation (IgM lambda in 1 and both IgM kappa and IgG lambda in the other).
Figure 2.
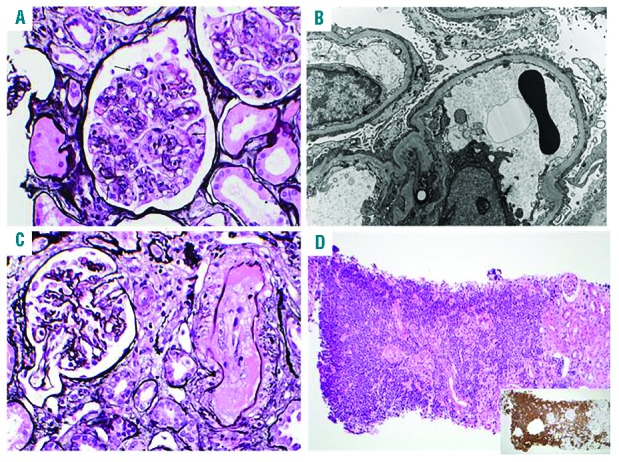
Most common findings on kidney biopsy (MPGN, CLL infiltrate, thrombotic microangiopathy, MCD). (A) MPGN. Glomeruli show mesangial sclerosis, mesangial hypercellularity, and segmental glomerular basement membrane duplication (arrows) associated with cellular interposition (silver stain, X400); (B) MCD. Podocytes show diffuse foot process effacement and segmental microvillus transformation. The glomerular basement membranes appear normal in thickness and texture and are devoid of electron dense immune deposits (X8000). Glomeruli were unremarkable on light microscopy (not shown); (C) thrombotic microangiopathy. The interlobular artery depicted is occluded by endothelial cell swelling and extensive intimal deposition of fibrin which stains pink on silver stain, consistent with arterial thrombosis. The adjacent glomerulus exhibits ischemic-type global thickening and wrinkling of the glomerular basement membrane (silver stain, X400); (D) CLL. Extensive cortical interstitial infiltration by monotonous CLL B cells (H&E, X100), which stain strongly for CD19 (small box, X100). The infiltrate was weakly positive for CD20 and negative for CD3 (not shown).
Table 3.
Baseline characteristics at the time of CLL diagnosis among 27 patients with the four most common pathological findings on kidney biopsy.
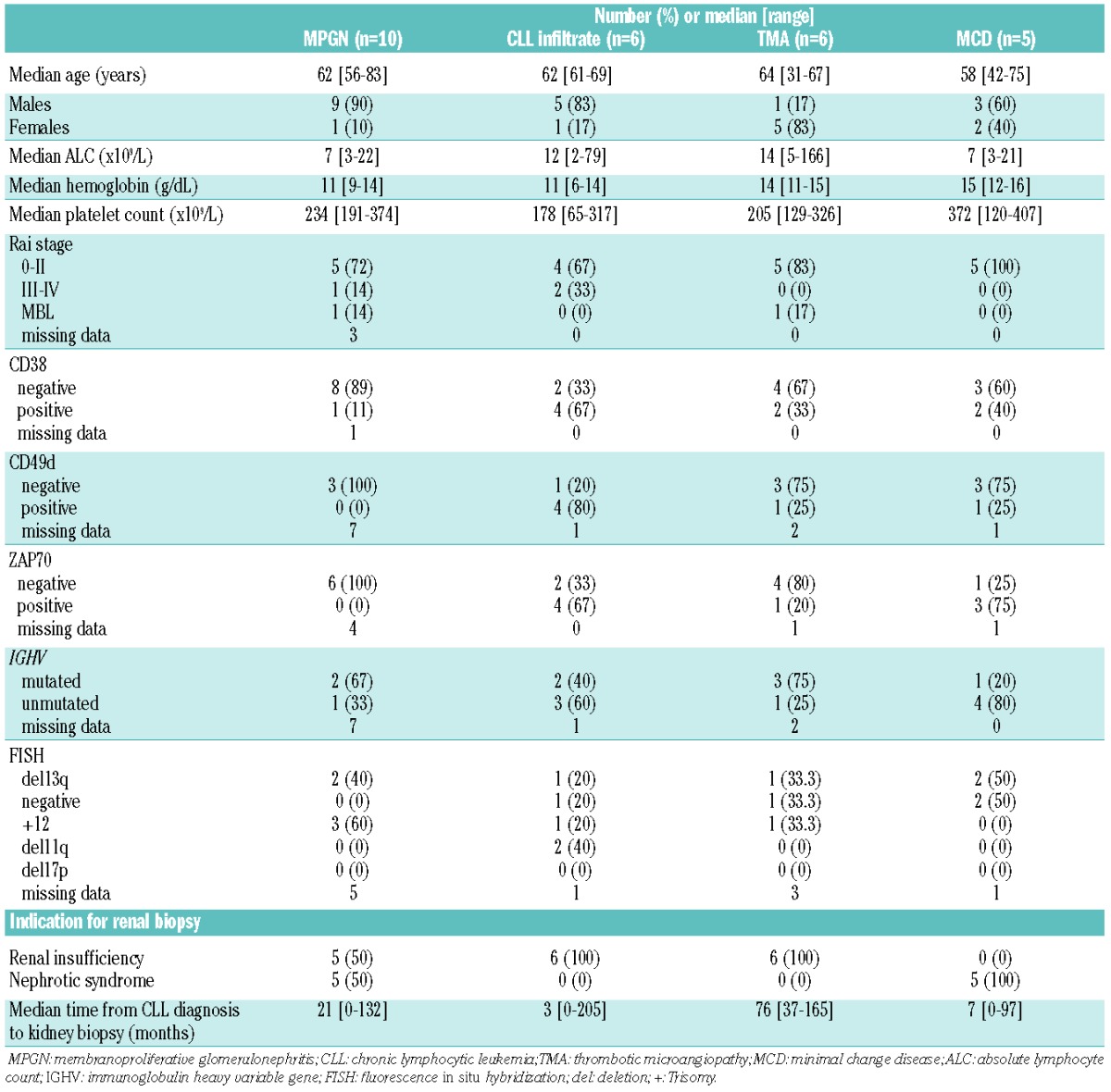
Reasons for renal biopsy in the ten patients with MPGN were equally distributed between renal failure and nephrotic syndrome (5 patients each). Serology for hepatitis B and C virus, and anti-nuclear antibodies were negative in all patients. Four out of the ten cases of MPGN showed some degree of CLL infiltration, either focal or diffuse.
At the time of renal biopsy, none of the patients with MPGN had been previously treated. Two patients did not receive any subsequent therapy despite the MPGN diagnosis: one had an initial creatinine of 2.3 mg/dL and was lost to follow-up, while the other worsened acutely, before treatment for CLL could be started, needed dialysis and eventually received a renal transplant. The remaining eight patients all received CLL-directed therapy within 1 month of renal biopsy. Five were treated with a rituximab, cyclophosphamide and prednisone (RCP)-based regimen (3 with vincristine), and three received a rituximab-based