

Abstract
Objectives:
To investigate the association between stress, shift work, and eating behavior among non-Saudi female nurses working in Central Saudi Arabia.
Methods:
A sample of 395 non-Saudi female nurses from 2 major hospitals in Riyadh, Kingdom of Saudi Arabia participated in this cross-sectional study. The nurses completed a questionnaire from November 2013 to January 2014 that included items relating to stress and eating behavior using the Dutch Eating Behavior Questionnaire (DEBQ). The questionnaire also contained items pertaining to socio-demographic data, body mass index, shift work, and hours worked per week.
Results:
For all eating styles, stress, and shift duty influenced the amount of food nurses consumed, but was more significant under a restrained eating style. Under this eating style, a significantly higher percentage of nurses reported eating more fast food, snacks, and binging, while fruits and vegetables were the least likely to be eaten under stress. High stressed nurses were more likely to present with abnormal restrained eating (odds ratio [OR]=1.52, p=0.004), emotional (OR=1.24; p=0.001), and external (OR=1.21; p=0.001) DEBQ scores. Working nighttime shift duty was positively associated with restrained eating (OR=1.53; p=0.029) and emotional eating (OR=1.24; p=0.001), but negatively associated with external eating (OR=0.45; p=0.001).
Conclusion:
Our findings suggest that stress and shift duty were associated with eating habits.
Kingdom of Saudi Arabia (KSA) has committed enormous resources to improving health care, with the ultimate goal of providing free and accessible health care services. The Kingdom currently faces a chronic shortage of local nurses. In 2013, Saudi nurses comprised 25% of the total nurse workforce.1 This shortage, as well as the expansion in public and private health care sectors, has contributed to an increased demand for expatriate nurses from different countries. For example, nurses come from over 40 different countries, including the Philippines, Sudan, United Kingdom, Ireland, India, and USA.2,3 Stress and shift work are both factors that influence nurses’ eating behavior. The mechanism through which stress influences food choices involves hormonal interactions and metabolic processes, as well as individual differences in psychological and neurochemical response to stress and eating.4,5 Stress is associated with reduced levels of insulin and leptin, which interact to bring about changes in appetite. Stress elicits a more passive response driven by the hypothalamic pituitary adrenal, with an increase in cortisol that may entice people to consume hedonic, energy-dense foods and potentially lead to unwanted weight gain and obesity.5-7 Research has indicated that work-related stress induces consumption of foods that are high in sugar, fat, and salt, and a decrease in the consumption of fruits, vegetables, and fiber.8-11 Emotional eating under stress was associated with a higher intake of sweets and negatively associated with fruit and vegetable intake, and it was found to occur in people with poor coping skills, poor interceptive awareness, and high alexithymia.12-15 Restrained eaters ate more than usual or binged under stress and increased their intake of fatty and sugary foods. External eating under stress was found to have gender differences in subjects’ reports of food choices. In women, sweet foods emerged as important when compared with men. In laboratory and survey studies,16-18 restrained eaters consistently showed hyperphagia; sweets and chocolate, cake and biscuits, and savory snacks were reported to be eaten more under stress. Food choices leaned toward more high energy-dense, snack-type foods. Recent studies19,20 have identified shift work as a major source of stress. Several studies9,21,22 have shown that this affects the circadian distribution of food, regularity of meals, and the number of meals eaten during the different shifts. These studies9,19,22 have demonstrated a higher total energy intake among night nurses than day nurses and reduced consumption of dietary fibers, primarily due to a reduction in the consumption of green vegetables and in increase in sucrose resulting from higher intake of soft drinks, snacks, or limited food choices. This study examined the associations among stress, shift work, and eating behavior among non-Saudi female nurses in Riyadh, KSA.
Methods
From the pilot survey, we assumed the proportion of abnormal eating was 60% among nurses on shift duty and a desired 95% confidence interval of 5%. The study sample size was estimated at 369. The study was conducted in Riyadh, KSA, in 2 major hospitals: the King Fahad Medical City (KFMC), the largest governmental medical city in KSA, which provides free medical services to the whole population, and King Khalid University Hospital (KKUH), which is the largest teaching hospital in KSA. Fifteen records were eliminated due to missing values. The distribution of nurses in the 2 hospitals is approximately the same.
