

Abstract
Background
Minority children have the highest US uninsurance rates; Latino and African-American children account for 53 % of uninsured American children, despite comprising only 48 % of the total US child population. The study aim was to examine parental awareness of and the reasons for lacking health insurance in Medicaid/CHIP-eligible minority children, and the impact of the children’s uninsurance on health, access to care, unmet needs, and family financial burden.
Methods
For this cross-sectional study, a consecutive series of uninsured, Medicaid/CHIP-eligible Latino and African-American children was recruited at 97 urban Texas community sites, including supermarkets, health fairs, and schools. Measures/outcomes were assessed using validated instruments, and included sociodemographic characteristics, uninsurance duration, reasons for the child being uninsured, health status, special healthcare needs, access to medical and dental care, unmet needs, use of health services, quality of care, satisfaction with care, out-of-pocket costs of care, and financial burden.
Results
The mean time uninsured for the 267 participants was 14 months; 5 % had never been insured. The most common reason for insurance loss was expired and never reapplied (30 %), and for never being insured, high insurance costs. Only 49 % of parents were aware that their uninsured child was Medicaid/CHIP eligible. Thirty-eight percent of children had suboptimal health, and 2/3 had special healthcare needs, but 64 % have no primary-care provider; 83 % of parents worry about their child’s health more than others. Unmet healthcare needs include: healthcare, 73 %; mental healthcare, 70 %; mobility aids/devices, 67 %; dental, 61 %; specialty care, 57 %; and vision, 46 %. Due to the child’s health, 35 % of parents had financial problems, 23 % cut work hours, and 10 % ceased work. Higher proportions of Latinos lack primary-care providers, and higher proportions of African-Americans experience family financial burden.
Conclusions
Half of parents of uninsured minority children are unaware that their children are Medicaid/CHIP-eligible. These uninsured children have suboptimal health, impaired access to care, and major unmet needs. The child’s health causes considerable family financial burden, and one in 10 parents ceased work. The study findings indicate urgent needs for better parental education about Medicaid/CHIP, and for improved Medicaid/CHIP outreach and enrollment.
Keywords: Child, Adolescent, Medically uninsured, Public health, Hispanic Americans, African-Americans
Background
Although the number and proportion of US children without health insurance modestly declined between 2008-2012 [1], 6 % of US children (4.8 million) are uninsured [2], and 68 % (3.3 million) are eligible for but not enrolled in Medicaid or the Children’s Health Insurance Program (CHIP) [3]. Among uninsured US children, racial/ethnic disparities exist. In contrast to only 4.9 % of white children being uninsured, 9.6 % of Latino and 5.1 % of African-American children are uninsured [2]. Indeed, Latino and African-American children account for 53 % of uninsured American children [4], despite comprising only 48 % of the total population of US children [5].
Although 2.4 million Latino and African-American children are uninsured [4], not enough is known about the health and healthcare impact on these children of uninsurance, particularly from studies analyzing primary (rather than administrative/secondary) data. For the 1.6 million uninsured Latino and African-American children eligible for but not enrolled in Medicaid/CHIP, it is unknown what proportion of parents are aware of their children’s Medicaid/CHIP eligibility, and the reasons why these children remain uninsured. The study aims, therefore, were to identify the health and healthcare impact, parental awareness of uninsured children’s Medicaid/CHIP eligibility, and reasons why children lost or never had health insurance, among uninsured minority children eligible for but not enrolled in Medicaid/CHIP. Specifically, the objective was to use uniquely extensive primary data on a sample of uninsured minority children eligible for but not enrolled in Medicaid/CHIP to assess: parental sociodemographic features and health-insurance characteristics, and children’s sociodemographic features, health insurance, reasons for loss of health insurance and never having health insurance, health status, special healthcare needs (SHCNs), access to healthcare, unmet healthcare needs, use of health services, out-of-pocket healthcare costs, quality of care, quality of life, parental satisfaction with care, financial burden of children’s healthcare, and missed school and work due to the child’s health.
Methods
Study design and participants
In this cross-sectional study, a consecutive series of uninsured Latino and African-American children 0-18 years old residing in Dallas County who were eligible for but not enrolled in Medicaid/CHIP was recruited from June 2011 to January 2014 at 97 community sites in regions with the highest proportion of uninsured and low-income residents. To avoid distortion due to clustering, only one uninsured child per family was enrolled. To ensure participants were representative of families with uninsured children in these regions, recruitment occurred in a variety of community settings, including supermarkets, department stores, dollar stores, Goodwill stores, restaurants, public libraries, community centers, food banks, health fairs, Boys and Girls clubs, YMCAs, churches, schools, community outpatient clinics, day-care establishments, Laundromats, apartment complexes, housing projects, homeless shelters, and WIC centers. Participant eligibility criteria included: 1) children 0-18 years old currently lacking health insurance; 2) parental self-identification of the child as Latino/Hispanic, African-American/black, or both; and 3) the child is eligible for Medicaid or CHIP. Eligibility for Medicaid or CHIP initially was determined in the field by research staff using family income, assets, and other information required to determine eligibility by the State of Texas, and then officially confirmed through electronic verification by the Texas Health and Human Services Commission, which administers both Medicaid and CHIP for the state. Subjects subsequently participated in a randomized trial, called Kids’ HELP (Kids' Health Insurance by Educating Lots of Parents), of the effects of parent mentors on insuring uninsured minority children, full details of which are available elsewhere [6].
Dallas County, TX, is an ideal setting for studying uninsured minority children, because: 1) Texas has the highest proportion and number of uninsured of any state in America, at 19 % and five million, respectively; 2) Texas has the highest number of uninsured children (783,938); and 3) 15.9 % of children in Dallas County are uninsured, compared with 9 % in Texas and 6 % in the US [7–9].
All participants provided written consent and/or assent (when indicated). This study was approved by the University of Texas Southwestern Institutional Review Board.
