

Abstract
An azygos anterior cerebral artery (ACA) is a rare variant of normal embryogenesis in which confluence of two A1 segments results in a single A2 segment with the absence of anterior communicating artery. The occurrence of an aneurysm at the bifurcation of azygos ACA is rare with few cases reported in the literature. We report a case of a 40-year-old lady who presented with subarachnoid hemorrhage following rupture of a giant, saccular distal azygos ACA aneurysm. Bifrontal craniotomy and clipping of an aneurysm was performed. The clinical significance of azygos ACA and surgical strategies in clipping these aneurysms are discussed with a review of literature.
Keywords: Anterior cerebral artery, azygos artery, saccular aneurysm
Introduction
Azygos anterior cerebral artery (azygos ACA) is a rare anatomical variation of the circle of Willis with a low incidence of 1% to 4%.[1,2,3,4] In this variant of normal embryogenesis, the confluence of both A1 segments results in formation of single distal ACA in the interhemispheric fissure.[1,3,5] This unique vascular configuration results in increased hemodynamic stress at the bifurcation of distal ACA predisposing to aneurysm formation.[2,3,6] The complex aneurysmal morphology makes surgical intervention challenging. We report a patient with giant, saccular, bilobed distal azygos ACA aneurysm, and discuss the surgical challenges.
Case Report
A 40-year-old lady presented to the Emergency Department with sudden onset severe bifrontal headache associated with one episode of vomiting. She had no loss of consciousness. Her past medical history was not significant except for occasional bouts of headache, which was relieved by analgesics. Her vital parameters were normal - pulse 78/min and blood pressure of 140/80 mm Hg. She was conscious alert with no motor deficit (World Federation of Neurosurgical Societies grade 1). Emergency noncontrast computerized tomography (CT) scan of the brain was performed, which revealed subarachnoid hemorrhage in interhemispheric fissure with right frontal hematoma and extension of the hematoma in the right lateral ventricle and third ventricle [Figure 1a]. In the Intensive Care Unit, she received antiedema measures, antiepileptics, and adequate hydration. She underwent CT angiogram of the brain that revealed single, giant, bilobed, and saccular aneurysm in the interhemispheric fissure at the genu of corpus callosum. The distal ACA was unpaired. An aneurysm was arising from the bifurcation of this azygos A2 segment. It was directed anteriorly with the fundus buried in both cingulate gyrus and medial frontal lobe. The teat was directed anteriorly and to the left [Figure 1b–d]. A right frontal craniotomy was performed on the 2nd day of bleed. The brain was tense on opening the dura mater. The right frontal hematoma was evacuated. The interhemispheric fissure was dissected out, and the proximal azygos A2 segment was identified. It was traced distally at its bifurcation to identify the aneurysm and the two A3 segments (pericallosal arteries). The neck of the aneurysm was identified, and the entire aneurysm was dissected out using temporary clip on azygos A2 segment for the duration of approximately 5 min. Two permanent Yasargil clips were applied at the neck of an aneurysm - one a straight and other right angled fenestrated clip to obliterate the neck completely. The flow in the distal A3 segments was confirmed using intraoperative Doppler. Postoperative recovery was uneventful. Follow-up CT angiogram done showed complete obliteration of an aneurysm with patency of the parent azygos ACA and distal pericallosal arteries [Figure 2a and b].
Figure 1.
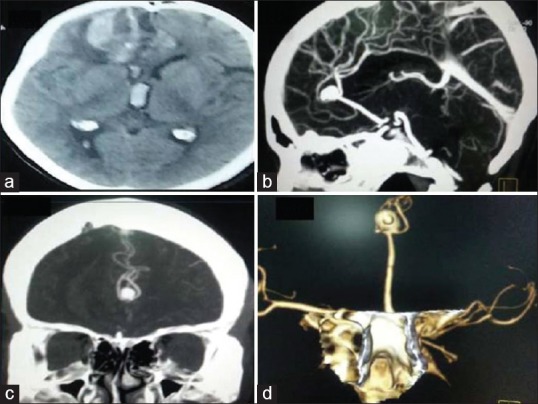
Plain computerized tomography of the brain reveals subarachnoid hemorrhage in interhemispheric fissure with right frontal hematoma and extension of the hematoma in the right lateral ventricle and third ventricle (a). Computerized tomography angiogram of the brain revealed single, giant, bilobed, saccular aneurysm in the interhemispheric fissure at the genu of corpus callosum (b). The aneurysm is arising from the bifurcation of distal azygos A2 segment with the teat directed anteriorly and to the left (b-d)
Figure 2.