The survey was designed through an iterative process that included searching the recent literature and discussions with several experts in the areas of nutrition, nursing, health behaviors, and survey development. Based on a review of the literature and suggestions received from experts, we developed a pilot questionnaire. Since the official language spoken in the 2 hospitals is English, and non-Saudi workers typically speak English, the survey was developed in English. To minimize the time burden of respondents, we merged a number of scales or items to limit the number of survey items. Participants received a letter explaining the study and informing them that they could ask questions or refuse to participate. A pilot survey was distributed to 15 nurses who were not included in the sample; these nurses were asked to comment on the clarity, length, and content of the survey, and to report any technical problems they encountered. The survey was distributed from November 2013 to January 2014. Two reminders were sent to non-respondents.
All participants involved in the study were informed in the cover letter that completion of the survey would serve as consent to participate in the study. Permission to distribute the survey was obtained from KKUH and KFMC. The study was approved by the College of Medical Sciences Ethics Committee and the institutional review board at KFMC, Riyadh, KSA. The responses received from nurses were automatically populated in a secure data server using SurveyMonkey. Body max index (BMI) was calculated as weight (kg) divided by height (m) squared from self-reported data. The literature provides evidence of the reliability of self-reported height and weight values. Moreover, our sample of nurses possesses the education to take such measurements accurately.23-25 The BMI is categorized according to the World Health Organization cut-off points.26 Participants were classified into 4 categories: 1) underweight (BMI <18.5), 2) normal weight (BMI 18.5-24.9), 3) overweight (BMI 25-29.9), and 4) obese (BMI >30). The survey included some items related to work schedule (regular daytime/shift duty). Shift duty was defined as work performed outside of typical daytime hours, including rotating shifts and night shifts. Furthermore, participants were asked to record the frequency of their night shifts per month (0, 1-3 times, 4-7 times, more than 7 times).
Eating behavior refers to a complex interplay among physiological, psychological, social, and genetic factors that influence meal timing, quality of food intake, and food preference. The Dutch Eating Behavior Questionnaire (DEBQ)27 is a 33-item self-reported questionnaire. The DEBQ measures 3 unhealthy eating behaviors: restrained eating (10 items), which is the tendency to restrict food intake in order to control body weight; emotional eating (13 items), which is the tendency to cope with negative emotions (for example, anxiety or irritability); and external eating (10 items), which is the extent to which external cues of food trigger eating episodes (for example, the reinforcing value of the sight and smell of attractive food). All items were rated on a 5-point Likert-type scale with response categories that ranged from 1 (never) to 5 (very often). Furthermore, we classified eating styles to ‘yes’ if the scores were above the 75th percentile and to ‘no” if it is less or equal to 75th percentile. The scales have a high internal consistency (reliability between 0.80 and 0.95) and good construct and predictive validity.27 The Cronbach’s alpha in the current sample is 0.94 for emotional eating, 0.89 for external eating, and 95 for restrained eating.
Participants’ eating habits were assessed using items to elicit information on the frequency of eating fast food and snacks (never, sometimes, often, or almost every day). Furthermore, the number of servings of fruit and vegetables was assessed and the serving size was defined as a medium-sized portion of fruit, half a cup of vegetables, fruit or juice, or one cup of salad and potatoes. Binge eating was assessed by one question that asked how often during the past 12 months the nurse had engaged in episodes of binge eating, defined as “eating an unusually large amount of food in one go and at the time feeling that your eating was out of control.”28 The perceived stress scale (PSS) developed by Cohen et al29 containing 4 items was used. The PSS is the most widely used psychological instrument for measuring the perception of stress. It is a measure of the degree to which situations in one’s life are appraised as stressful. The scale also includes a number of direct queries on current levels of experienced stress. Moreover, the questions are of a general nature and hence are relatively free of content specific to any sub-population group. The questions in the scale were rated as: 0= never, 1= almost never, 2= sometimes, 3= fairly often, and 4= very often. Scores range from 0 to 16. Because there are no published cut-off points for high versus moderate or low stress for the PSS, we stratified the stress score into high stress if the scores were above the 75th percentile;30,31 specifically, we choose a PSS greater than 11 to define high stress and a PSS less than 6 to define low stress.
Data analysis was performed using the Statistical Package for the Social Sciences version 21 software (IBM Corp., Armonk, NY, USA). The Shapiro-Wilk test for normality revealed the following statistics: 0.716 for restrained, 0.827 for emotional, 0.791 for external, and 0.689 for stress (p<0.001). Since the assumption of normality was rejected, nurses in this study were categorized as having unhealthy eating behavior if their scores were ≥75th percentile.32 We used the Kruskal Wallis test to compare characteristics. Chi-square was used to assess the level of association between eating behaviors, BMI, stress, and shift work. Bivariate correlation analysis to test the correlation between eating styles, stress, and BMI, using the Spearman correlation coefficient. Multivariate analysis of covariance was carried out for the 3 eating styles with stress and shift work. For each food style, we adjusted for other food styles. Multiple logistic regression was used to determine factors associated with food styles after adjusting for confounders (age, gender, education, experience, and marital status).
