

Abstract
Objectives:
To investigate the effects of air-lock technique (ALT) on pain of intramuscular (IM) injection delivered to the ventrogluteal and dorsogluteal site (DS).
Methods:
A randomized controlled trial design was used to assess the pain intensity associated with IM injections administered using 2 different methods and injection sites. Recruitment of patients was carried out between April and August 2013 at the Department of Brain Surgery, Cekirge State Hospital, Bursa, Turkey. The sample comprised 60 patients who developed no complications at the IM site, and had no illness that could affect their perception of pain. The patients were randomly divided into 2 groups of 30 patients. Patients in the first group received injections in the ventrogluteal site (VS), while the DS was used for injections in the second group. Patients in each group received 2 injections, one using ALT and one not using the technique. After each injection, the pain felt by patients during the injection was immediately assessed using a visual analog scale.
Results:
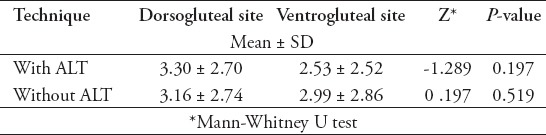
The mean pain score after injections to the DS by the ALT was 3.30 ± 2.70, while the mean pain score after injections to the VS using the same technique was 2.53 ± 2.52.
Conclusion:
Although the difference between groups was not significant, the results of the study supported the idea that injections delivered to the VS by ALT are less painful than those delivered to the DS.
Drugs are delivered via many routes, such as orally, topically, and parenterally.1 One of the techniques for parenteral drug delivery is intramuscular (IM) injection, and one of the sites for this is the large muscle masses.2 Intramuscular injection is a technique, which causes the patient pain and discomfort.3-5 According to the results of one study,6 40% of patients receiving IM drug injections rate it as a very painful process. In the administration of IM injections, the choice of a reliable injection site and injection technique are important factors in the reduction of pain arising from IM injection. In the literature, it has been stated that one site used for IM injection, the dorsogluteal site (DS), is rich in blood vessels, is close to the sciatic nerve, and has a thicker layer of subcutaneous tissue than other sites, making it the most risky site, while the ventrogluteal site (VS) can be safely used instead.1,7-10 The dorsogluteal area, which is frequently preferred by health professionals has been reported to be the most risky area for IM injection.10 If the injection site is not chosen correctly, very serious complications may result.7,8 It is accepted that the VS is safer for injections and causes less pain, because there are no large blood vessels and nerves in the area, and it is distant from bony tissue. This area has the added advantages that the subcutaneous layer here is thin, the necessary position for the patient is easy, and the probability of the medication being delivered to the subcutaneous tissue is low.11-13 Although the literature identifies the VS as the safest site for IM injections, studies have shown that most health professionals do not use this site and are unwilling to change; in addition, although they are aware of the complications that can arise from the use of the DS, they do not give up in using this site.11,12 A study in Turkey14 showed that 60% of nurses always used the DS for IM injections. At the same time, it is believed that the air-lock technique (ALT) used in the administration of IM injections reduces tissue trauma, and reduces pain at the time of injection by preventing the medication from reaching the subcutaneous tissue.9 In a study carried out by Mac Gabhann15 it was stated that the ALT was found to be effective in reducing discomfort due to IM techniques. Najafidolatabad et al16 reported that the ALT was effective in reducing the pain felt after IM injection. It was observed that there are very few studies examining the effectiveness of reduction of IM-induced pain in the dorsogluteal and ventrogluteal injection regions, and the ALT applied there. Besides, it was found that the results of existing studies were not up to date. In this study, we aim to investigate the effects of ALT on the pain of IM injections delivered to the ventrogluteal and DS. This research was conducted for the purpose of providing additional data to practitioners at the level of clinical evidence, and contribute to the literature in light of the current data.
Methods
A randomized controlled trial design was used to assess pain intensity associated with IM injections administered using 2 different methods and injection sites. The present study was designed to investigate the effect of ALT on pain of IM injections delivered to the ventrogluteal and DS. The study was approved by the Ethics Committee of Uludag University, Bursa, Turkey following the guidelines set for the use of human subjects under the Helsinki Declaration. All participants were given information on the study before participating, and patient’s provided written informed consent before voluntary participation. For this trial, the recruitment of patients was carried out between April and August 2013 at the Department of Brain Surgery, Cekirge State Hospital Bursa in the western region of Turkey. The participants were those who had been admitted to the hospital and had previously been prescribed diclofenac sodium by the attending physician to be administered intramuscularly at least every 24 hours. In the center where the survey was conducted, only patients who had been prescribed diclofenac sodium intramuscularly were included. Inclusion criteria of patients in the study were being over 18 years of age, establishing a correct assessment of pain, had been diagnosed intervertebral disc herniation, and have not received any analgesic for at least 6 hours. Exclusion criteria were based on the following points: patients diagnosed with any disease that influenced pain perception, and those who had any illness in their extremities, which would prevent them from taking up any required position. Sixty patients were included in the study after screening for suitability. Patients were randomized into 2 groups with 30 patients each, according to age and gender. The first group received injections to the DS with the use of ALT and one not using the technique, and the second group were injected in the VS with the use of ALT and one not using the technique. In the selection of the injection method, a simple randomization method was used. The sample size was statistically determined using Power Analysis. Results showed for the sample size 0.80 power and 0.05 type I error was 56.