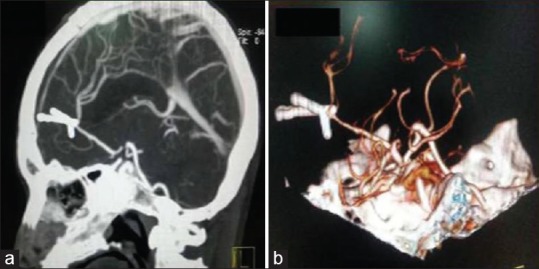
Postoperative computerized tomography angiogram of the brain showed complete obliteration of the aneurysm with patency of the parent azygos anterior cerebral artery and distal pericallosal arteries (a and b). Two permanent Yasargil clips were applied at the neck of the aneurysm - one a straight and other right angled fenestrated clip
Discussion
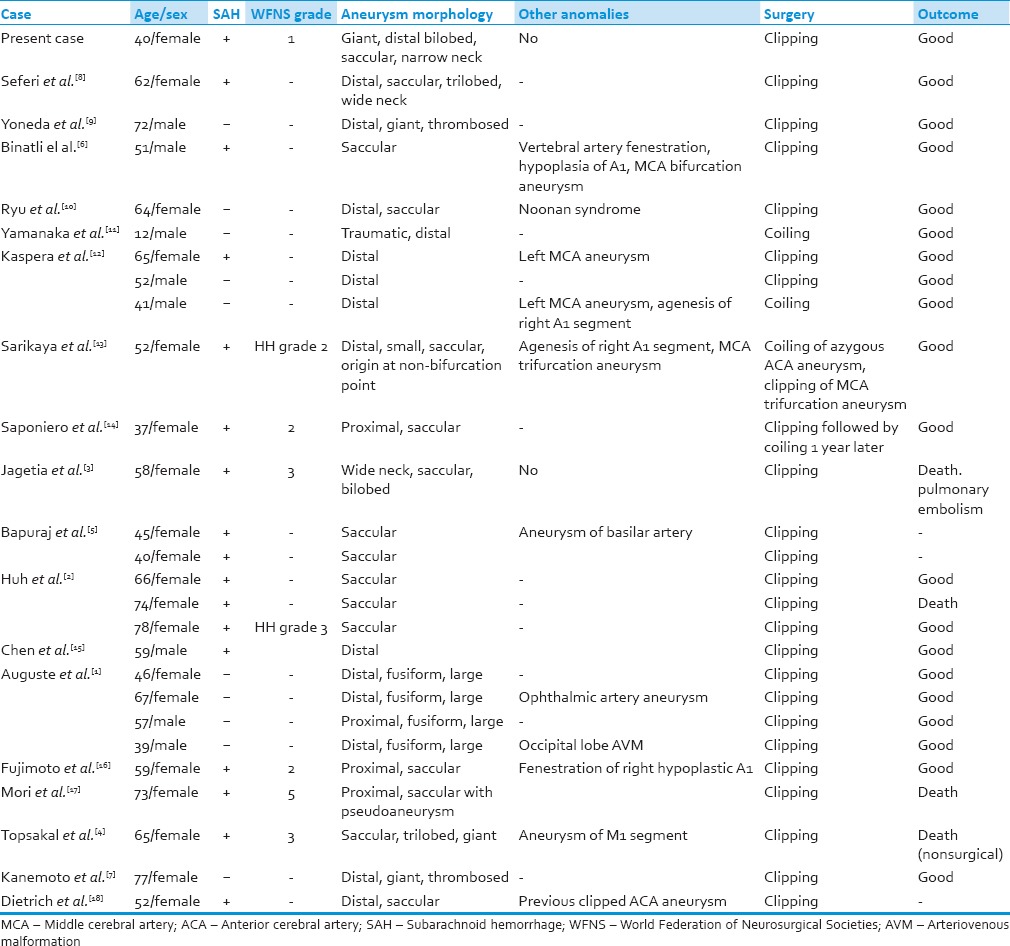
Unpaired distal ACA, also known as azygos ACA, is an uncommon vascular anomaly of the circle of Willis.[1,4] In this variant of normal embryogenesis, the anterior communicating artery is absent. The right and left horizontal A1 segments join to form a single A2 segment in the interhemispheric fissure.[1,3,5] This rare anatomical variation is commonly seen in lower animals such as snakes, crocodiles, and lower primates.[5] Based on angiographic studies in adult population or cadaveric series, it has a very low incidence of 1–4%.[2,3,4] This unique vascular configuration predisposes to aneurysm formation. The incidence of aneurysm formation in azygos ACA is high ranging between 13% and 71%.[5,6,7] Most of the aneurysms at the distal end of the azygos ACA are single, saccular, and small in size.[3,5,6] Very few cases with nonsaccular morphology and giant ACA aneurysms have been reported.[1,4,7] Table 1 summarizes all cases of azygos ACA aneurysms reported in the literature since the year 2000.[1,3,5,6,7,8,9,10,11,12,13,14,15,16,17,18]
Table 1.