Surveys
Primary caregivers (as identified by families) completed eligibility screening surveys (using Texas Medicaid/CHIP eligibility criteria [10]) and two questionnaires (in English or Spanish, according to parental preference) orally administered by trained bilingual research assistants, to overcome language and literacy barriers. The conceptual framework for the questionnaire domains and questions was a slightly modified version of the World Health Organization’s social-determinants-of-health framework [11]: specifically, survey items focused on social determinants of health, defined as the conditions in which people are born, grow, live, work, and age, and which are considered primarily responsible for health inequities. The first questionnaire consisted of 82 questions addressing parental and children’s characteristics; whenever possible, validated questions from longstanding national and state surveys and published articles were used [12–25]. Fourteen questions addressed parental sociodemographics and health insurance, and 68 examined children’s sociodemographics, health insurance, reasons for loss of health insurance and never having health insurance, health status, SHCNs, access to healthcare, unmet healthcare needs, use of health services, out-of-pocket healthcare costs, quality of care, parental satisfaction with care, financial burden of children’s healthcare, and missed school and work due to the child’s health. The Maternal and Child Health Bureau’s standard definition for SHCNs was used (those who have a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally) [26]. Children’s quality of life was assessed using the Pediatric Quality of Life Inventory Version 4.0 Generic Core Scales (PedsQL) [27]. Responses to open-ended questions were categorized by theme, and frequencies of response themes tallied. Complete details on definitions, outcomes, and survey instruments are available elsewhere [6].
Parental awareness of the uninsured child’s Medicaid/CHIP eligibility was assessed with the yes/no question, “Your child is eligible for Medicaid or CHIP. Did you know that?” For affirmative responses, parents also were asked the open-ended question, “Why have you chosen not to enroll your child in Medicaid or CHIP?” Although implementation of the Affordable Care Act (ACA) occurred in only the final month of the 32 months of data collection, parents were asked whether the ACA affected their awareness and knowledge of children’s Medicaid/CHIP, and none reported any ACA impact.
Analyses
SAS 9.3 was used for all analyses, with a two-tailed P < .05 considered statistically significant. To summarize parental and child characteristics, percentages were used for categorical data and means for continuous data. Bivariate analyses identified racial/ethnic differences and factors associated with parental awareness of Medicaid/CHIP eligibility. The non-parametric Wilcoxon test was used to evaluate continuous variables, and the Pearson Chi-square test for categorical outcomes. For the hierarchical multivariable logistic regression analysis of factors associated with parental unawareness of children’s Medicaid/CHIP eligibility, SAS Proc Logistic was used, with stepwise selection and an initial alpha-to-enter of 0.15 [28].
Results
Sample characteristics
We screened 49,361 caregivers; 49,094 candidates were excluded, due to failure to meet inclusion criteria, children already having Medicaid/CHIP or private insurance, and other reasons, yielding the final sample of 267 children (Fig. 1). The mean child age was seven years old, half were female, about 2/3 were Latino, 1/3 were African-American, and most were US-born (Table 1). Primary caregivers (hereafter referred to as parents) were predominantly female; 1/3 had limited English proficiency (LEP), the plurality were married and living with the spouse, >40 % were not high-school graduates, and > ½ were unemployed. About ¼ of parents had health insurance, primarily Medicaid. The mean annual family income was $21,857. There were means of two children and two adults in the households.
Fig. 1.
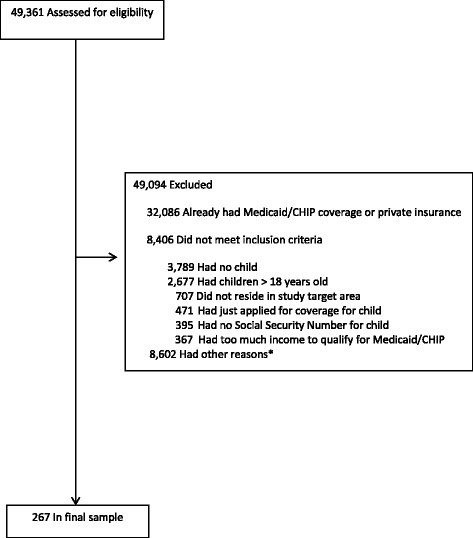
Participant accrual and reasons for exclusion of ineligible study candidates. *Including not interested in participating in study, took information without further follow-up, legal-custody issues, and grandparent did not know whether or not the child was insured
Table 1.
Selected characteristics of uninsured minority children and their parents (N = 267)
| Characteristic | Mean or % |
|---|---|
| Age of child (years), mean (range) | 7.3 (1, 18) |
| Gender of child | |
| Male | 50 % |
| Female | 50 % |
| Race/ethnicity of child | |
| Latino | 65 % |
| African-American | 35 % |
| Child born in US | 95 % |
| Gender of primary caregiver | |
| Female | 96 % |
| Male | 4 % |
| Primary caregiver has limited English proficiency | 32 % |
| Marital status of primary caregiver | |
| Married, living with spouse | 39 % |
| Single | 30 % |
| Married, separated from spouse | 13 % |
| Common-law marriage | 7 % |
| Divorced | 6 % |
| Living with partner | 4 % |
| Widowed | 1 % |
| Primary caregiver not high-school graduate | 43 % |
| Primary caregiver unemployed | 53 % |
| Primary caregiver has health insurance | 26 % |
| Type of insurance coverage for insured caregiver | |
| Public | 52 % |
| Private | 45 % |
| Other | 3 % |
| Mean combined annual family income (range) | $21,857 ($1,440, $64,000) |
| Mean number of children in household (range) | 2.3 (1, 13) |
| Mean number of adults in household (range) | 2.1 (1, 6) |
| Primary caregiver aware that child is eligible for Medicaid or CHIP | 49 % |
| Child ever had health insurance before | 95 % |
| Insurance that uninsured child had in past | |
| Medicaid | 72 % |
| CHIP | 14 % |
| Private | 13 % |
| Instituto Mexicano del Seguro Sociala | 1 % |
| Mean months without insurance (range) | 14.2 (1-144) |
| Median months without insurance (inner 95th percentile range) | 6 (1, 84) |
| Reason child lost insuranceb | |
| Insurance expired and never reapplied | 30 % |
| Was told making too much income/did not qualify | 13 % |
| Changed job | 13 % |
| Change of address | 11 % |
| Applied but never got reply or information | 9 % |
| Missing paperwork | 8 % |
| Does not know | 6 % |
| Father was supposed to cover child | 4 % |
| Too expensive | 2 % |
| Did not provide reason | 2 % |
| Child was determined to be disabled | 1 % |
| Sometimes paid premium late and was dropped | 1 % |
| Language barrier | 1 % |
| Insurance stopped when child was adopted | 1 % |
| Child not US citizen | 1 % |
| Told child aged out of health-insurance coverage | 1 % |
| Not legal guardian | 1 % |
aPublic health insurance in Mexico
bCited by parents of uninsured minority children (N = 257) who were eligible for but not enrolled in Medicaid or CHIP. Does not include 12 children who have never been insured during their lifetime. Proportions sum to > 100 % because parents could choose more than one reason
Less than ½ of parents were aware their uninsured child was Medicaid/CHIP eligible (Table 1). Ninety-five percent of children ever had insurance before, most commonly Medicaid (almost ¾ of children), followed by CHIP, private insurance, and Mexico’s public health insurance. The mean months without health insurance was 14, ranging from 1 month to 12 years, with a median of six months uninsured.