Results
Table 1 shows information for eating styles in relation to socioeconomic and work variables of the respondents. Most of the nurses were married (69.6%) and under 40 years of age (68.6%). Most nurses reported finishing their bachelor degree (56.2%), with 23% having an undergraduate diploma and only 8.9% with higher education. Most of the nurses worked night shift duty (65.3%) more than 7 times per month (40.3%). In this sample, almost 50% were classified as having normal BMI and 50.6% were either overweight (37.7%) or obese (12.9%). The table further showed the association between food styles, socioeconomic, and work variables. Stress and education were significantly associated with all eating styles. Those with high stress and with undergraduate diplomas were more prone to restrained eating, emotional eating, and external eating than those with low stress and higher educational levels. The results further showed a significant association between marital status and shift work with restrained and external eating. Those who were married had a greater propensity toward restrained and external eating. Those working night shift duty were more likely to experience restrained eating, but less likely to experience external eating. Moreover, BMI and frequency of night shifts per month were associated with restrained eating. Overweight nurses and those working 4 to 7 night shifts per month were more inclined toward restrained eating compared with other groups.
Table 1.
Demographic characteristtics of 395 non-Saudi female nurses from 2 major hospitals in Riyadh, Saudi Arabia.
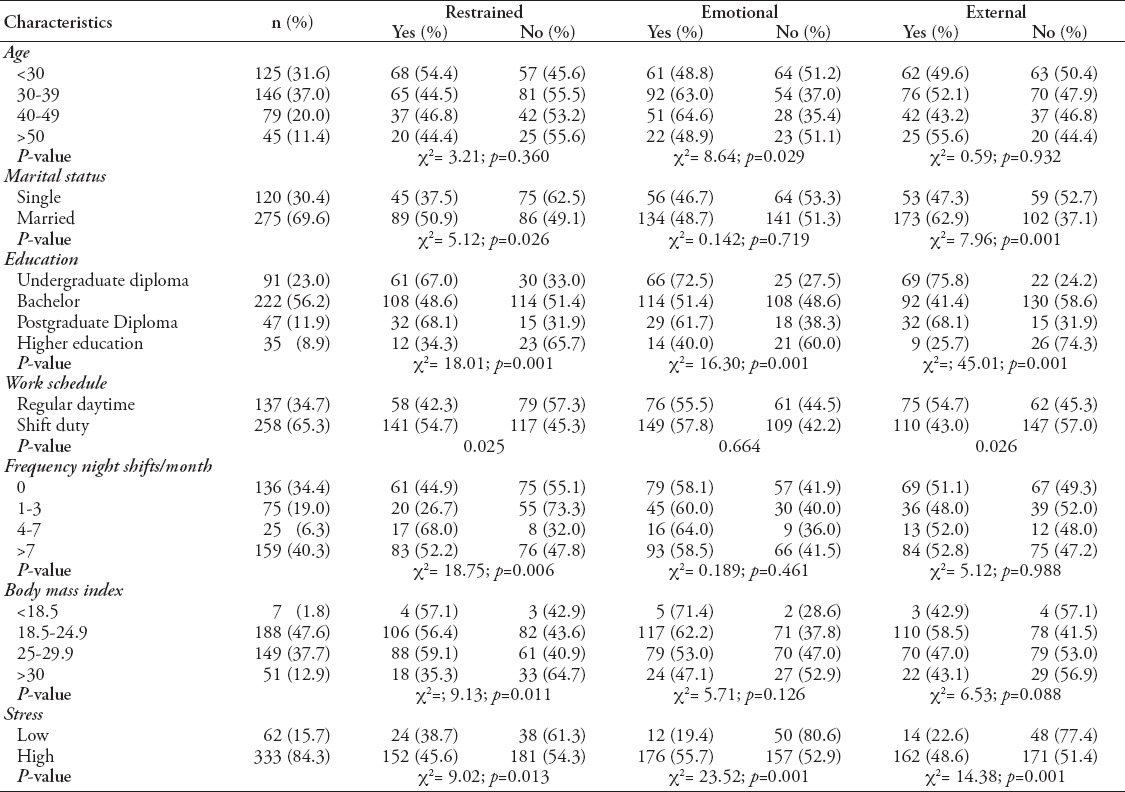
Table 2 presents the Spearman correlation coefficients between eating styles, stress, and BMI. Results indicated that stress had a significant and positive correlation with all eating styles. This suggests that nurses with high stress had more eating problems. The BMI was significant and positively correlated with restrained, emotional styles, and stress. Multivariate analysis of covariance (results not shown) showed a significant difference between the levels of stress and shift work for all eating styles. Interaction between levels of stress and levels of shift work were detected.