Instruments
In the data collection, a self-administered questionnaire was used. This questionnaire consisted of 2 parts. The first part included items on age, gender, body mass index (BMI), and disease. The second part contained a visual analog scale (VAS) that was used to measure the perceived pain intensity during IM. Immediately following each injection, VAS was given to the patients and they were asked to mark a point on the line that best represented their pain at the time of injection. The distance from ‘no pain’ to the patient’s mark was then measured in centimeters - this was the VAS score (0-10). Zero represents no pain, and 10 represents the worst imaginable pain on this scale.17
Data collection
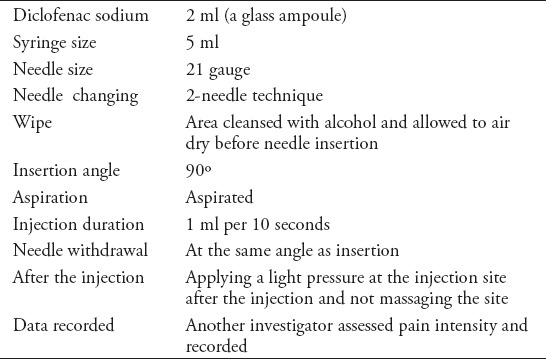
Subjects who satisfied the criteria were recruited, and were required to receive 2 doses of diclofenac sodium. The injection was applied to the DS with the patient in a prone position and the extremities held in a position of internal rotation. The researcher located the DS and the injection was administered into the gluteus maximus at the upper outer portion above the line. The injection was administered to the VS with the patient in a lateral position, the extremities which were uppermost brought into flexion and the extremities, which were below placed forwards. The VS was located by putting the palm of the right hand on the left greater trochanter of the patient so that the index finger pointed towards the anterior superior iliac spine. After that, the injection was administered to the center of this site. Patients were randomized into 2 groups for injections to the dorsogluteal or ventrogluteal regions. The randomized patients in both groups were injected twice in the right or left injection region, with and without using the ALT. Each patient’s left or right injection region was randomized for the 2 injection methods, with or without using the ALT. In the ALT, the dose of medication that was to be administered to the patient was first drawn into the syringe, and then 0.5 ml of air was added. During the administration of the injection, the full dose of medication was delivered to the injection site, followed by a bubble of air. After each injection, another researcher who was unaware of the injection method recorded the pain intensity on the data collection form by having the pain intensity felt by the patient after the injection marked on the VAS. Similar IM injection protocols were administered for all participants. The protocol was designed as shown in Table 1.
Table 1.
Intramuscular injection protocol for all participants and techniques.
Statistical analysis was performed using the Statistical Package for Social Sciences version 18 software (SPSS Inc., Chicago, IL, USA). Numerical and percentage distribution of sociodemographic data on patients’ identification characteristics were calculated. Conformity of numerical data to normal distribution was examined with the Kolmogorov-Smirnov test. Non-parametric testing was used in the analysis of such data as the numerical data did not fit normal distribution. The variations in age, gender, and BMI in the 2 groups and the difference in mean pain scores after the injections were analyzed using the Mann-Whitney U test. The level of significance was set at p<0.05.
Results
It was determined that 53.3% of the patients who received the injections to the DS were female, with a mean age of 46.23 ± 13.33, and mean BMI of 26.71 ± 4.74. Of those who received the injection to the VS, 63.3% were female, with mean age of 49.66 ± 11.83, and mean BMI of 27.67 ± 4.36. Results of the statistical analysis showed that there was no statistically significant difference in age (p=0.296), gender (p=0.600), or BMI (p=0.375) between the 2 groups of patients. The pain scores of the patients after injections were administered to the DS and VS, with or without using ALT are shown in Table 2. The results of the statistical analysis showed that there was no statistically significant difference between the average pain scores for all injections received by patients in either group (p>0.05, Table 2).
Table 2.
Comparison of mean pain scores of injection-site groups by use of air-lock technique (ALT).