regimen with or without steroids (rituximab with high-dose methylprednisolone in 2 cases, rituximab as a single agent in 1). All five patients treated with RCP-based regimens achieved complete remission of CLL and significant improvement in renal abnormalities, with a median renal and CLL response duration of 32 months (range, 13–75). Only one of these five patients experienced progression of CLL (but no renal relapse) after 40 months of follow-up. Among the three patients treated with rituximab-based regimens with or without steroids, one (with fibrillary glomerulonephritis) had an improvement in his renal abnormalities with rituximab as a single agent, whereas the remaining two (1 with proliferative glomerulonephritis with monoclonal IgG deposits and 1 with cryoglobulinemic glomerulonephritis) did not (1 needed chronic dialysis and eventually proceeded to renal transplant). All patients with MPGN were also conservatively managed with a low salt diet, diuretics and ACE inhibitors.
Chronic lymphocytic leukemia interstitial infiltration
In six patients, CLL infiltration of the kidney was the primary etiology of renal pathology detected on kidney biopsy (Figure 2D). CLL infiltrates were established histologically based on morphology of samples stained with hematoxylin and eosin and on their immunohistochemical profile. CLL cells were small and monotonous and frequently formed dense aggregates in the cortex. They stained positive for CD20, CD23, CD5, CD19, and PAX5, and were negative for CD3. The characteristics of these patients at the time of their CLL diagnosis are shown in Table 3. Of interest, at the time of kidney biopsy, the median absolute lymphocyte count was 3.2×109/L (range 0.2–4.5×109/L), and lymphadenopathy was present in all six patients. In all patients, renal failure (median creatinine 3.1 mg/dL; range, 1.7–8.5) was the reason for renal biopsy. The CLL infiltrate was diffuse (affecting 50–100% of the cortex) in three patients and focal (affecting 20–30% of cortex) in the remaining three. No meaningful difference in creatinine clearance was observed between these two groups (21 versus 32 mL/min; P=0.98). At the time of kidney biopsy, two patients were untreated (the renal pathology and CLL were diagnosed concomitantly), and four had previously received treatment (the renal pathology was diagnosed at a median time of 32 months after the CLL diagnosis; range, 3–205 months).