Table 2.
Spearman’s correlation coefficients between eating styles, stress, and body max index (BMI) in 395 non-Saudi female nurses from 2 major hospitals in Riyadh, Saudi Arabia.
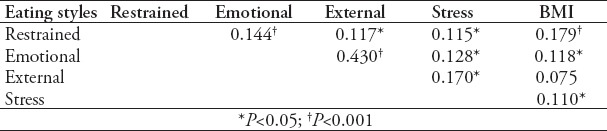
Table 3 displays the result of the Chi-square test χ2, which explore the association between levels of food styles with the levels of stress. For all eating styles, stress influenced the amount of food nurses consumed, but was more significant under restrained eating. Under the restrained eating style, a significantly higher percentage of nurses (often and almost every day) reported eating more fast food, snacks, and binging, while fruits and vegetables were the least likely to be eaten under stress (2 and fewer than 2 servings).
Table 3.
Eating styles (restrained, emotional, external) with stress (low, high) in 395 non-Saudi female nurses from 2 major hospitals in Riyadh, Saudi Arabia.
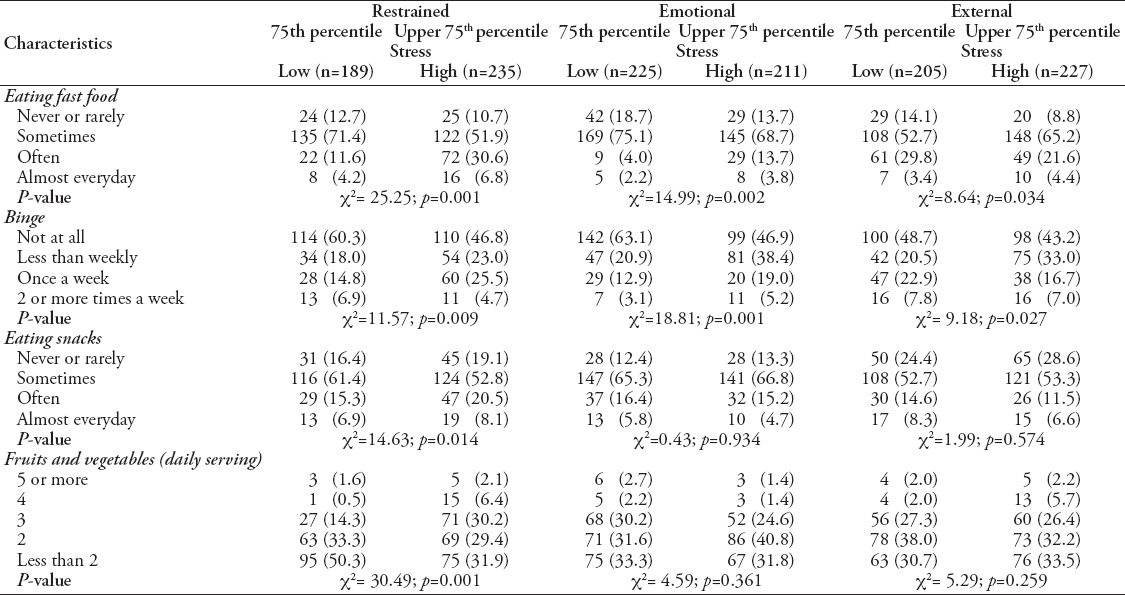
Table 4 presented the result of the chi-square test χ2, which demonstrated the association between levels of eating styles with levels of work schedule. Under restrained eating style, a significant higher percentage of shift duty nurses (often and almost everyday) reported eating more fast food, snacks, and binging, while fruits and vegetables were the least likely to be eaten during shift duty (2 and less than 2 servings).
Table 4.
Eating styles (restrained, emotional, external) with work schedule (daytime, shift duty) in 395 non-Saudi female nurses from 2 major hospitals in Riyadh, Saudi Arabia.