Reasons for insurance loss/never having insurance
Insurance coverage most commonly was lost due to insurance expiration without parents ever reapplying, in 1/3 of cases (Table 1). The next most common reasons were the family had too much income/did not qualify, changing jobs, change of address, and applied but never received a subsequent reply. The remaining 12 reasons were cited by <9 % of parents.
For the 5 % of children never insured during their lifetime, the most common reasons for the child never being covered included the high cost of insurance (1/4), and language barriers, moving to Texas, and hassles, each at 15 %. Other reasons included originally not a documented citizen, being told the child is ineligible due to parental employment, applied but never heard back, and no reason, each at 8 %. Thus, in contrast to children with previous insurance coverage, unique reasons for those never covered include a move to Texas, hassles, and being told parental employment makes children ineligible.
Factors associated with parental unawareness
Several factors were associated with parental unawareness of uninsured children’s Medicaid/CHIP eligibility (Table 2). The mean duration of uninsurance was longer for unaware vs. aware parents (17 vs. 12 months), and the mean family income was higher by almost $4,000. Latino parents (57 %) were more likely to be unaware than African-American parents (40 %). Racial/ethnic differences in awareness, however, disappeared after adjustment for uninsurance duration and income (Table 3).
Table 2.
Bivariate analysis of factors associated with parental unawareness of their uninsured child’s eligibility for Medicaid or CHIP
| Characteristic | Unaware of child’s medicaid/CHIP eligibilitya | Aware of child’s medicaid/CHIP eligibility | P |
|---|---|---|---|
| Mean time uninsured, months | 16.8 | 11.8 | .01 |
| Mean annual combined family | |||
| income | $23,777 | $19,871 | .01 |
| Race/ethnicity | .04 | ||
| Latino | 57.1 % | 42.9 % | |
| African-American | 40.4 % | 59.6 % | |
aNo other factors were significantly associated with unawareness of child’s insurance eligibility
Table 3.
Multivariable hierarchical logistic regression analysis of factors associated with parental unawareness of their uninsured child’s eligibility for Medicaid or CHIPa
| Odds Ratio (95 % CI) of Parental Unawareness of Uninsured Child’s Eligibility for Medicaid/CHIP | |||
|---|---|---|---|
| Characteristic | Model 1 | Model 2 | Model 3 |
| Latino race/ethnicityb | 2.0 (1.2, 3.3) | 1.7 (0.99, 2.9) | 1.6 (0.9, 2.8) |
| Mean annual combined family income | — | 1.0 (0.99, 1.0) | 1.0 (0.99, 1.0) |
| Mean months uninsured | — | — | 0.98 (0.98, 1.0) |
aAll sociodemographic characteristics were eligible for model entry, but those listed are the only factors in the final model. Bold denotes a statistically significant odds ratio.
bReferent: African-American/black race/ethnicity
Health status and SHCNs
Over one-third of children had not excellent/very good health status (Table 4). More than four in five parents reported worrying about their child’s health more than other people, and ¾ expressed worry/concern about the child’s health. About 2/3 of children have SHCNs, consisting of 17 conditions, including particularly high rates (≥12 %) of eczema, respiratory allergies, asthma, behavior problems, and bone/joint conditions. In addition to these five conditions, noteworthy among the remaining 12 conditions include a 5-7 % prevalence of attention-deficit-hyperactivity disorder (ADHD), speech problems, depression, and anxiety; a 1-2 % prevalence of hearing problems, autism, and brain injury; and > ¼ with other health problems.
Table 4.
Health status, special healthcare needs, access to healthcare, unmet healthcare needs,a use of health services, parental out-of-pocket costs of health services, quality of pediatric care, parental satisfaction with pediatric care, parental-reported financial burden of child’s healthcare, and missed school and work days due to child’s health among uninsured minority children eligible for but not insured by Medicaid or CHIP (N = 267)
| Measure | Proportion, Mean, or Mean Cost |
|---|---|
| Health status | |
| Health status not excellent/very good | 38 % |
| Worry about child’s health more than other people | 83 % |
| Have emotional worry or concern about child’s physical health | 75 % |
| Special healthcare need | |
| Any special healthcare need | 66 % |
| Eczema | 28 % |
| Respiratory allergy | 18 % |
| Asthma | 15 % |
| Behavior problem | 13 % |
| Bone or joint problem | 12 % |
| More than three ear infections | 7 % |
| Allergy | 7 % |
| ADHD | 7 % |
| Speech problem | 7 % |
| Depression | 6 % |
| Headache | 6 % |
| Anxiety | 5 % |
| Hearing problem | 2 % |
| Autism | 1 % |
| Brain injury | 1 % |
| Diabetes | 0.4 % |
| Any other health problem | 27 % |
| Access to healthcare | |
| Child has no PCP | 64 % |
| Child has no usual source of preventive care | 40 % |
| Sources of preventive care and sick care different | 55 % |
| Never/sometimes gets immediate care from PCP | 10 % |
| Usual source of care has no night or weekend office hours | 88 % |
| Does not have access to 24-hour telephone coverage for sick care | 88 % |
| No access to same-day sick-care visit without appointment | 67 % |
| Child has no usual source of sick care | 18 % |
| Difficult getting appointment for sick care | 12 % |
| Never/sometimes has access to interpreterb | 11 % |
| Has problems getting care from specialists | 8 % |
| Has problem getting special servicesc | 8 % |
| Never/sometimes can obtain after-hours telephone help or advice | 6 % |
| Unmet healthcare needs | |
| Delayed or didn’t get needed healthcare | 73 % |
| Didn’t receive all needed dental care | 61 % |
| Didn’t receive all needed preventive care | 51 % |
| Didn’t receive all needed hearing aids or hearing care | 100 % |
| Didn’t receive all needed physical, occupational, or speech therapy | 79 % |
| Didn’t receive all needed mental healthcare | 70 % |
| Didn’t receive all needed mobility aids or devicesd | 67 % |
| Didn’t receive all needed specialty care | 57 % |
| Problems obtaining needed specialty referral | 53 % |
| Didn’t receive all needed home healthcare | 50 % |
| Didn’t receive all needed vision care | 46 % |
| Didn’t receive all needed medical supplies or equipmente | 23 % |
