

INTRODUCTION
Severe burns present a significant clinical challenge and are resource intensive. Predicting mortality at admission for burn patients is useful in determining the likely outcomes of interventions and in stratifying levels of care. In addition, it can provide benchmarks for audit and research.
More than 45 composite models exist for the prediction of mortality in thermal injury, of which only a handful have been developed with methodological rigor.1 The 4 most routinely used are the Revised Baux score,2 the Belgian Outcome in Burn Injury score,3 Boston score,4 and Abbreviated Burn Severity Index (ABSI).5 Our aim was to validate and compare the utility of these scoring systems in an Irish population.
MATERIALS AND METHODS
All acute admissions to the national burns unit of the Republic of Ireland from 2010 to 2014 were included, and a database including relevant admission and outcome information was collated. Predicted mortality was calculated using the Belgian, Boston, ABSI, and Revised Baux scores, with a nomogram being used for the Revised Baux score.6 Predicted mortality was compared with observed mortality for each scoring system. Predictive accuracy was assessed using a receiver operating characteristics curve, and positive and negative predictive values were calculated.
RESULTS
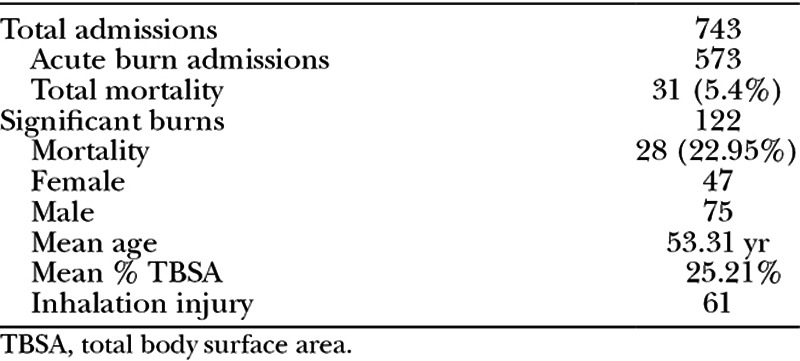
Demographic data can be seen in Table 1. Mortality was found to be 5.4% (31/573) over the study period. A total of 122 burns had a ≥10% total body surface area thermal injury. The mean age of this group was 53.31 years, with a mean total body surface area of 25.21% (range, 10–90%) and an inhalational injury rate of 50% (n = 61).
Table 1.
Demographic Data for Burn Injury Admissions in National Burns Unit of Ireland
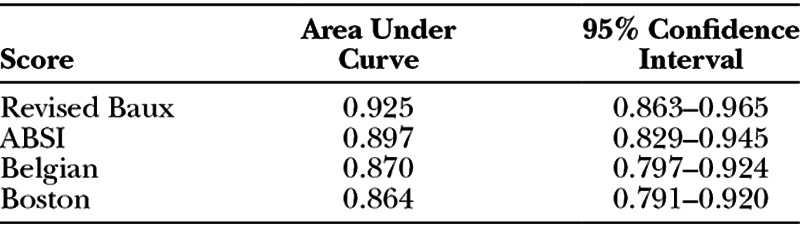
All 4 mortality prediction scores proved to be valid in our group (area under receiver operating characteristics curve > 0.80). The Revised Baux score performed the best, with an area under receiver operating characteristics curve of 0.925 (Fig. 1; Table 2). The observed deaths in our group were 28. The Belgian Outcome in Burn Injury score was the most accurate at predicting deaths in our group, with 27.33 deaths predicted. The Revised Baux score predicted 30.67 deaths.
Fig. 1.
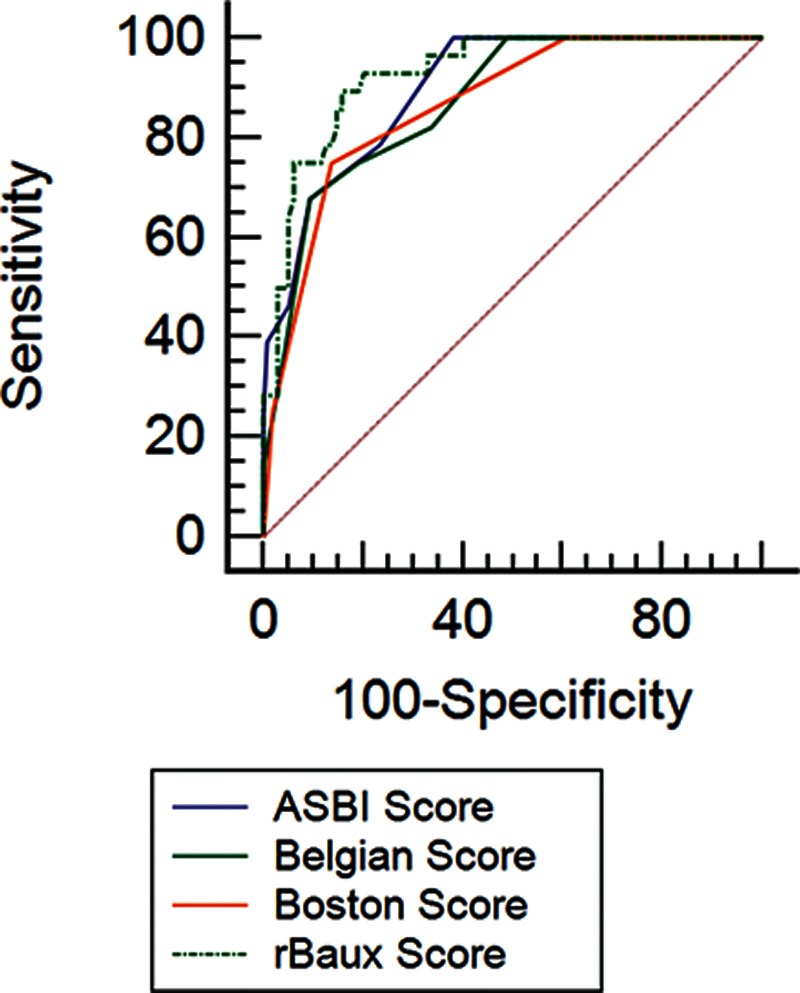
Receiver operating characteristics curves for mortality prediction scores. rBaux indicates revised Baux.