Discussion
According to the results, there was no difference between the 2 groups to whom injections were given by the 2 different methods at the DS and VS in terms of independent variables such as age, gender, or BMI. It can be seen from these results that the patients had similar characteristics and that this did not affect the results of the study. Although the difference did not reach statistical significance, the mean pain scores of patients who received injections at the DS were higher than those of the other group of patients (Table 2). In the literature, the DS is reported as the most risky site for IM injections because it is rich in blood vessels, it is close to the sciatic nerve, and the subcutaneous tissue is thicker there than at other sites, while the VS is suggested as a more secure alternative.7-11,18-20
In a study by Gunes et al,21 it was established that patients’ mean pain scores after injections to the DS were higher than those of patients who had received injections to the VS. Similarly, Moharreri et al22 reported that injections to the VS caused less pain and bleeding than those to the DS. In accordance to these results, the results of our present study support the literature.
The results of our study showed that patients who received injections to the VS had higher mean pain scores when the ALT was used than when it was not used, while the patients who received injections to the DS showed the opposite result (Table 2). In the literature, it is asserted that the use of ALT reduces tissue trauma, and the pain felt during injection.9,15 Najafidolatabad et al16 in a study comparing the 2 injection techniques reported that pain experienced after injections using ALT was less. On the other hand, it was reported in a study by Ehsani et al23 that the ALT had no effect on reducing the pain of injection. The results of our study showed support for the literature in the case of patients who received ventrogluteal injections. However, the opposite result for patients who received dorsogluteal injections suggests that since the thickness of the subcutaneous tissue is greater at the DS than at the VS, and that it is less suitable than the VS for injections, it is possible that the ALT has no effect on pain of injections at that site.
Intramuscular injections, which are frequently performed by health professionals in clinics are common painful parts of routine health care. Improper injection techniques can lead to pain and increase the risk of patient’s injury associated with IM injections. Thus, good injection technique can make the experience relatively painless for the patient. Intramuscular injections of diclofenac sodium should preferably be administered to the VS using the ALT. This study provides empirical data for evidence-based nursing and contributes in helping health care professionals reduce injection pain.
This study has some limitations. First, since the research was only conducted on patients with intervertebral disc herniation, it is not possible to generalize the results of the research. The second limitation of the study is that while injection region and ALT were examined, the effect on pain complications and the effect on other complications were not examined.
In conclusion, the results of the study showed that the mean pain scores of patients in the group, which received injections to the VS by both techniques, were lower than those of patients who received injections to the DS. In addition, it was established that the process of injection to the VS by ALT was less painful than when the injection was given without the use of that technique. In light of these results, we recommend that IM injections of diclofenac sodium should be given at the VS, preferably using the ALT. We recommend that the study results should be generalized by repetition with larger sample and with healthy human subjects in groups with different ages, gender, and BMIs.
Acknowledgment
The authors gratefully acknowledge Alexander M. Rylands, M. A., of the Foreign Languages Department of Ege University, Turkey for translating this article. We would like to thank Alexander M. Rylands and all the patients who took part in the study.
Footnotes
Withdrawal policy.
By submission, the author grants the journal right of first publication. Therefore, the journal discourages unethical withdrawal of manuscript from the publication process after peer review. The corresponding author should send a formal request signed by all co-authors stating the reason for withdrawing the manuscript. Withdrawal of manuscript is only considered valid when the editor accepts, or approves the reason to withdraw the manuscript from publication. Subsequently, the author must receive a confirmation from the editorial office. Only at that stage, authors are free to submit the manuscript elsewhere.
No response from the authors to all journal communication after review and acceptance is also considered unethical withdrawal. Withdrawn manuscripts noted to have already been submitted or published in another journal will be subjected to sanctions in accordance with the journal policy. The journal will take disciplinary measures for unacceptable withdrawal of manuscripts. An embargo of 5 years will be enforced for the author and their co-authors, and their institute will be notified of this action.