| Didn’t receive all needed acute care | 19 % |
| Didn’t receive all needed prescription medications | 18 % |
| Use and out-of-pocket cost of health services | |
| Mean number of any doctor visits in past year | 3.3 |
| Mean out-of-pocket cost per doctor visitf | $141.7 |
| Mean number of preventive care visits in past year | 1.0 |
| Mean out-of-pocket cost per preventive-care visitg | $46.7 |
| Mean number of sick visits in past year | 1.8 |
| Mean out-of-pocket cost per sick visith | $195.1 |
| Mean number of ED visits in past year | 0.9 |
| Mean out-of-pocket cost per ED visiti | $421.0 |
| Mean number of hospital stays in past year | 0.1 |
| Mean out-of-pocket cost per hospital stayj | $593.1 |
| Parental-reported financial burden of child’s healthcare | |
| Need additional income to cover child’s medical expenses | 45 % |
| Child’s health caused financial problems for family | 35 % |
| Family cut down on work hours to obtain healthcare for child | 23 % |
| Stopped working because of child’s health | 10 % |
| Missed school and work days due to child’s health | |
| Mean missed school days due to child’s illness | 3.4 |
| Mean missed work days due to child’s illness | 1.7 |
| Mean wage loss due to missed work days for child’s illnessk | $342.9 |
| Other mean costs related to taking care of sick childk | $155.5 |
| Quality of carel | |
| Mean rating of child’s well-child visits | 8.3 |
| Mean rating of quality of child’s primary-care provider | 8.9 |
| Mean rating of quality of child’s acute care | 8.6 |
| Mean rating of quality of child’s specialty provider | 8.3 |
| Parental satisfaction with child’s pediatric care | |
| Doctor never/sometimes asks how you are feeling as parent | 40 % |
| Doctor never/sometimes understands how your prefer to raise child | 27 % |
| Doctor never/sometimes take time to understand child’s specific needs | 21 % |
| Doctor never/sometimes respect you are expert on your child | 16 % |
| Did not ask all questions I wanted to ask doctor | 15 % |
| Doctor didn’t spend enough time with child | 14 % |
| Would not recommend child’s healthcare provider to friends | 24 % |
| Quality of life (mean PedsQL score) | |
| Total | 91 |
| Physical functioning | 93 |
| Social functioning | 92 |
| Emotional functioning | 86 |
| School functioning | 85 |
aThe denominator for each unmet healthcare need consists of only those parents responding that their child needed the particular category of care or service
bOnly among parents who had limited English proficiency
cIncludes physical therapy, medical equipment (such as wheelchairs), special-education services, or counseling
dIncludes canes, crutches, wheelchairs, or scooters
eSuch as G-tubes and nebulizer machines
fAmong children who made any doctor visit
gAmong children who made any preventive visit
hAmong children who made any sick visit
iAmong children who made any ED visit
jAmong children who were hospitalized
kAmong parents who missed any work due child’s illness
lOn scale of 0-10, where 0 = worst and 10 = best
Access and unmet needs
Substantial access barriers to healthcare and unmet needs were identified (Table 4). Approximately 2/3 of children have no primary-care provider (PCP), 40 % have no usual preventive-care source, >½ have different sources of preventive and sick care, and one in 10 never/sometimes gets immediate care from the PCP. About nine in 10 have a usual source of care that has no night or weekend hours and have no access to 24-h phone coverage for sick care, 2/3 have no access to same-day sick-care visits without appointments, one in five has no usual sick-care source, one in eight has difficulty obtaining sick-care appointments, and 11 % of LEP parents never/sometimes have access to medical interpreters. One in 12 children needing specialty care experienced problems obtaining specialty care, 8 % of those needing special services encountered problems obtaining those services, and 6 % of parents are never/sometimes able to obtain after-hours telephone help/advice.
Almost ¾ of parents delayed/didn’t get needed healthcare for their children (Table 4). Almost two-thirds of children had unmet dental-care needs, and > ½ had unmet preventive-care needs. All children with auditory deficits had unmet needs for hearing aids/hearing care. Among children with specific needs, >2/3 had unmet needs for physical/occupational/speech therapy; mental healthcare; and mobility aids/devices. Almost 60 % of children had unmet specialty-care needs, and > ½ had problems obtaining specialty referrals. Approximately half of children had unmet needs for home healthcare and vision care. About ¼ of children needing medical supplies/equipment did not receive them, and one in five children had unmet needs for acute care and prescription medications.
Use of services, financial burden, and missed school and work
Children averaged three physician visits, one preventive visit, two sick visits, one ED visit, and 0.1 hospital stays annually (Table 4). Mean out-of-pocket costs ranged from $47/preventive visit to $593/hospitalization.
Almost ½ of parents reported needing additional income to cover children’s medical expenses, and >1/3 that the child’s health caused family financial problems (Table 4). Approximately ¼ of parents reported the family cut work hours to obtain healthcare for children, and one in 10 stopped working because of their child’s health.
Children missed a mean of three school days, and parents a mean of two work days annually due to children’s illnesses (Table 4). The mean wage loss was $343/missed work day, and families also incurred mean additional costs of $156 in the past year due to children’s illnesses.
Quality of care, satisfaction with care, and quality of life
Mean quality-of-care ratings ranged from 8-9 (Table 4). Forty percent of parents reported children’s doctor never/sometimes asks how they are feeling as parents, and > ¼ that doctors never/sometimes understand how they prefer to raise their child (Table 4). Between 14-21 % of parents reported the doctor never/sometimes understands children’s specific needs or respects the parent as the expert on the child, the doctor didn’t spend enough time with the child, and the parent did not ask doctors all questions he/she wanted. Almost ¼ of parents would not recommend their child’s healthcare provider to friends. The overall mean PedsQL score was 91 (Table 4).