Table 2.
Area under the Receiver Operating Characteristics Curve for Mortality Prediction Scores
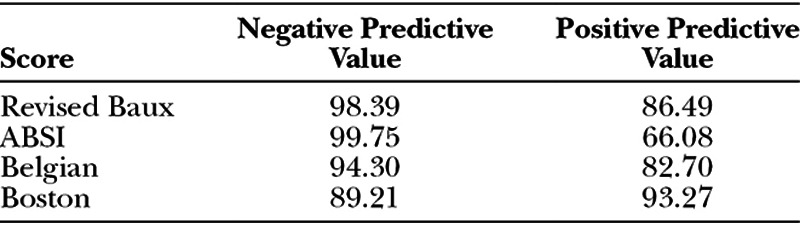
To be a useful model, the score must have both high negative and positive predictive values. The Revised Baux score and Belgian score performed best in this respect (Table 3). The ABSI had the highest negative predictive value of 99.75%; however, it had a low positive predictive value of 66.08%, significantly overpredicting the mortality rate, whereas the Boston score underpredicted mortality with the lowest negative predictive value of 89.21%.
Table 3.
Negative and Positive Predictive Values for Mortality Prediction Scores
DISCUSSION
Predicting mortality at admission in severe burns is a useful clinical adjunct. Several different scoring systems have been developed, and this indicates the complexity in calculating such a prediction. In reality, the use of only 1 or 2 of these tools should be necessary for clinical practice and research.
The 4 evaluated scoring systems in this study proved to be valid in an Irish population. The most accurate, reliable, and, therefore, useful predictors of mortality were considered to be the Revised Baux score and the Belgian Outcome in Burn Injury scoring system.
This compares favorably with other research, which has shown that the Belgian Outcome in Burn Injury score and the Revised Baux score seem to be particularly useful in predicting mortality in thermal injury.7,8
Footnotes
Presented at the Association for Research in Vision and Ophthalmology Annual Meeting, May 1–5, 2002, Fort Lauderdale, Fla. and at the Irish Association of Plastic Surgeons Meeting, May 14-15 2015, Galway, Ireland.
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the Irish Association of Plastic Surgeons.
IAPS: Irish Association of Plastic Surgeons (IAPS) Summer Meeting, in Galway, Ireland, May 14-15, 2015.
REFERENCES
- 1.Hussain A, Choukairi F, Dunn K. Predicting survival in thermal injury: a systematic review of methodology of composite prediction models. Burns. 2013;39:835–850. doi: 10.1016/j.burns.2012.12.010. [DOI] [PubMed] [Google Scholar]
- 2.Osler T, Glance LG, Hosmer DW. Simplified estimates of the probability of death after burn injuries: extending and updating the Baux score. J Trauma. 2010;68:690–697. doi: 10.1097/TA.0b013e3181c453b3. [DOI] [PubMed] [Google Scholar]
- 3.Belgian Outcome in Burn Injury Study Group. Development and validation of a model for prediction of mortality in patients with acute burn injury. Br J Surg. 2009;96:111–117. doi: 10.1002/bjs.6329. [DOI] [PubMed] [Google Scholar]
- 4.Ryan CM, Schoenfeld DA, Thorpe WP, et al. Objective estimates of the probability of death from burn injuries. N Engl J Med. 1998;338:362–366. doi: 10.1056/NEJM199802053380604. [DOI] [PubMed] [Google Scholar]
- 5.Tobiasen J, Hiebert JH, Edlich RF. Prediction of burn mortality. Surg Gynecol Obstet. 1982;154:711–714. [PubMed] [Google Scholar]
- 6.Williams DJ, Walker JD. A nomogram for calculation of the Revised Baux Score. Burns. 2015;41:85–90. doi: 10.1016/j.burns.2014.05.001. [DOI] [PubMed] [Google Scholar]
- 7.Douglas HE, Ratcliffe A, Sandhu R, et al. Comparison of mortality prediction models in burns ICU patients in Pinderfields Hospital over 3 years. Burns. 2015;41:49–52. doi: 10.1016/j.burns.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 8.Brusselaers N, Agbenorku P, Hoyte-Williams PE. Assessment of mortality prediction models in a Ghanaian burn population. Burns. 2013;39:997–1003. doi: 10.1016/j.burns.2012.10.023. [DOI] [PubMed] [Google Scholar]