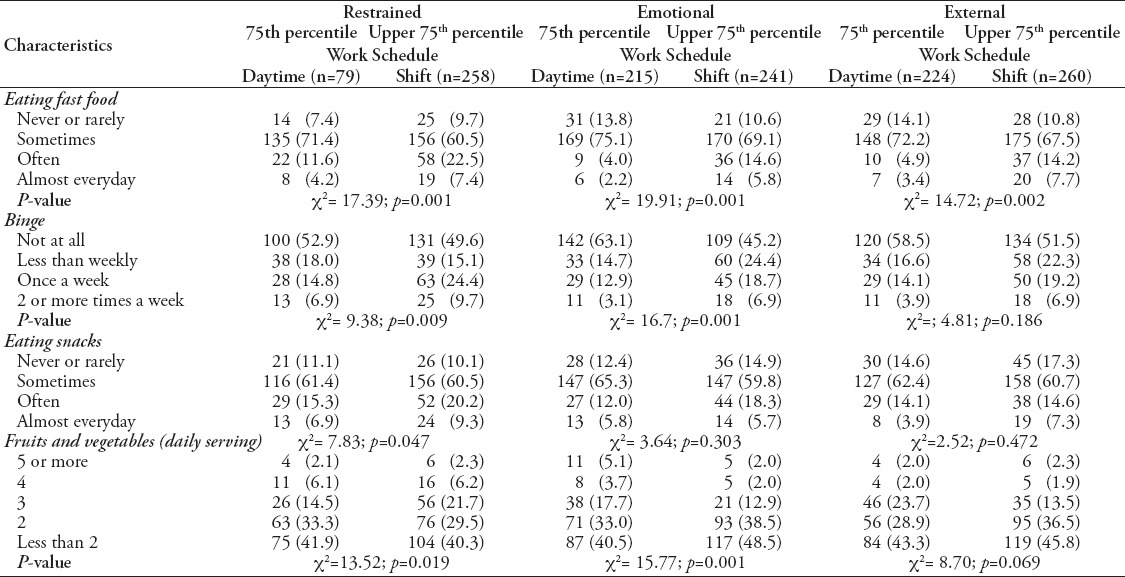
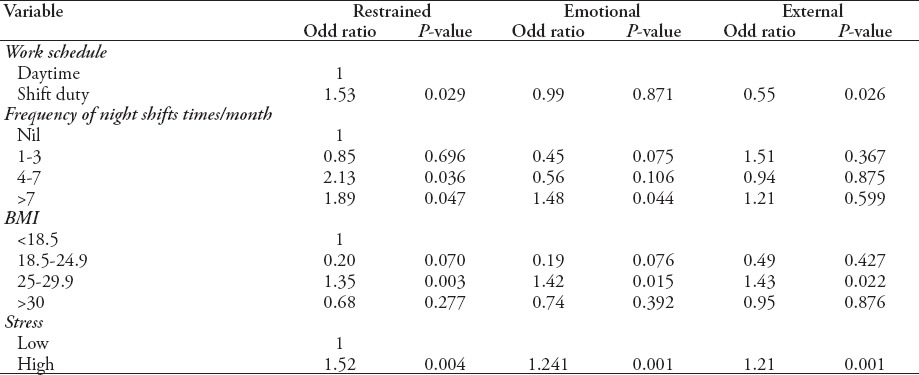
Table 5 reported the results of the multiple logistic regression for all eating styles after adjusting for all confounders. Nurses working night shift duty were 53% more likely to have abnormal restrained eating, and were less likely by approximately 45% to present abnormal external eating than those working the day shift. Nurses who were overweight were 35% more likely to have abnormal restrained, 42% emotional, and 43% external eating when compared with the underweight nurses. Those who worked 4-7 nights per month or more were significantly more likely to have abnormal eating scores in restrained style when compared with nil. Nurses who reported high stress had a 52% higher odds in abnormal restrained eating, a 24% higher odds in abnormal emotional eating, and 21% higher odds in external eating when compared with nurses with low stress.
Table 5.
Stepwise logistic regression of work schedule, body max index (BMI), and stress with eating frequency styles after adjusting for confounders.