Racial/ethnic differences
A higher proportion of Latinos report worrying about their child’s health more than others, at almost 90 % vs. 3/4 of African-Americans (Table 5). Almost ¾ of Latino children have no PCP, vs. about ½ of African-American children, and Latino children are more likely to have no usual preventive-care source, and different sources of preventive and acute care. Almost all Latino children have usual sources of care without night or weekend hours and lacking 24-h phone coverage for sick care, vs. approximately ¾ of African-American children for both. Mean out-of-pocket costs per doctor visit and per sick visit and the number of yearly sick visits also were greater for Latino children.
Table 5.
Racial/ethnic differences in health status, special healthcare needs, access to healthcare, unmet healthcare needs, use of health services, parental out-of-pocket costs of health services, parental satisfaction with pediatric care, and parental-reported financial burden of child’s healthcare among uninsured minority children eligible for but not insured by Medicaid or CHIP (N = 267)a
| Measure | Latinos (N = 174) | African-Americans (N = 93) | P |
|---|---|---|---|
| Health status | |||
| Worry about child’s health more than other people | 89 % | 73 % | <.01 |
| Special healthcare need | |||
| Asthma | 10 % | 25 % | <.01 |
| ADHD | 4 % | 12 % | .02 |
| Access to healthcare | |||
| Has no PCP | 70 % | 52 % | <.01 |
| No usual source of preventive care | 51 % | 23 % | <.01 |
| Source of sick care and preventive care different | 60 % | 45 % | .02 |
| Usual source of care has no night or weekend office hours | 93 % | 79 % | <.01 |
| Doesn’t have 24-hour phone coverage for sick care | 95 % | 75 % | <.01 |
| No access to same-day sick-care visit without appointment | 27 % | 43 % | .01 |
| Never/sometimes receive help or advice over phone | 3 % | 11 % | .01 |
| Unmet healthcare needs | |||
| Didn’t receive all needed acute care | 5 % | 18 % | .01 |
| Didn’t receive all needed prescription medications | 7 % | 15 % | .03 |
| Use and out-of-pocket costs of health services | |||
| Mean out-of-pocket cost per doctor visitb | $153.2 | $119.5 | <.01 |
| Mean out-of-pocket cost per preventive-care visitc | $50.0 | $40.4 | .03 |
| Mean out-of-pocket cost per sick visitd | 210.3 | 160.5 | .01 |
| Mean number of sick visits in past year | 1.8 | 1.7 | .04 |
| Mean number of ED visits in past year | 0.5 | 1.5 | .03 |
| Parental satisfaction with care | |||
| Doctor never/sometimes understands how I prefer to raise my child | 21 % | 37 % | .01 |
| Parental-reported financial burden | |||
| Need additional income to cover child’s medical expenses | 39 % | 55 % | .02 |
aThere were no significant racial/ethnic differences for any measure not listed in the table
bAmong children who made any doctor visit
cAmong children who made any preventive-care visit
dAmong children who made any sick visit
African-American children are more likely than Latino children to have asthma and ADHD, no access to same-day sick care without appointments, to never/sometimes receive phone help/advice, and to make ED visits. African-American parents more often reported their child’s doctor never/sometimes understands how parents prefer to raise children, and > ½ need additional income to cover children’s medical expenses, vs. <40 % of Latino parents.
Discussion
Over half of parents are unaware that their uninsured minority children are Medicaid/CHIP eligible. These new quantitative results complement prior qualitative work documenting that lack of Medicaid/CHIP awareness is a major reason why parents have not insured uninsured minority children [29, 30]. These qualitative studies shed light on the reasons for parental unawareness of uninsured children’s Medicaid/CHIP eligibility, including parents lacking basic knowledge about Medicaid/CHIP, their eligibility rules, and the application process; language and immigration issues; income verification obstacles; misinformation from insurance representatives; system impediments; and family mobility. The current study findings indicate lack of Medicaid/CHIP awareness remains a substantial barrier for the 3.3 million uninsured US children eligible for but not enrolled in Medicaid/CHIP, and suggest that enhancing awareness and outreach will be crucial to insuring more uninsured children. The data indicate that special efforts should be made to target populations at highest risk of parental unawareness of children’s Medicaid/CHIP eligibility, including those uninsured the longest, those at the higher end of income eligibility, and Latinos.
The results reveal that broad system issues also impede parents from insuring Medicaid/CHIP-eligible children. One in seven children lost insurance because Medicaid/CHIP representatives incorrectly told parents that their children did not qualify for these programs or parental income was excessive, although all children were Medicaid/CHIP eligible. Insurance representatives also incorrectly told some families that children had “aged out” of coverage. Remedying these serious system barriers to insuring uninsured children may require better training of insurance representatives and careful monitoring and reporting of such system glitches. In addition, 9 % of parents reported they had applied for Medicaid/CHIP for their children, but never received a reply, suggesting substantial room for system improvement in application tracking and responses.
Ninety-five percent of uninsured children previously had insurance, underscoring Medicaid/CHIP retention will continue to be especially important in eliminating childhood uninsurance. About ¾ of children previously had Medicaid coverage, indicating Medicaid loss is a considerable challenge, and perhaps reflecting Texas (at the time of this study) was one of two states still requiring Medicaid renewal every six months, and one of 27 states not providing 12-month continuous Medicaid eligibility (i.e., regardless of family-income fluctuations) [31]. Parents reported a panoply of reasons for children losing coverage, most commonly not reapplying after insurance expiration and not knowing why coverage was lost, suggesting better parental education is needed. It is concerning that system problems accounted for ¼ of children losing coverage. Although all children were Medicaid/CHIP eligible, 13 % incorrectly were told they were ineligible, and 9 % applied with no response from the Medicaid/CHIP program. Parents changing jobs and family moves comprised ¼ of the reasons why children lost insurance; such challenging impediments may require tailored interventions known to be effective in insuring uninsured minority children, such as community health workers [32] and parent mentors [33].