One patient had a poor performance status and co-morbidity that precluded therapy. This patient needed chronic dialysis and eventually died of CLL disease progression. In the remaining five patients, the renal infiltration and resulting renal failure were felt to be an indication for CLL treatment, and all were subsequently treated within 1 month of renal biopsy. One patient was treated with dose-modified pentostatin, cyclophosphamide and rituximab, with stable disease (11 months), but no improvement in renal function (creatinine clearance stable at 25 mL/min, with no need for dialysis). Of the remaining four patients, two were treated with rituximab, cyclophosphamide, vincristine and prednisone (RCVP), one with rituximab plus high-dose methylprednisolone, and one with ofatumumab plus high-dose methylprednisolone. All achieved a response in their CLL (1 complete remission, 3 partial remissions, and 1 stable disease) and significant improvement in renal function. One patient treated with RCVP is still in remission after 8 years; the other three patients experienced relapse of their CLL after a median of 8 months (range, 6–12 months). Of note, none of these patients experienced recurrence of renal insufficiency at the time of CLL relapse.
Minimal change disease
Five patients were diagnosed with MCD as the primary cause of renal dysfunction (Figure 2B). Their baseline characteristics are shown in Table 3. All patients with MCD had nephrotic syndrome as an indication for renal biopsy. None of these five cases showed any concomitant CLL infiltration in the kidney. Concomitant risk factors for MCD, such as active infection, other cancer, allergy or use of medications associated with MCD, were not present in any of these five patients at the time of kidney biopsy.
At the time of renal biopsy, only one patient with MCD had been previously treated (with 3 different lines of chemo-immunotherapy). The MCD in this patient was subsequently treated with rituximab and prednisone, with resolution of his nephrotic syndrome. The four previously untreated patients received a variety of treatment regimens in an effort to improve the MCD, as it was felt to be CLL-related, including: obinutuzumab and chlorambucil (n=1), RCP (n=1), rituximab as a single agent (n=1), and prednisone alone (n=1). All five patients achieved complete resolution of their nephrotic syndrome. Three of these five patients have had no recurrence in the nephrotic syndrome after a median of 48 months (range, 15–156 months). Two patients developed recurrence of the MCD. The patient treated with rituximab as a single agent had recurrence of MCD after 2 months, despite no evidence of CLL progression. Computed tomography scans at that time revealed a peritoneal mass that on biopsy proved to be a peritoneal mesothelioma. The patient treated with RCP had both CLL progression and recurrence of MCD after 5 months, which were successfully treated with the combination of rituximab and bendamustine (still in remission as of most recent follow-up, 8 months later). All patients with MCD were also conservatively managed with a low salt diet, diuretics and ACE inhibitors.
Other chronic lymphocytic leukemia-related renal biopsy findings
Other less frequently observed CLL-related causes of renal pathology included: acute interstitial nephritis (n=4; manifesting histologically as granulomatous infiltration in 3 out of 4 patients); AL lambda amyloidosis (n=3; CLL expressing surface lambda chain in all patients, none had evidence of co-existent plasma cell neoplasm, only 1 had a detectable IgG lambda serum monoclonal protein on immunofixation); light chain cast nephropathy (n=3; 2 with concomitant plasma cell neoplasm, and CLL/SLL expressing surface kappa chain in all cases; in the only case with no concomitant plasma cell neoplasm, plasma cells in the bone marrow were not increased, and immunofixation showed a IgG kappa serum monoclonal protein); membranous glomerulonephritis (n=2); and unclassified mesangial proliferative glomerulonephritis (n=2).
Potential concomitant risk factors, such as infections, autoimmune processes and second cancers, were not present in any of these cases at the time of renal biopsy.
Causes of renal pathology that were considered to be indirectly related to the chronic lymphocytic leukemia
Thrombotic microangiopathy
TMA was identified as the cause of renal dysfunction on kidney biopsy in six patients (Figure 2C). Their baseline characteristics are shown in Table 3. All patients presented with renal insufficiency. Two of these six patients had concomitant CLL infiltration (either focal or diffuse) on renal biopsy. All patients presented with anemia, thrombocytopenia or schistocytes on peripheral blood smear. ADAMTS 13 levels, obtained only in one patient, were low. None of the affected patients presented with neurological symptoms.
All cases with TMA had co-existent risk factors for microangiopathy, potentially related to CLL, at the time of renal biopsy: recent use of pentostatin (n=4), metastatic lung cancer (n=1), and recent stem cell transplant (n=1). Plasmapheresis was initiated in the patient who had received a stem cell transplant, but it was unsuccessful, and eventually chronic dialysis was needed. All other patients had spontaneous improvement of their renal function with discontinuation of pentostatin or with treatment of the concomitant cancer.
Other causes of renal pathology considered to be indirectly related to the chronic lymphocytic leukemia
Other renal biopsy findings indirectly related to CLL included: adenovirus acute interstitial nephritis (n=1); bacterial infection-associated crescentic glomerulonephritis (n=1, serum anti-streptococcal antibodies negative); and p-ANCA associated pauci-immune crescentic glomerulonephritis, in the context of systemic vasculitis (n=1).