References
- 1.Nicoll LH, Hesby A. Intramuscular injection: an integrative research review and guideline for evidence-based practice. Appl Nurs Res. 2002;15:149–162. doi: 10.1053/apnr.2002.34142. [DOI] [PubMed] [Google Scholar]
- 2.Tugrul E, Denat Y. Nurses ventrogluteal field injection practices related to knowledge, opinions and practices. Journal of Dokuz Eylul University Faculty of Nursing. 2014;7:275–284. [Google Scholar]
- 3.Engstrom JL, Giglio NN, Takacs SM, Ellis MC, Cherwenka DI. Procedures used to prepare and administer intramuscular injections: a study of infertility nurses. J Obstet Gynecol Neonatal Nurs. 2000;29:159–168. doi: 10.1111/j.1552-6909.2000.tb02036.x. [DOI] [PubMed] [Google Scholar]
- 4.Celik N, Khorshid L. The use of ShotBlocker for reducing the pain and anxiety associated with intramuscular injection: a randomized, placebo controlled study. Holist Nurs Pract. 2015;29:261–271. doi: 10.1097/HNP.0000000000000105. [DOI] [PubMed] [Google Scholar]
- 5.Kanika K, Prasad S. Effect of massage on pain perception after administration of intramuscular injection among adult patients. Nursing and Midwifery Research Journal. 2011;3:130–138. [Google Scholar]
- 6.Cupitt M, Kasipandian V. Pain and intramuscular injections. Anaesthesia. 2004;59:88–99. doi: 10.1111/j.1365-2044.2004.03589.x. [DOI] [PubMed] [Google Scholar]
- 7.Small S. Preventing sciatic nerve injury from intramuscular injections: literature review. J Adv Nurs. 2004;47:287–296. doi: 10.1111/j.1365-2648.2004.03092.x. [DOI] [PubMed] [Google Scholar]
- 8.Malkin B. Are techniques used for intramuscular injection based on research evidence? Nurs Times. 2008;104:48–51. [PubMed] [Google Scholar]
- 9.Rodger MA, King L. Drawing up and administering intramuscular injections: a review of the literature. J Adv Nurs. 2000;31:574–582. doi: 10.1046/j.1365-2648.2000.01312.x. [DOI] [PubMed] [Google Scholar]
- 10.Wynaden D, Landsborough I, McGowan S, Baigmohamad Z, Finn M, Pennebaker D. Best practice guidelines for the administration of intramuscular injections in the mental health setting. Int J Ment Health Nurs. 2006;15:195–200. doi: 10.1111/j.1447-0349.2006.00423.x. [DOI] [PubMed] [Google Scholar]
- 11.Donaldson C, Green J. Using the ventrogluteal site for intramuscular injection. Nurs Times. 2005;101:36–38. [PubMed] [Google Scholar]
- 12.Greenway K. Using the ventrogluteal site for intramuscular injection. Nurs Stand. 2004;18:39–42. doi: 10.7748/ns2004.03.18.25.39.c3560. [DOI] [PubMed] [Google Scholar]
- 13.Hunter J. Intramuscular injection techniques. Nurs Stand. 2008;22:35–40. doi: 10.7748/ns2008.02.22.24.35.c6413. [DOI] [PubMed] [Google Scholar]
- 14.Gunes UY, Zaybak A, Bicici B, Cevik K. The examination of the procedures regarding to intramuscular injection used by the nurses. Journal of Ataturk University School of Nursing. 2009;12:84–90. [Google Scholar]
- 15.Mac Gabhann L. A comparison of two depot injection techniques. Nurs Stand. 1998;12:39–41. doi: 10.7748/ns1998.06.12.37.39.c2512. [DOI] [PubMed] [Google Scholar]
- 16.Najafidolatabad SH, Malekzadeh J, Mohebbinovbandegani Z. Comparison of the pain severity, drug leakage and ecchymosis rates caused by the application on tramadol intramuscular injection in Z-track and air-lock techniques. Investigación y Educación en Enfermería. 2010;28:171–175. [Google Scholar]
- 17.Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of intermittent and Constant Osteoarthritis Pain (ICOAP) Arthritis Care Res (Hoboken) 2011;63:240–252. doi: 10.1002/acr.20543. [DOI] [PubMed] [Google Scholar]
- 18.Kara D, Uzelli D, Karaman D. Using ventrogluteal site in intramuscular injections is a priority or an alternative? International Journal of Caring Sciences. 2015;8:507–513. [Google Scholar]
- 19.Greenway K. Rituals in nursing: intramuscular injections. J Clin Nurs. 2014;23:3583–3588. doi: 10.1111/jocn.12627. [DOI] [PubMed] [Google Scholar]
- 20.Gunes UY, Zaybak A, Tamsel S. The examination of the reliability of the method used in identifying of ventrogluteal site. Journal of Cumhuriyet University School of Nursing. 2008;12:1–8. [Google Scholar]
- 21.Gunes UY, Kara D, Arı S, Ceyhan O. Which site is more painful in intramuscular injections? The dorsogluteal site or ventrogluteal site? A case study from Turkey. Clinical Nursing Studies. 2013;1:74–81. [Google Scholar]
- 22.Moharreri AR, Nasiri H, Jahanshahi M, Rahmani H, Abdollahi A, Rabiei M. The comparison of pain intensity and rate of bleeding in intramuscular injection in dorsogluteal and ventrogluteal area. Journal of Gorgan University of Medical Sciences. 2007;9:37–41. [Google Scholar]
- 23.Ehsani M, Hatamipour KH, Sedaghatı M, Ghanbari A. A comparative study on pain severity caused by Z-track and air lock methods for intramuscular injection. Journal of Ardabil University of Medical Sciences. 2012;11:309–315. [Google Scholar]