Both the duration without coverage and proportion of children never insured are troubling. Multiple studies document uninsured children are significantly more likely than insured children to have suboptimal health, no regular physician, delayed immunizations, unmet needs, impaired specialty access [34] and higher odds of ED visits [35], avoidable hospitalizations [36], injury hospitalizations [37], adverse newborn outcomes [38], and death in hospitals, ICUs, and after trauma [39, 40]. Our study population averaged 14 months without insurance, with some uninsured up to 12 years, placing many at high risk for these deleterious consequences, with the one in 20 children never insured during their lifetime at especially high risk. Parental reasons for children never having insurance seem amenable to interventions, including language barriers, hassles, better understanding of eligibility criteria, more responsive Medicaid/CHIP systems, and reducing premiums and copays.
The study findings indicate that uninsurance takes a major toll on children’s health, and that many have SHCNs. Approximately 40 % of children have suboptimal health, 2/3 have SHCNs, and four in five parents worry about their child’s health more than others. These findings suggest that insuring these uninsured children has the potential to improve children’s health while reducing parental worry.
Substantial access barriers and unmet needs were noted. Although RCTs are needed, evidence from observational studies indicates insuring uninsured children improves access, reduces unmet needs, and increases preventive and acute visits [14–16, 18, 41–43]. This is the first study, however, to our knowledge, to use primary data from in-depth surveys to identify considerable unmet needs for uninsured children with SHCNs, including unmet needs for 100 % of children requiring hearing aids/hearing care, and most children needing physical/occupational/speech therapy, mental healthcare, mobility aids, and home healthcare.
Identified racial/ethnic differences have implications for providing care for uninsured children. The findings suggest that for clinicians and health systems caring for uninsured Latino children, it may prove particularly useful to reduce parental worry about children’s health and out-of-pocket costs, and ensure that children have PCPs, regular sources of preventive care, and 24-h phone sick-care coverage. For clinicians and health systems caring for uninsured African-American children, it may prove particularly useful to focus on higher rates of asthma and ADHD, access to same-day sick visits without appointments, unmet acute-care and prescription needs, phone help/advice, reducing ED visits, improving providers’ understanding of parental preferences for raising children, and additional income needs for children’s medical expenses.
Certain study limitations should be noted. The research was conducted in urban settings in Texas, so the results may not necessarily generalize to non-urban settings or other states. Only Latinos and African-American children participated, so the findings may not generalize to uninsured children in other racial/ethnic groups. Outcomes were not assessed for insured or white children in the same communities, so comparisons between insured and uninsured children and whites and minorities could not be performed. Due to the length of the three surveys on insurance and healthcare, we were unable to ask questions regarding other public services accessed, such as WIC or public housing. The final sample size of 267 was relatively small, but is the largest community-based sample (to our knowledge) of uninsured children to be assessed for such a wide spectrum of outcomes.
Sizeable family financial burdens and costs of care were identified. Substantial proportions of parents reported needing additional income for children’s medical expenses, children’s illnesses causing family financial problems, and families reducing work hours to obtain children’s healthcare, and one in 10 parents ceased work because of the child’s health. This is particularly concerning, given that all of these children are in poor or low-income families with very limited financial means and reserves. This is further compounded by major out-of-pocket expenses for pediatric care, including a mean of $142/doctor visit, $47/preventive-care visit, $195/sick visit, $421/ED visit, and $593/hospitalization. Factoring in additional economic losses incurred by caring for sick children, including a mean wage loss of $343/day and child-care expenses of $156/day, it is clear that uninsured children are costly for parents, families, businesses, and local economies.
Conclusions
Half of parents of uninsured minority children are unaware that their children are Medicaid/CHIP-eligible. These uninsured children have suboptimal health, impaired access to care, and major unmet needs for healthcare, mental healthcare, mobility aids/devices, dental care, specialty care, and vision care. The child’s health causes considerable family financial burden, and one in 10 parents ceased work because of their children’s poor health. These study finding indicate urgent needs for better parental education about Medicaid/CHIP and for improved Medicaid/CHIP outreach and enrollment. The data also indicate that special efforts should be made to target populations at highest risk of parental unawareness of children’s Medicaid/CHIP eligibility, including those uninsured the longest, those at the higher end of income eligibility, and Latinos.
For clinicians and health systems, the study results revealed racial/ethnic group-specific barriers which would seem to be crucial to target in efforts to improve the health and healthcare of uninsured minority children. For uninsured Latino children, these critical identified barriers include parental worry about children’s health and out-of-pocket costs, and children lacking PCPs, regular sources of preventive care, and 24-hour phone sick-care coverage. For uninsured African-American children, key identified barriers include higher rates of asthma and ADHD, lack of access to same-day sick visits without appointments, unmet acute-care and prescription needs, inadequate access to phone help/advice, high ED visit rates, limited healthcare provider understanding of parental preferences for raising children, and additional income needs for children’s medical expenses.
Acknowledgments
We are very grateful to all of the survey participants for their enthusiasm and dedication to improving the health and healthcare of uninsured children.
Funding source
Supported by Award Number R01HD066219 (to Dr. Flores) from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD). The content is solely the responsibility of the authors, and does not necessarily represent the official views of NICHD or National Institutes of Health.
Prior presentations
Presented in part as a platform presentation at the annual meeting of the Pediatric Academic Societies in Vancouver, BC, on May 4, 2014, and as a poster at the annual research meeting of AcademyHealth in San Diego, CA, on June 8, 2014.
Abbreviations
- ADHD
attention-deficit hyperactivity disorder
- CHIP
Children’s Health Insurance Program
- ED
emergency department
- LEP
limited English proficiency
- PCP
primary-care provider
- PedsQL
Pediatric Quality of Life Inventory Version 4.0 Generic Core Scales
- RCT
randomized, controlled trial
- SHCN
special healthcare need
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
GF conceptualized and designed the study, conducted data management, supervised data collection and management, supervised the study, drafted the initial manuscript, and reviewed and revised the manuscript. HL assisted with data collection and management, conducted statistical analyses, and reviewed and revised the manuscript. CW coordinated the study, assisted with data management, supervised data collection, and reviewed and revised the manuscript. ML assisted with data collection and reviewed and revised the manuscript. AP assisted with data management, collected data, and reviewed and revised the manuscript. MH assisted with data management, collected data, and reviewed and revised the manuscript. MF assisted with study coordination, assisted with data management, collected data, and reviewed and revised the manuscript. KM assisted with data management, collected data, and reviewed and revised the manuscript. All authors read and approved the final manuscript.