Causes of renal pathology unrelated to chronic lymphocytic leukemia
Causes of renal failure and/or nephrotic syndrome unrelated to CLL included diabetic glomerulosclerosis (n=2), obesity-related focal segmental glomerulosclerosis (n=2), and hypertensive nephrosclerosis (n=1). Of note, only one of these patients had evidence of CLL renal infiltration. These five patients were managed with treatment for the primary etiology in conjunction with a low salt diet, diuretics and ACE inhibitors. Stable renal function was maintained in four of them (1 died of CLL progression), whereas one patient progressed to end-stage renal disease requiring dialysis.
Overall survival among the most common causes of renal pathology
In our study, the four most common renal pathology findings (in at least 5 patients) were MPGN, CLL infiltration as primary etiology, MCD and TMA. After a median follow-up of 60 months (range, 12–216), deaths were reported in 19 (39%) patients including one of ten (10%) patients with MPGN, four of six (66%) patients with CLL infiltration (as the primary etiology of the renal failure), two of six (33%) patients with TMA, and none of five (0%) patients with MCD. The median overall survival was reached only in cases with CLL infiltration (as the primary etiology) and was 84 months (range, 12–206 months). The median overall survival has not been reached in patients with MPGN, MCD and TMA (P=0.28).
Discussion
Renal insufficiency is a relatively common problem among patients with CLL, present in 7.5% of patients at the time of CLL diagnosis and in an additional 16.2% during the course of disease.28 The mechanism of renal failure in such patients varies, but the CLL infiltrate may compress the renal tubules as well as the microvasculature, resulting in intrarenal obstruction and ischemia. Other potential causes of renal insufficiency in patients with CLL include contrast-induced nephropathy, treatment-related tumor lysis, chemotherapy-related toxicity and ureteral obstruction by lymphadenopathy.29 CLL can also be associated with and lead to glomerular pathology, including acute glomerulonephritis, the nephrotic syndrome, and chronic glomerulonephritis. The pathological lesions resulting in these clinical conditions include glomerulonephridites which on light microscopy show mesangioproliferative, membranoproliferative, or endocapillary proliferative glomerulonephritis (e.g., cryoglobulinemic glomerulonephritis, immunotactoid glomerulonephritis, and proliferative glomerulonephritis with monoclonal IgG deposits) and non-proliferative glomerulopathies (e.g., membranous glomerulopathy or MCD). These conditions may be associated with the presence of CLL-related proteins, such as cryoglobulins, monoclonal immunoglobulins, or light chains.29 Since patients with CLL also have an increased risk of infections, second cancers and autoimmune processes, glomerulopathies indirectly related to CLL, such as bacterial infection-associated glomerulonephritis, autoimmune disease associated glomerulonephritis or TMA, can also be observed. Finally, since the median age at diagnosis of CLL is 72 years and comorbid health conditions in patients with CLL are common, renal pathology unrelated to CLL can occur (e.g., diabetic nephropathy, obesity-associated focal segmental glomerulosclerosis, and hypertensive nephrosclerosis).29
Unlike plasma cell dyscrasias, in which kidney biopsy is routinely performed to evaluate unexplained renal insufficiency or nephrotic syndrome,30 and based on available literature, renal biopsies are rarely performed in patients with CLL and are mostly reported as case reports. As a consequence, little is known about the mechanism(s) causing renal abnormalities in CLL. In addition, no cases of renal abnormalities associated with MBL have been reported in the literature. In our series of over 4,000 patients, approximately 1% required renal biopsy during the course of their disease and the biopsy results revealed important etiologies for renal disease in CLL and MBL. In a majority of these 49 patients, the etiology of the renal failure/nephrotic syndrome was either directly (n=35; 71%) or indirectly (n=9; 18%) related to CLL.
MPGN was the most common pathological finding in our study and was equally likely to present as renal insufficiency or nephrotic syndrome. In our series, the glomerular injury in these patients was mediated by direct glomerular deposition of monoclonal protein (such as in cases of proliferative glomerulonephritis with monoclonal IgG deposits and immunotactoid glomerulonephritis), cryoglobulins, and immune-complexes; in one case of C3 glomerulonephritis, indirect damage was potentially mediated through abnormal activation of the alternative complement cascade.31 Similar mechanisms were described in the majority of the 27 cases reported in the literature.11,13,15,16,19,25,26
Treatment of CLL with concomitant renal abnormalities is challenging. In fact, creatinine clearance is one of the strongest predictors of fludarabine toxicity, a mainstay of CLL therapy.32 As a consequence, a variety of alternative regimens have been used to treat CLL-associated MPGN including prednisone, chlorambucil, interferon-alpha, rituximab and bendamustine, and rituximab and cyclophosphamide (with or without vincristine).15,19,25,26,33,34 In our study, rituximab in combination with cyclophosphamide appeared more effective than nonalkylating agent-based regimens for renal pathology complicating CLL. Notably, cyclophosphamide is typically used in the treatment of a number of aggressive glomerulonephritides, though its superiority over other cytostatic drugs has never been proven for MPGN.35 The RCVP regimen has been previously proposed as an effective regimen for the treatment of CLL with co-existent autoimmune cytopenias.36 The ability to selectively suppress the autoimmune process associated with MPGN and to be cytotoxic to CLL without causing further renal toxicity may make RCVP the optimal treatment for this condition.