Discussion
Several previous studies8,17,22 conducted across various occupations and cultures showed that the type of work undertaken appears unimportant in the association between stress and eating. Workers who experienced stress at work also tended to report unhealthy dietary patterns.8,17,22 In addition to the common stressors in the nursing practice, these nurses face additional stress from language and cultural differences. Our nurses were recruited from different countries, and cultural differences play a role in how job-related stress interacts with food intake. Studies carried out in other countries8,33 indicated that cultural differences were associated with psychosocial working conditions and eating habits. For example, in Finland8 eating behavior and working conditions were not related. In Britain,22 shift workers reported eating healthier food than those working day shift. Most nurses who reported abnormal eating when stress was restrained compared with emotional and external. This is in line with the results in other occupations that found restrained eating to be the best predictor of stress-induced eating.19,34-36 Research has shown that the type of food consumed in a stressful workplace tended to be high in sugar and fat.37,38 Although this study did not test for fat consumption specifically, fast food is often high in fats. Stress-restrained interaction has been reported in animal literature.11 The combination of caloric restrictions and stress increased the consumption of platable (high fat) food in female rats as compared with dietary restriction or stress alone.4,20,37 It could be speculated that fast food composition with its aesthetics (taste), could have more of an influence on why certain foods are chosen over others during stressful times. Our results are in keeping with the findings of those previously reported38 that suggested a significantly strong restraint-binge eating association in the presence of significant daily stress, such as job stress. Our results showed that under restrained eating those who binged once or more times a week were higher (30.2%) compared with emotional (24.2%) and external (23.7%) eating. Woods et al39 reported that the combined effect of job stress on binge eating behavior was only present in conditions of abnormal eating behavior, because those individuals are already at risk of binge eating. They concluded that the effects of these different forms of stress are multiplicative rather than additive when considered together.
Regarding the relationship among the 3 eating styles, the results agreed with previous research16 that showed significant correlations between the emotional and external eating styles, and small but significant correlations between restrained and emotional eating styles. The correlation among eating styles and BMI showed a positive association between both restrained and emotional eating, supporting previous studies.5,10,12 The typical response to job stress is not to avoid food, but to seek out and consume energy-dense food. However, the external style did not show a significant correlation with BMI, contrary to earlier studies.5,12
Our study demonstrated that shift duty was associated with abnormal restraint eating behavior. During shift duty including night shift, there were decreased frequencies of eating all type of food. Most of the nurses who work shift duty eat more fast food and snacks, and less vegetables. These results are similar to those reported by the study of Wang et al,19 which showed that nurses working night shifts preferred fast food and more snacks in order to keep them awake and maintain energy due to their heavy work load. Reeves et al40 reported that nurses working the night shift eat dinner too early before leaving for duty and eat very little food; they then try to compensate by snacking. Sahu and Dey41 found that the daily intake of carbohydrates, protein, and fats are significantly lower during the night shift than the day shift. and the amount of full meals, appetite, and eating satisfaction were significantly lower during the night shift. Factors, such as time availability and social context play an important role in determining food intake during the night shift.
Study limitations
This study was cross-sectional in design, and precluded the possibility of assessing cauasality. We did not include many food items that may be associated with eating styles, but despite the limited food items included, these items provided valuable information on food choices among nurses when they are under stress. Also, the self-report data raises concerns regarding accurate recall.
In conclusion, this study is conducted among non-Saudi female nurses in KSA, investigating the association between job stress and eating food behavior considering several variables as confounders. Our findings suggest that stress and shift duty were associated with changes in eating behavior. Those who reported stress ate more fast food and less fruits and vegetables. Hospitals can attempt to make appropriate provisions and provide facilities for the nurses at night. Healthy eating and canteen facilities may make it easier for night shift workers to cope and improve available dietary choices.
Acknowledgment
The author would like to extend his sincere appreciation to the Deanship of Scientific Research at King Saud University for funding this research through the Research Group Project. Author is indebted to the administration of the 2 hospitals for allowing him to carry out this study and to the nurses who took an active part. The author would like to thank Dr. Badreldin Mohamed for his assistance with the statistical analyses.