Contributor Information
Glenn Flores, Phone: (952) 992-3367, Email: glenn.flores@medica.com.
Hua Lin, Email: Hua.Lin@UTSouthwestern.edu.
Candy Walker, Email: Candice.Walker@tsrh.org.
Michael Lee, Email: MICHAEL.LEE@childrens.com.
Alberto Portillo, Email: alberto.portillo@sbcglobal.net.
Monica Henry, Email: monicaphenry@gmail.com.
Marco Fierro, Email: Marco.Fierro@UTSouthwestern.edu.
Kenneth Massey, Email: kfmassey@gmail.com.
References
- 1.State Health Access Data Assistance Center . For Kids’ Sake: State-Level Trends in Children’s Health Insurance. A State-by-State Analysis. Princeton: Robert Wood Johnson Foundation; 2014. [Google Scholar]
- 2.Smith JC, Medalia C, US Census Bureau . Health insurance coverage in the United States: 2014. Washington, DC: U.S. Government Printing Office; 2014. [Google Scholar]
- 3.Kenney GM, Haley JM, Anderson N, Lynch V. Children eligible for Medicaid or CHIP: Who remains uninsured, and why? Acad Pediatr. 2015;15(3 Suppl):S36–S43. doi: 10.1016/j.acap.2015.01.009. [DOI] [PubMed] [Google Scholar]
- 4.U.S. Census Bureau, Current Population Survey. Table HI08. Health insurance coverage status and type of coverage by selected characteristics for children under 18: 2014. https://www.census.gov/hhes/www/cpstables/032015/health/toc.htm. Accessed 25 November 2015.
- 5.US Census Bureau. Children Characteristics. 2014 American Community Survey 1-Year Estimates. http://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=ACS_14_1YR_S0901&prodType=table. Accessed 25 November 2015.
- 6.Flores G, Walker C, Lin H, Lee M, Fierro M, Henry M, et al. Design, methods, and baseline characteristics of the Kids’ Health Insurance by Educating Lots of Parents (Kids’ HELP) trial: A randomized, controlled trial of the effectiveness of parent mentors in insuring uninsured minority children. Contemp Clin Trials. 2015;40:124–137. doi: 10.1016/j.cct.2014.11.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Texas Medical Association. The uninsured in Texas. http://www.texmed.org/uninsured_in_texas/. Accessed 2 February 2016.
- 8.Henry J. Kaiser Family Foundation. State health facts. Health insurance coverage of children 0-18. http://kff.org/other/state-indicator/children-0-18/. Accessed 2 February 2016.
- 9.Children’s Health. Beyond abc. Assessing the well-being of children in Dallas County and the North Texas corridor 2015. https://www.childrens.com/keeping-familieshealthy/community-resources/health-information-resources/beyond-abc-reports. Accessed 2 February 2016.
- 10.Texas Health and Human Services Commission. CHIP/Children’s Medicaid. Can I get it? http://chipmedicaid.org/en/Can-I-Get-It Accessed 3 September 2014.
- 11.World Health Organization. What are social determinants of health? http://www.who.int/social_determinants/en/. Accessed 2 February 2016.
- 12.Health Resources and Services Administration, Maternal and Child Health Bureau, Centers for Disease Control and Prevention, National Center for Health Statistics, State and Local Area Integrated Telephone Survey. National Survey of Children’s Health, 2003. Interview Sections 1-11. Atlanta, GA; Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/data/slaits/NSCH_Questionnaire.pdf. Accessed 10 September 2014.
- 13.Magee JC, Ritterband LM, Thorndike FP, Cox DJ, Borowitz SM. Exploring the relationship between parental worry about their children’s health and usage of an internet intervention for pediatric encopresis. J Pediatr Psychol. 2009;34(5):530–538. doi: 10.1093/jpepsy/jsn091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Szilagyi PG, Zwanziger J, Rodewald LE, Holl JL, Mukamel DB, Trafton S, et al. Evaluation of a state health insurance program for low-income children: implications for state child health insurance programs. Pediatrics. 2000;105(2):363–71. doi: 10.1542/peds.105.2.363. [DOI] [PubMed] [Google Scholar]
- 15.Moreno L, Hoag SD. Covering the uninsured through TennCare: does it make a difference? Health Aff (Millwood) 2001;20(1):231–9. doi: 10.1377/hlthaff.20.1.231. [DOI] [PubMed] [Google Scholar]
- 16.Szilagyi PG, Dick AW, Klein JD, Shone LP, Zwanziger J, McInerny T. Improved access and quality of care after enrollment in the New York State Children's Health Insurance Program (SCHIP) Pediatrics. 2004;113(5):e395–404. doi: 10.1542/peds.113.5.e395. [DOI] [PubMed] [Google Scholar]
- 17.Kempe A, Beaty BL, Crane LA, Stokstad J, Barrow J, Belman S, et al. Changes in access, utilization, and quality of care after enrollment into a state child health insurance plan. Pediatrics. 2005;115(2):364–71. doi: 10.1542/peds.2004-0475. [DOI] [PubMed] [Google Scholar]
- 18.Holl JL, Szilagyi PG, Rodewald LE, Shone LP, Zwanziger J, Mukamel DB, et al. Evaluation of New York State's Child Health Plus: access, utilization, quality of health care, and health status. Pediatrics. 2000;105(3 Suppl E):711–8. Accessed 10 September 2014. [PubMed]
- 19.Centers for Disease Control and Prevention. SLAITS National Survey of Children with Special Health Care Needs. Atlanta, GA; Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/data/slaits/NS-CSHCN%20Questionnaire%20(website)1.pdf. Accessed 10 September 2014.
- 20.Flores G, Snowden-Bridon C, Torres S, Perez R, Walter T, Brotanek J, et al. Improving asthma outcomes in minority children: A randomized, controlled trial of parent mentors. Pediatrics. 2009;124(6):1522–32. doi: 10.1542/peds.2009-0230. [DOI] [PubMed] [Google Scholar]
- 21.Centers for Disease Control and Prevention. SLAITS: The State and Local Area Integrated Telephone Survey. National Survey of Early Childhood Health. Appendix III. Atlanta, GA; Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/data/slaits/survey_sech00.pdf. Accessed 10 September 2014.