CLL infiltration of the kidney as the primary etiology of renal failure was the second most common cause of renal pathology in our study. Although reported in up to 90% of CLL patients in autopsy series, only ten cases of CLL infiltration of the kidney causing clinical sequelae have been reported to date.3,4,11 Accordingly, great care must be taken to determine whether CLL cells infiltrating the kidney are or are not the etiology of renal pathology. This determination requires close collaboration between hematologists, nephrologists and pathologists expert in the care of patients with CLL and its effects on the kidney. In our study, two-thirds of patients with CLL infiltration of the kidney as the cause of their renal failure had relapsed refractory CLL. Interstitial infiltration by CLL cells can be confused with acute interstitial nephritis, a much more common lesion in the kidney. On routine histology, the presence of large lymphoid aggregates of monotonous lymphocytes without associated tubulitis favors CLL infiltration. In these cases, immunohistochemical staining for CD3, CD20, CD5, and CD23 are helpful to confirm or exclude CLL infiltration. The treatment of this population is a challenge, particularly if concomitant renal complications are present. Rituximab-based regimens have been proposed in the past as therapy for these patients, given their limited toxicity, but with unsatisfactory results. We also do not know if the novel biological agents, such as B-cell receptor inhibitors or anti-apoptotic drugs, will be able to play a future role in such patients.
TMA was a relatively common etiology for renal abnormalities in our series. No cases of directly CLL-associated TMA have been described in the literature. Consistent with this, all six cases of TMA in our cohort were likely secondary to either CLL treatment (allogeneic stem cell transplantation in 1 case, pentostatin in 4 cases) or potential CLL complications (metastatic cancer in 1 case). Although the association between TMA and metastatic cancer or stem cell transplantation is well recognized,37,38 chemotherapy-induced TMA can be underappreciated, particularly for less frequently used drugs such as pentostatin. Pentostatin is a specific inhibitor of adenosine deaminase providing response frequencies comparable to those of fludarabine but with apparently lower toxicity and greater ease of administration. Although TMA is not a common side effect of pentostatin, three cases have been previously reported.39,40 The precise mechanism of TMA in pentostatin-treated patients is unclear, but all four patients with pentostatin-induced TMA in our series improved with discontinuation of drug, and none required plasma exchange.
MCD was another common etiology of renal pathology observed in our study. The underlying cause of MCD is still unclear, despite accumulating evidence that systemic T-cell dysfunction, with consequent cytokine production, may be involved. The serum levels of interleukin-17A, interferon-γ, interleukin-2, interleukin-10, interleukin-4, and interleukin-21 are significantly higher in patients with MCD than in healthy controls, and this may translate into foot process fusion and consequent nephroticsyn drome.41,42 A similar mechanism has been advocated for MCD complicating B-cell neoplasias, including CLL and other non-Hodgkin lymphomas, in which T-cell dysfunction is a common finding.23,43,44 It should be noted that all cases of MCD in our series presented with the nephrotic syndrome. The immune pathogenesis of MCD in CLL is further supported by the high response rate and response duration reported both in the literature and in our study with the use of immunosuppressive agents, such as prednisone or rituximab-based regimens.13,22,23
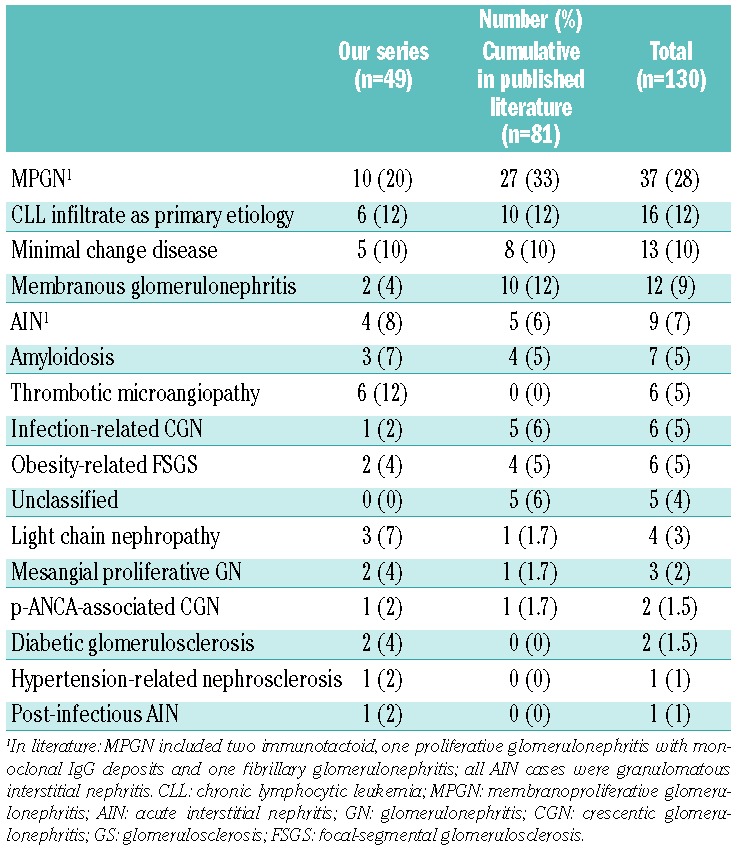
The combination of our series and cases reported in the literature shows that MPGN, CLL infiltration and MCD are the three most common findings in patients with CLL and renal abnormalities (Table 4). Of interest, the addition of our data to the reported literature highlighted the high prevalence of membranous glomerulonephritis. Membranous glomerulonephritis is reported as a frequent cause of nephrotic syndrome in patients with carcinoma but is not typically thought to be associated with lymphoproliferative disorders.45 Nonetheless, cases of membranous glomerulonephritis associated with CLL have been increasingly recognized and, of interest, have been reported to respond to fludarabine as a single agent, emphasizing the importance of recognizing membranous glomerulonephritis in CLL and that treatment of CLL may assist in its resolution.46,47
Table 4.