Footnotes
References
- 1.Abu-Zinadah S. Nursing situation in Saudi Arabia. Riyadh (KSA): Saudi Commission for Health Specialities; 2006. [Google Scholar]
- 2.Aldossary A, While A, Barriball L. Health care and nursing in Saudi Arabia. Int Nurs Rev. 2008;55:125–128. doi: 10.1111/j.1466-7657.2007.00596.x. [DOI] [PubMed] [Google Scholar]
- 3.Aboul-Enein FH. Personal contemporary observations of nursing care in Saudi Arabia. Int J Nurs Pract. 2002;8:228–230. doi: 10.1046/j.1440-172x.2002.00370.x. [DOI] [PubMed] [Google Scholar]
- 4.Oliver G, Wardle J. Perceived effects of stress on food choice. Physiol Behav. 1999;66:511–515. doi: 10.1016/s0031-9384(98)00322-9. [DOI] [PubMed] [Google Scholar]
- 5.Torres SJ, Nowson CA. Relationship between stress, eating behavior, and obesity. Nutrition. 2007;23:887–894. doi: 10.1016/j.nut.2007.08.008. [DOI] [PubMed] [Google Scholar]
- 6.Zellner DA, Loaiza S, Gonzalez Z, Pita J, Morales J, Pecora D, et al. Food selection changes under stress. Physiol Behav. 2006;87:789–793. doi: 10.1016/j.physbeh.2006.01.014. [DOI] [PubMed] [Google Scholar]
- 7.Kandiah J, Yake M, Jones J, Meyer M. Stress influences appetite and comfort food preferences in college women. Nutr Res. 2006;26:118–123. [Google Scholar]
- 8.Stewart-Knox BJ. Eating and stress at work: The need for public health promotion intervention and an opportunity for food product development? Trends in Food Science and Technology. 2014;35:52–60. [Google Scholar]
- 9.Zhao I, Bogossian F, Turner C. A cross-sectional analysis of the association between night-only or rotating shift work and overweight/obesity among female nurses and midwives. J Occup Environ Med. 2012;54:834–840. doi: 10.1097/JOM.0b013e31824e1058. [DOI] [PubMed] [Google Scholar]
- 10.Buss J. Associations between obesity and stress and shift work among nurses. Workplace Health Saf. 2012;60:453–458. doi: 10.1177/216507991206001007. [DOI] [PubMed] [Google Scholar]
- 11.Wardle J, Steptoe A, Oliver G, Lipsey Z. Stress, dietary restraint and food intake. J Psychosom Res. 2000;48:195–202. doi: 10.1016/s0022-3999(00)00076-3. [DOI] [PubMed] [Google Scholar]
- 12.Nguyen-Michel ST, Unger JB, Spruijt-Metz D. Dietary correlates of emotional eating in adolescence. Appetite. 2007;49:494–499. doi: 10.1016/j.appet.2007.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.van Strien T, Herman CP, Anschutz DJ, Engels RC, de Weerth C. Moderation of distress-induced eating by emotional eating scores. Appetite. 2012;58:277–284. doi: 10.1016/j.appet.2011.10.005. [DOI] [PubMed] [Google Scholar]
- 14.Cools J, Schotte DE, McNally RJ. Emotional arousal and overeating in restrained eaters. J Abnorm Psychol. 1992;101:348–351. doi: 10.1037//0021-843x.101.2.348. [DOI] [PubMed] [Google Scholar]
- 15.Wallis DJ, Hetherington MM. Emotions and eating. Self-reported and experimentally induced changes in food intake under stress. Appetite. 2009;52:355–362. doi: 10.1016/j.appet.2008.11.007. [DOI] [PubMed] [Google Scholar]
- 16.Goossens L, Braet C, Van Vlierberghe L, Mels S. Loss of control over eating in overweight youngsters: the role of anxiety, depression and emotional eating. Eur Eat Disord Rev. 2009;17:68–78. doi: 10.1002/erv.892. [DOI] [PubMed] [Google Scholar]
- 17.Weinstein SE, Shide DJ, Rolls BJ. Changes in food intake in response to stress in men and women: psychological factors. Appetite. 1997;28:7–18. doi: 10.1006/appe.1996.0056. [DOI] [PubMed] [Google Scholar]
- 18.McCann BS, Warnick GR, Knopp RH. Changes in plasma lipids and dietary intake accompanying shifts in perceived workload and stress. Psychosom Med. 1990;52:97–108. doi: 10.1097/00006842-199001000-00008. [DOI] [PubMed] [Google Scholar]
- 19.Wong H, Wong MC, Wong SY, Lee A. The association between shift duty and abnormal eating behavior among nurses working in a major hospital: a cross-sectional study. Int J Nurs Stud. 2010;47:1021–1027. doi: 10.1016/j.ijnurstu.2010.01.001. [DOI] [PubMed] [Google Scholar]
- 20.Laitinen J, Ek E, Sovio U. Stress-related eating and drinking behavior and body mass index and predictors of this behavior. Prev Med. 2002;34:29–39. doi: 10.1006/pmed.2001.0948. [DOI] [PubMed] [Google Scholar]
- 21.van Amelsvoort LG, Schouten EG, Kok FJ. Duration of shiftwork related to body mass index and waist to hip ratio. Int J Obes Relat Metab Disord. 1999;23:973–978. doi: 10.1038/sj.ijo.0801028. [DOI] [PubMed] [Google Scholar]