- 22.Agency for Healthcare Research and Quality . CAHPS Health Plan Survey 4.0. Version: Child Medicaid Questionnaire. Rockville: Agency for Healthcare Research and Quality; 2008. [Google Scholar]
- 23.Lewis CC, Scott DE, Pantell RH, Wolf MH. Parent satisfaction with children’s medical care: development, field test, and validation of a questionnaire. Med Care. 1986;24(3):209–215. doi: 10.1097/00005650-198603000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Lave JR, Keane CR, Lin CJ, Ricci EM, Amersbach G, LaVallee CP. Impact of a children’s health insurance program on newly enrolled children. JAMA. 1998;279(22):1820–1825. doi: 10.1001/jama.279.22.1820. [DOI] [PubMed] [Google Scholar]
- 25.Centers for Disease Control and Prevention . Draft 2009 NHIS Questionnaire - Sample Child. Atlanta: Centers for Disease Control and Prevention; 2009. [Google Scholar]
- 26.McPherson M, Arango P, Fox H, Lauver C, McManus M, Newacheck P, et al. A new definition of children with special health care needs. Pediatrics. 1998;102(1):137–140. doi: 10.1542/peds.102.1.137. [DOI] [PubMed] [Google Scholar]
- 27.Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800–812. doi: 10.1097/00005650-200108000-00006. [DOI] [PubMed] [Google Scholar]
- 28.Feinstein AR. Multivariable analysis: an introduction. New Haven: Yale University Press; 1996. [Google Scholar]
- 29.Flores G, Abreu M, Brown V, Tomany-Korman SC. How Medicaid and the State Children’s Health Insurance Program can do a better job of insuring uninsured children: the perspectives of parents of uninsured Latino children. Ambul Pediatr. 2005;5(6):332–340. doi: 10.1367/A04-067R2.1. [DOI] [PubMed] [Google Scholar]
- 30.Leverenz D, Flores G, Bridon C. Why are so many eligible children still uninsured? The perspectives of parents of uninsured African-American children. Abstract, 2010 American Public Health Association meeting. https://apha.confex.com/apha/138am/webprogram/Paper219447.html. Accessed 10 September 2014.
- 31.Heberlein M, Brooks T, Alker J, Artiga S, Stephens J. Getting into Gear for 2014: Findings from a 50-State Survey of Eligibility, Enrollment, Renewal, and Cost-Sharing Policies in Medicaid and CHIP, 2012–2013. Washington, DC: The Henry J. Kaiser Family Foundation; 2013. [Google Scholar]
- 32.Flores G, Abreu M, Chaisson CE, Meyers A, Sachdeva RC, Fernandez H, et al. A randomized trial of the effectiveness of community-based case management in insuring uninsured Latino children. Pediatrics. 2005;116(6):1433–1441. doi: 10.1542/peds.2005-0786. [DOI] [PubMed] [Google Scholar]
- 33.Flores G, Lin H, Walker C, Lee M, Currie J, Allgeyer R, et al. Parent mentors and insuring uninsured children: A randomized controlled trial. Pediatrics. 2016; In press. [DOI] [PMC free article] [PubMed]
- 34.Federico SG, Steiner JF, Beaty B, Crane L, Kempe A. Disruptions in insurance coverage: patterns and relationship to health care access, unmet need, and utilization before enrollment in the State Children’s Health Insurance Program. Pediatrics. 2007;120(4):e1009–e1016. doi: 10.1542/peds.2006-3094. [DOI] [PubMed] [Google Scholar]
- 35.Johnson WG, Rimsza ME. The effects of access to pediatric care and insurance coverage on emergency department utilization. Pediatrics. 2004;113(3 Pt 1):483–487. doi: 10.1542/peds.113.3.483. [DOI] [PubMed] [Google Scholar]
- 36.Flores G, Abreu M, Chaisson CE, Sun D. Keeping children out of hospitals: Parents’ and physicians’ perspectives on how pediatric hospitalizations for ambulatory sensitive conditions can be avoided. Pediatrics. 2003;112(5):1021–1030. doi: 10.1542/peds.112.5.1021. [DOI] [PubMed] [Google Scholar]
- 37.Hostetler SG, Xiang H, Kelleher K, Smith GA. Health care access after injury by insurance type in a pediatric population. Pediatr Emerg Care. 2005;21(7):420–426. doi: 10.1097/01.pec.0000169430.68325.a0. [DOI] [PubMed] [Google Scholar]
- 38.Braveman P, Oliva G, Miller MG, Reiter R, Egerter S. Adverse outcomes and lack of insurance among newborns in an eight-county area of California, 1982 to 1986. N Engl J Med. 1989;321(8):508–513. doi: 10.1056/NEJM198908243210805. [DOI] [PubMed] [Google Scholar]
- 39.Caskey RN, Davis MM. Differences associated with age, transfer status, and insurance coverage in end-of-life hospital care for children. J Hosp Med. 2008;3(5):376–383. doi: 10.1002/jhm.360. [DOI] [PubMed] [Google Scholar]
- 40.Hakmeh W, Barker J, Szpunar SM, Fox JM, Irvin CB. Effect of race and insurance on outcome of pediatric trauma. Acad Emerg Med. 2010;17(8):809–812. doi: 10.1111/j.1553-2712.2010.00819.x. [DOI] [PubMed] [Google Scholar]
- 41.Slifkin RT, Freeman VA, Silberman P. Effect of the North Carolina State Children’s Health Insurance Program on beneficiary access to care. Arch Pediatr Adolesc Med. 2002;156(12):1223–1229. doi: 10.1001/archpedi.156.12.1223. [DOI] [PubMed] [Google Scholar]
- 42.Dick AW, Brach C, Allison RA, Shenkman E, Shone LP, Szilagyi PG, et al. SCHIP’s impact in three states: how do the most vulnerable children fare? Health Aff (Millwood) 2004;23(5):63–75. doi: 10.1377/hlthaff.23.5.63. [DOI] [PubMed] [Google Scholar]
- 43.Chamberlain LJ, Hughes DC, Bishop JS, Matsuda DH, Sassoubre L. Universal health care coverage for children: impact on pediatric health care providers. J Health Care Poor Underserved. 2005;16(4):622–633. doi: 10.1353/hpu.2005.0090. [DOI] [PubMed] [Google Scholar]