Features on renal biopsy in Mayo series and published studies.
In conclusion, our findings emphasize that renal abnormalities in patients with CLL may be more common than previously appreciated. CLL patients who develop renal insufficiency without a clear etiology should undergo renal biopsy with review by an expert pathologist with individualization of the management plan formulated by CLL experts in collaboration with nephrologists. In fact, renal biopsy frequently clarifies the mechanism underlying the renal insufficiency and/or the nephrotic syndrome in patients with MBL/CLL, and allows for more effective treatment.
Footnotes
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org. Dr. Shanafelt is a Clinical Scholar of the Leukemia and Lymphoma Society.
References
- 1.Ratterman M, Kruczek K, Sulo S, Shanafelt TD, Kay NE, Nabhan C. Extramedullary chronic lymphocytic leukemia: systematic analysis of cases reported between 1975 and 2012. Leuk Res. 2014;38(3):299–303. [DOI] [PubMed] [Google Scholar]
- 2.Phillips JK, Bass PS, Majumdar G, Davies DR, Jones NF, Pearson TC. Renal failure caused by leukaemic infiltration in chronic lymphocytic leukaemia. J Clin Pathol. 1993;46(12):1131–1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Barcos M, Lane W, Gomez GA, et al. An autopsy study of 1206 acute and chronic leukemias (1958 to 1982). Cancer. 1987;60(4):827–837. [DOI] [PubMed] [Google Scholar]
- 4.Xiao JC, Walz-Mattmuller R, Ruck P, Horny HP, Kaiserling E. Renal involvement in myeloproliferative and lymphoproliferative disorders. A study of autopsy cases. Gen Diagn Pathol. 1997;142(3–4):147–153. [PubMed] [Google Scholar]
- 5.Schwarze EW. Pathoanatomical features of the kidney in myelomonocytic and chronic lymphocytic leukemia. Virchows Arch A Pathol Anat Histol. 1975;368(3):243–251. [DOI] [PubMed] [Google Scholar]
- 6.Rifkin SI. Acute renal failure secondary to chronic lymphocytic leukemia: a case report. Medscape J Med. 2008;10(3):67. [PMC free article] [PubMed] [Google Scholar]
- 7.Uprety D, Peterson A, Shah BK. Renal failure secondary to leukemic infiltration of kidneys in CLL–a case report and review of literature. Ann Hematol. 2013;92(2):271–273. [DOI] [PubMed] [Google Scholar]
- 8.Hewamana S, Pepper C, Jenkins C, Rowntree C. Acute renal failure as the presenting feature of leukaemic infiltration in chronic lymphocytic leukaemia. Clin Exp Nephrol. 2009;13(2):179–181. [DOI] [PubMed] [Google Scholar]
- 9.Erten N, Saka B, Caliskan YK, Besisik S, Karan MA, Tascioglu C. Acute renal failure due to leukaemic infiltration in chronic lymphocytic leukaemia: case report. Int J Clin Pract Suppl. 2005;(147):53–55. [DOI] [PubMed] [Google Scholar]
- 10.Haraldsdottir V, Haanen C, Jordans JG. Chronic lymphocytic leukaemia presenting as renal failure with lymphocytic infiltration of the kidneys. Neth J Med. 1992;41(1–2):64–67. [PubMed] [Google Scholar]
- 11.Poitou-Verkinder AL, Francois A, Drieux F, et al. The spectrum of kidney pathology in B-cell chronic lymphocytic leukemia / small lymphocytic lymphoma: a 25-year multi-center experience. PLoS One. 2015;10(3):e0119156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Inoue T, Sato T, Okada H, et al. Granulomatous interstitial nephritis in chronic lymphocytic leukaemia. Nephrol Dial Transplant. 2010;25(12):4107–4109. [DOI] [PubMed] [Google Scholar]
- 13.Da’as N, Polliack A, Cohen Y, et al. Kidney involvement and renal manifestations in non-Hodgkin’s lymphoma and lymphocytic leukemia: a retrospective study in 700 patients. Eur J Haematol. 2001;67(3):158–164. [DOI] [PubMed] [Google Scholar]
- 14.Yahata N, Kawanishi Y, Okabe S, et al. Membranous glomerulonephritis with nephrotic syndrome associated with chronic lymphocytic leukemia. Am J Nephrol. 2000;20(5):402–407. [DOI] [PubMed] [Google Scholar]
