

Abstract
Background:
Traumatic brain injury (TBI) is one of the leading causes of death. Evidence-based guidelines for TBI care have been widely discussed, but in-hospital treatment and outcome of these patients has been highly variable especially in developing countries like India.
Objectives:
To evaluate the epidemiology and outcome of patients with head injuries at a Level 1 trauma center in India.
Materials and Methods:
In this retro-prospective study, all patients with head injury who were admitted in the department of neurosurgery over a 15 months period (November 2007-January 2009) were included in the study. Post-resuscitation GCS was used for categorizing the severity of head injuries and outcome was assessed at discharge using GOS. All patients were managed as per laid down departmental protocols.
Results:
A total of 2068 patients of head injury were admitted during the study period. The mean age was 24 years (range 1-85). 71.4% were male and 28.6% were female. The most commonly involved age group was 20-40 years (43%) and the most common mode of injury was road traffic accidents (64%). 53% of the patients had severe head injury (GCS ≤ 8), 18% had moderate head injury (GCS 9 ≤ 13) and 29% had minor head injuries (GCS ≥ 14). The mean hospital stay was 14 days (range 1-62 days). Overall in-hospital mortality was 22% (454 cases). 39% died within 48 hours of injury. 2% of minor, 12% of moderate and 36% of severe head injured patients expired; Mortality was 38% in children (≤12 years). Amongst those who survived, 45% had good outcome (GOS 4 or 5), 13% were severely disabled (GOS 3) and 19% were vegetative (GOS 2).
Conclusions:
This is the one of the largest single center study on severe head injuries and shows enormity of the problem facing developing countries like India.
Keywords: Developing country, head injury, management, mortality, outcome
Introduction
Worldwide, head injury is the single largest cause of death and disability following injury.[1] Most head injuries are due to road side accidents.[2] The burden of head injury is greatest in low-and middle income countries (LAMIC), where 85% of the worlds population live.[3] The World Health Organization (WHO) estimates that almost 90% of deaths due to injuries occur in these settings.[1] Head Injury is the leading cause of disability in people under 40, severely disabling 150-200 people per million annually.[4,5] In 2005, road traffic injuries resulted in the death of an estimated 110,000 persons, 2.5 million hospitalizations, 8-9 million minor injuries and economic losses to the tune of 3% of the gross domestic product (GDP) in India.[6] The accident rate of 35 per 1000 vehicles in India is also amongst the highest in the world.[7] However, resources have not been diverted adequately by governments towards prevention, management and rehabilitation of head injuries in LAMIC such as India. In this study we attempt to assess the burden of head injury at single level 1 trauma center in New Delhi and to assess outcome in such patients.
Materials and Methods
In this retro-prospective study, all patients with head injury who were admitted in the department of neurosurgery in last 15 months period (November 2007-January 2009) were enrolled.
Patients with polytrauma admitted under other departments and patients who were not admitted were excluded from study. Post-resuscitation GCS was used for categorizing the severity of head injuries and outcome was assessed at discharge using GOS. All patients were managed as per laid down departmental protocols. Based on the post-resuscitation GCS, the head injury was categorized as minor head injury (GCS 13-15), moderate head injury (GCS 9-12) and severe head injury (GCS 8 or less).
Results
Demographics
A total 2068 patients of head injury were enrolled during the study period. The overall series was comprised of age group in the range from 1 to 85 years with mean of 24 years. The most commonly affected age group was between 21 and 40 years (41%). There were 71.5% males and 28.5% females. Most common mode of injury is from road traffic accidents seen in 64% of the cases followed by assault seen in 26% of the cases.
There were 598 (28.9%) minor, 380 (18.38%) moderate and 1090 (52.7%) severe head injuries.
Management
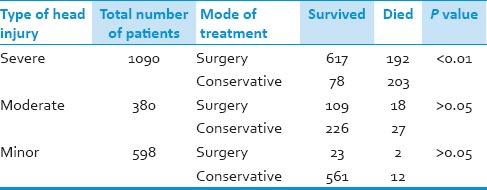
Amongst the 598 minor head injuries, 573 (95.8%) were managed conservatively and 25 (4.2%) underwent surgery for various mass lesions. In the 380 moderate head injuries, 253 (66.6%) were managed conservatively and 127 (33.4%) underwent surgery. Of the 1090 severe head injuries, 286 (26.2%) were managed conservatively and 809 (74.2%) underwent surgery [Table 1].
Table 1.
Mode of treatment of patients with head injury. Patients with severe head injury who were operated had a significantly better outcome than those who were not operated
Outcome
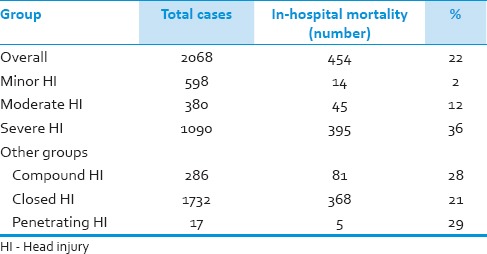
Hospital stay ranged from 1 to 62 (14 ± 2) days. The overall in-hospital mortality was 22% (n = 454). The mortality was 2% in patients with minor head injuries, 12% in patients with moderate head injuries and 36% in severe head injuries [Table 2].
Table 2.
In-hospital mortality of patients with head injury
Thirty-nine percent (n = 177) of the patients died within 48 hours of injury. Mortality was higher in the extremes of age. Children less than 12 years had 38% mortality and elderly (>50 years) carried 37% mortality rates following head injury.
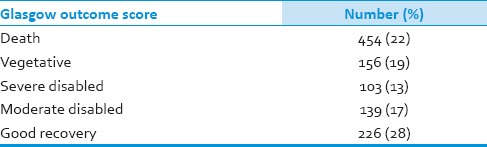
Amongst those who survived, 45% had good outcome (GOS 4 or 5), 13% were severely disabled (GOS 3) and 19% were vegetative (GOS 2) [Table 3].