- 22.Lennernäs M, Hambraeus L, Akerstedt T. Shift related dietary intake in day and shift workers. Appetite. 1995;25:253–265. doi: 10.1006/appe.1995.0060. [DOI] [PubMed] [Google Scholar]
- 23.Connor Gorber S, Tremblay M, Moher D, Gorber B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: a systematic review. Obes Rev. 2007;8:307–326. doi: 10.1111/j.1467-789X.2007.00347.x. [DOI] [PubMed] [Google Scholar]
- 24.Dekkers JC, van Wier MF, Hendriksen IJ, Twisk JW, van Mechelen W. Accuracy of self-reported body weight, height and waist circumference in a Dutch overweight working population. BMC Med Res Methodol. 2008;8:69. doi: 10.1186/1471-2288-8-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pasalich M, Lee AH, Burke L, Jancey J, Howat P. Accuracy of self-reported anthropometric measures in older Australian adults. Australas J Ageing. 2014;33:E27–E32. doi: 10.1111/ajag.12035. [DOI] [PubMed] [Google Scholar]
- 26.World Health Organization. Obesity: preventing and managing the global epidemic. Geneva (CH): WHO; 2000. [PubMed] [Google Scholar]
- 27.van Strien T, Frijters JE, Bergers GP, Defares PB. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. International Journal of Eating Disorders. 1986;5:295–315. [Google Scholar]
- 28.Hay PJ, Mond J, Buttner P, Darby A. Eating disorder behaviors are increasing: findings from two sequential community surveys in South Australia. PLoS One. 2008;3:e1541. doi: 10.1371/journal.pone.0001541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–396. [PubMed] [Google Scholar]
- 30.El-Masry R, Ghreiz SM, Helal RM, Audeh AM, Shams T. Perceived stress and burnout among medical students during the clinical period of their education. Ibnosina Journal of Medicine and Biomedical Sciences. 2013;5:179–188. [Google Scholar]
- 31.Silveira ML, Pekow PS, Dole N, Markenson G, Chasan-Taber L. Correlates of high perceived stress among pregnant Hispanic women in western Massachusetts. Matern Child Health J. 2013;17:1138–1150. doi: 10.1007/s10995-012-1106-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hou F, Xu S, Zhao Y, Lu Q, Zhang S, Zu P, et al. Effects of emotional symptoms and life stress on eating behaviors among adolescents. Appetite. 2013;68:63–68. doi: 10.1016/j.appet.2013.04.010. [DOI] [PubMed] [Google Scholar]
- 33.Kiviniemi MT, Orom H, Giovino GA. Race/ethnicity, psychological distress, and fruit/vegetable consumption. The nature of the distress-behavior relation differs by race/ethnicity. Appetite. 2011;56:737–740. doi: 10.1016/j.appet.2011.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Polivy J, Herman CP. Distress and eating: why do dieters overeat? Int J Eat Disord. 1999;26:153–164. doi: 10.1002/(sici)1098-108x(199909)26:2<153::aid-eat4>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 35.Lennernäs MA, Hambraeus L, Akerstedt T. Nutrient intake in day workers and shift workers. Work and Stress. 1994;8:332–342. [Google Scholar]
- 36.Lowden A, Moreno C, Holmbäck U, Lennernäs M, Tucker P. Eating and shift work - effects on habits, metabolism and performance. Scand J Work Environ Health. 2010;36:150–162. doi: 10.5271/sjweh.2898. [DOI] [PubMed] [Google Scholar]
- 37.Marmonier C, Chapelot D, Louis-Sylvestre J. Effects of macronutrient content and energy density of snacks consumed in a satiety state on the onset of the next meal. Appetite. 2000;34:161–168. doi: 10.1006/appe.1999.0302. [DOI] [PubMed] [Google Scholar]
- 38.Nolan LJ, Geliebter A. Night eating is associated with emotional and external eating in college students. Eat Behav. 2012;13:202–206. doi: 10.1016/j.eatbeh.2012.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Woods AM, Racine SE, Klump KL. Examining the relationship between dietary restraint and binge eating: differential effects of major and minor stressors. Eat Behav. 2010;11:276–280. doi: 10.1016/j.eatbeh.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 40.Reeves SL, Newling-Ward E, Gissane C. The effect of shift-work on food intake and eating habits. Nutrition and Food Science. 2004;34:216–221. [Google Scholar]
- 41.Sahu S, Dey M. Changes in food intake pattern of nurses working in rapidly rotating shift. Al Ameen J Med Sci. 2011;4:14–22. [Google Scholar]