- 15.Mutluay R, Aki SZ, Erten Y, et al. Membranoproliferative glomerulonephritis and light-chain nephropathy in association with chronic lymphocytic leukemia. Clin Nephrol. 2008;70(6):527–531. [DOI] [PubMed] [Google Scholar]
- 16.Hill PA, Firkin F, Dwyer KM, Lee P, Murphy BF. Membranoproliferative glomerulonephritis in association with chronic lymphocytic leukaemia: a report of three cases. Pathology. 2002;34(2):138–143. [DOI] [PubMed] [Google Scholar]
- 17.Kamat AV, Goldsmith D, O’Donnell P, van der Walt J, Carr R. Renal failure with granulomatous interstitial nephritis and diffuse leukemic renal infiltration in chronic lymphocytic leukemia. Ren Fail. 2007;29(6):763–765. [DOI] [PubMed] [Google Scholar]
- 18.Dou X, Hu H, Ju Y, et al. Concurrent nephrotic syndrome and acute renal failure caused by chronic lymphocytic leukemia (CLL): a case report and literature review. Diagn Pathol. 2011;6:99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Barbour SJ, Beaulieu MC, Zalunardo NY, Magil AB. Proliferative glomerulonephritis with monoclonal IgG deposits secondary to chronic lymphocytic leukemia. Report of two cases. Nephrol Dial Transplant. 2011;26(8):2712–2714. [DOI] [PubMed] [Google Scholar]
- 20.Pamuk GE, Uyanik MS, Demir M, Tekgunduz E, Turgut B, Soy M. Systemic antineutrophil cytoplasmic antibody vasculitis in a patient with chronic lymphocytic leukemia: quite a rare diagnosis. Leuk Res. 2007;31(8):1149–1151. [DOI] [PubMed] [Google Scholar]
- 21.Henriksen KJ, Hong RB, Sobrero MI, Chang A. Rare association of chronic lymphocytic leukemia/small lymphocytic lymphoma, ANCAs, and pauci-immune crescentic glomerulonephritis. Am J Kidney Dis. 2011;57(1):170–174. [DOI] [PubMed] [Google Scholar]
- 22.Aslam N, Nseir NI, Viverett JF, Bastacky SI, Johnson JP. Nephrotic syndrome in chronic lymphocytic leukemia: a paraneoplastic syndrome? Clin Nephrol. 2000;54(6):492–497. [PubMed] [Google Scholar]
- 23.Alzamora MG, Schmidli M, Hess U, Cathomas R, von Moos R. Minimal change glomerulonephritis in chronic lymphocytic leukemia: pathophysiological and therapeutic aspects. Onkologie. 2006;29(4):153–156. [DOI] [PubMed] [Google Scholar]
- 24.Arampatzis S, Giannakoulas N, Liakopoulos V, et al. Simultaneous clinical resolution of focal segmental glomerulosclerosis associated with chronic lymphocytic leukaemia treated with fludarabine, cyclophosphamide and rituximab. BMC Nephrol. 2011;12:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Seney FD, Jr, Federgreen WR, Stein H, Kashgarian M. A review of nephrotic syndrome associated with chronic lymphocytic leukemia. Arch Intern Med. 1986;146(1): 137–141. [PubMed] [Google Scholar]
- 26.Moulin B, Ronco PM, Mougenot B, Francois A, Fillastre JP, Mignon F. Glomerulonephritis in chronic lymphocytic leukemia and related B-cell lymphomas. Kidney Int. 1992;42(1):127–135. [DOI] [PubMed] [Google Scholar]
- 27.Hallek M, Cheson BD, Catovsky D, Caligaris-Cappio F, Dighiero G, Dohner H, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12):5446–5456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Shanafelt TD, Rabe KG, Hanson CA, et al. Renal disease in patients with chronic lymphocytic leukemia (CLL). Blood. 2013;122(21):abstr. [Google Scholar]
- 29.Hricik DE, Chung-Park M, Sedor JR. Glomerulonephritis. N Engl J Med. 1998;339(13):888–899. [DOI] [PubMed] [Google Scholar]
- 30.Fermand JP, Bridoux F, Kyle RA, Kastritis E, Weiss BM, Cook MA, et al. How I treat monoclonal gammopathy of renal significance (MGRS). Blood. 2013;122(22):3583–3590. [DOI] [PubMed] [Google Scholar]