Table 3.
Glasgow outcome score for the 2062 patients of head injury
Discussion
Incidence as well as severity of head injuries is rising in developing countries due to rapid industrialization with a lag in legal, healthcare and safety reforms. Delhi with a population of around 15 million has the dubious distinction of having the largest number of road traffic accidents of any city in India. The enormity of burden can be assessed by the fact that our study had 1090 severe head injured patients over 15 months and was conducted at only one hospital! One of the reasons for the step-motherly attitude by policy makers towards head injury prevention, management and rehabilitation is the lack of hard statistics of the actual burden of disease which head injuries carry.
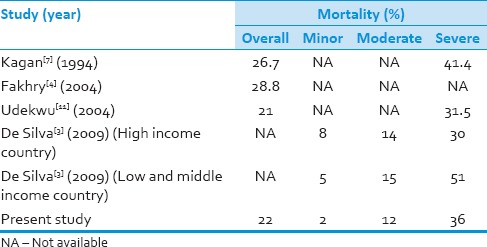
In spite of improvement in care for head injured patients, there has not been a marked decline in the mortality rates for severe head injuries. Kagan et al. found that mortality rates were between 26.7% and 41.4% for head injured patients in Level 1 trauma centers.[8] Fakhry et al. in their study found 28.8% mortality rate of severely head injured patients.[9] It has also been shown that developing (low and middle income) countries have a pooled mortality rate of 51% for severe head injuries as compared to 30% for high income countries.[3] The present study has an overall mortality of 22% with the mortality for severely head injured patients being is 36%. This is very favorably comparable to other studies [Table 4]. However, this mortality does not reflect the outcome in other centers in India where optimum treatment cannot be provided due to lack of resources.
Table 4.
Comparison with literature for outcome after mild, moderate and severe head injuries
In our center we follow a policy of aggressive monitoring and management of severe head injuries as published by Stein et al.[10] This has helped us in having outcomes better than the national average and to continually improve upon them over the years. In our study only 26.2% of the severe head injuries were managed conservatively with an extremely high mortality of 72%. The remaining 809 patients (74.2%) of severe head injury underwent aggressive management with surgery with a mortality of only 23.7%. This brings out the fact that aggressive monitoring and management has dramatically improved outcome in our hands.
Although minor head injuries constitute the largest group of head injuries, they do not reflect in this study as majority were kept under observation in the emergency department and not admitted. This also reflects on the immense pressure on in-hospital beds, thus keeping minor head injury admissions to the minimum. However, in spite of selective admission criteria for minor head injuries, our mortality rate is better than published.[3]
Conclusion
This is the largest study of its kind from India which shows mortality rates and outcome in patients with head injuries and shows enormity of the problem which developing countries like India face. Our mortality rates for head injured patients compare very favorably with international data.11
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349:1436–42. doi: 10.1016/S0140-6736(96)07495-8. [DOI] [PubMed] [Google Scholar]
- 2.Rajendra PB, Mathew TP, Agrawal A, Sabharawal G. Characteristics of associated craniofacial trauma in patients with head injuries: An experience with 100 cases. J Emerg Trauma Shock. 2009;2:89–94. doi: 10.4103/0974-2700.50742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.De Silva MJ, Roberts I, Perel P, Edwards P, Kenward MG, Fernandes J, et al. Patient outcome after traumatic brain injury in high-, middle- and low-income countries: Analysis of data on 8927 patients in 46 countries. Int J Epidemiol. 2009;38:452–8. doi: 10.1093/ije/dyn189. [DOI] [PubMed] [Google Scholar]
- 4.Fleminger S, Ponsford J. Long term outcome after traumatic brain injury. BMJ. 2005;331:1419–20. doi: 10.1136/bmj.331.7530.1419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bruns J, Jr, Hauser WA. The epidemiology of traumatic brain injury: A review. Epilepsia. 2003;44:2–10. doi: 10.1046/j.1528-1157.44.s10.3.x. [DOI] [PubMed] [Google Scholar]
- 6.Gururaj G. Road traffic deaths, injuries and disabilities in India: Current scenario. Natl Med J India. 2008;21:14–20. [PubMed] [Google Scholar]
- 7.Dandona R, Kumar GA, Ameer MA, Ahmed GM, Dandona L. Incidence and burden of road traffic injuries in urban India. Inj Prev. 2008;14:354–9. doi: 10.1136/ip.2008.019620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kagan RJ, Baker RJ. The impact of the volume of neurotrauma experience on mortality after head injury. Am Surg. 1994;60:394–400. [PubMed] [Google Scholar]
- 9.Fakhry SM, Trask AL, Waller MA, Watts DD. IRTC Neurotrauma Task Force. Management of brain-injured patients by an evidence-based medicine protocol improves outcomes and decreases hospital charges. J Trauma. 2004;56:492–500. doi: 10.1097/01.ta.0000115650.07193.66. [DOI] [PubMed] [Google Scholar]
- 10.Stein SC, Georgoff P, Meghan S, Mirza KL, El Falaky OM. Relationship of aggressive monitoring and treatment to improved outcomes in severe traumatic brain injury. J Neurosurg. 2010;112:1105–12. doi: 10.3171/2009.8.JNS09738. [DOI] [PubMed] [Google Scholar]
- 11.Udekwu P, Kromhout-Schiro S, Vaslef S, Baker C, Oller D. Glasgow Coma Scale score, mortality, and functional outcome in head-injured patients. J Trauma. 2004;56:1084–9. doi: 10.1097/01.ta.0000124283.02605.a5. [DOI] [PubMed] [Google Scholar]