- 31.Sethi S, Fervenza FC, Zhang YZ, Nasr SH, Leung N, Vrana J, et al. Proliferative Glomerulonephritis secondary to dysfunction of the alternative pathway of complement. Clin J Am Soc Nephrol. 2011;6(5): 1009–1017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Martell RE, Peterson BL, Cohen HJ, et al. Analysis of age, estimated creatinine clearance and pretreatment hematologic parameters as predictors of fludarabine toxicity in patients treated for chronic lymphocytic leukemia: a CALGB (9011) coordinated intergroup study. Cancer Chemother Pharmacol. 2002;50(1):37–45. [DOI] [PubMed] [Google Scholar]
- 33.Bartel C, Obermuller N, Rummel MJ, Geiger H, Hauser IA. Remission of a B cell CLL-associated membranoproliferative glomerulonephritis type I with rituximab and bendamustine. Clin Nephrol. 2008;69(4):285–289. [DOI] [PubMed] [Google Scholar]
- 34.Nakayama S, Yabe H, Nagai K. [Nephrotic syndrome associated with B-cell chronic lymphocytic leukemia successfully treated with interferon-alpha]. Rinsho Ketsueki. 1990;31(12):1924–1928. [PubMed] [Google Scholar]
- 35.Faedda R, Satta A, Tanda F, Pirisi M, Bartoli E. Immunosuppressive treatment of membranoproliferative glomerulonephritis. Nephron. 1994;67(1):59–65. [DOI] [PubMed] [Google Scholar]
- 36.Bowen DA, Call TG, Shanafelt TD, et al. Treatment of autoimmune cytopenia complicating progressive chronic lymphocytic leukemia/small lymphocytic lymphoma with rituximab, cyclophosphamide, vincristine, and prednisone. Leuk Lymphoma. 2010;51(4):620–627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ducos G, Mariotte E, Galicier L, et al. Metastatic cancer-related thrombotic microangiopathies: a cohort study. Future Oncol. 2014;10(10):1727–1734. [DOI] [PubMed] [Google Scholar]
- 38.Nadir Y, Brenner B. Thrombotic complications associated with stem cell transplantation. Blood Rev. 2012;26(5):183–187. [DOI] [PubMed] [Google Scholar]
- 39.Harris DC, Lawrence S, Bradstock KF, Carter JJ, Jones WG. Intraglomerular thrombosis with deoxycoformycin–reversible acute renal failure. Clin Nephrol. 1984;21(3):194–196. [PubMed] [Google Scholar]
- 40.Leach JW, Pham T, Diamandidis D, George JN. Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome (TTP-HUS) following treatment with deoxycoformycin in a patient with cutaneous T-cell lymphoma (Sezary syndrome): a case report. Am J Hematol. 1999;61(4):268–270. [DOI] [PubMed] [Google Scholar]
- 41.Shalhoub RJ. Pathogenesis of lipoid nephrosis: a disorder of T-cell function. Lancet. 1974;2(7880):556–560. [DOI] [PubMed] [Google Scholar]
- 42.Zhang N, Zhao P, Shrestha A, et al. A higher frequency of CD4(+)CXCR5(+) T follicular helper cells in adult patients with minimal change disease. Biomed Res Int. 2014;2014:836157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jhaveri KD, Shah HH, Patel C, Kadiyala A, Stokes MB, Radhakrishnan J. Glomerular diseases associated with cancer, chemotherapy, and hematopoietic stem cell transplantation. Adv Chronic Kidney Dis. 2014;21(1): 48–55. [DOI] [PubMed] [Google Scholar]
- 44.Scrivener S, Goddard RV, Kaminski ER, Prentice AG. Abnormal T-cell function in B-cell chronic lymphocytic leukaemia. Leuk Lymphoma. 2003;44(3):383–389. [DOI] [PubMed] [Google Scholar]
- 45.Eagen JW. Glomerulopathies of neoplasia. Kidney Int. 1977;11(5):297–303. [DOI] [PubMed] [Google Scholar]
- 46.Butty H, Asfoura J, Cortese F, Doyle M, Rutecki G. Chronic lymphocytic leukemia-associated membranous glomerulopathy: remission with fludarabine. Am J Kidney Dis. 1999;33(2):E8. [DOI] [PubMed] [Google Scholar]
- 47.Rocca AR, Giannakakis C, Serriello I, Guido G, Mosillo G, Salviani C. Fludarabine in chronic lymphocytic leukemia with membranous nephropathy. Ren Fail. 2013;35(2): 282–285. [DOI] [PubMed] [Google Scholar]