Summarizes all cases of azygos ACA aneurysms reported in the literature since the year 2000
Baptista after a review of 381 brain specimens described three types of distal ACA.[12] Type 1 is single, unpaired distal ACA, also called azygos ACA, which gives off branches to medial surface of both the cerebral hemispheres. Type 2 is “bihemispheric” ACA, in which both A2 segments are present. However, one of the A2 segment is dominant and gives branches to both the hemispheres while the other A2 segment is either hypoplastic or terminates early. Type 3 is accessory ACA in which a third artery arises from the anterior communicating segment in addition to paired A2 segments.[12] Type 1 variant of distal ACA has significant clinical relevance than the other two types. This unusual vascular configuration is associated with other anomalies such as neuronal migration defects, holoprosencephaly, agenesis of corpus callosum, saccular aneurysms, and arteriovenous malformation.[2,3,5]
This anatomic transition from paired A2 segment to a single, unpaired A2 segment of ACA originates either from the medial branch of the primitive olfactory artery at the initial 16 mm to 18 mm stage of embryogenesis or due to persistence of the median artery of the corpus callosum at 20 mm to 24 mm stage with regression or lack of development of the ACA.[3,6]
Azygos ACA bifurcates into bilateral pericallosal and callosomarginal arteries typically at the genu of corpus callosum, supplying the medial surface of both frontal lobes and a large part of corpus callosum.[1,3,5] Azygos ACA carries twice the blood flow as compared to paired A2 segment increasing the hemodynamic stress at its bifurcation, thereby increasing the susceptibility of aneurysm formation.[2,3,6] This is more so if the diameter of azygos ACA is equal to A1 segment. On the contrary Kaspera et al. have suggested that the complex geometry at the bifurcation of azygous ACA, along with the bend at the genu of corpus callosum may be responsible for aneurysm formation rather than merely increased blood flow velocity in azygos ACA.[12]
The rarity of this anatomical variant along with aneurysm formation poses a serious surgical challenge. Clipping of aneurysms of azygos ACA carries more risk as compared to those with paired A2 segments.[1,6] With the advent of endovascular therapy, neurosurgeons are less likely to be exposed to the art of clipping simple as well as complex aneurysms. Complex aneurysmal morphology, as in the present case with giant azygos ACA an aneurysm, makes it all the more challenging. In large and giant azygos, ACA an aneurysm with complex morphology, proximal control of the azygos ACA is essential to dissect the neck of aneurysm for permanent clip application. In order to place the temporary clip on the azygos ACA, neurosurgeons need to navigate deep into the interhemispheric fissure.[1] Hence, the dome of an aneurysm may be encountered, prior to the azygos ACA, with catastrophic consequences, especially in ruptured aneurysms.[1] The duration of temporary clipping of the azygos ACA during neck dissection has to be judicious. Prolonged temporary clipping of the azygos ACA is likely to result in ischemic insult to both the medial frontal lobe and corpus callosum with tragic results.[3] Once an aneurysm is clipped, the patency of the distal vessels needs to be confirmed by intraoperative Doppler or intraoperative angiogram. Compromise of any of the pericallosal or callosomarginal arteries or luminal narrowing or kinking of the azygos ACA needs to be ruled out.[5] Large or giant azygos ACA aneurysms also need complex and multiple clip placements to obliterate the aneurysm neck completely preserving the distal vessels.
In the present case, patient presented with subarachnoid hemorrhage due to rupture of distal azygos ACA an aneurysm. The aneurysm was giant, bilobed, saccular with narrow neck and angiogram did not demonstrate any other associated anomalies. The occurrence of giant distal ACA aneurysms in the present case could be due to increased hemodynamic stress or complex geometry at the branching of the azygos ACA. Proximal control of the azygos ACA was achieved in order to dissect the neck of the aneurysm. Two clips - one straight and other right angled fenestrated had to be applied in order to obliterate the neck completely. Patency of the distal vessels was confirmed on Doppler. The good outcome in this patient was due to meticulous surgical planning and technique.
Conclusion
Azygos ACA is a rare anatomical variant associated with aneurysm formation at its bifurcation. The complex aneurysmal morphology of azygos ACA merits meticulous surgical planning. Preserving the proximal azygos ACA as well distal pericallosal arteries, during clipping the aneurysm neck, is of paramount importance to avoid potentially threatening neurological morbidity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Auguste KI, Ware ML, Lawton MT. Nonsaccular aneurysms of the azygos anterior cerebral artery. Neurosurg Focus. 2004;17:E12. doi: 10.3171/foc.2004.17.5.12. [DOI] [PubMed] [Google Scholar]
- 2.Huh JS, Park SK, Shin JJ, Kim TH. Saccular aneurysm of the azygos anterior cerebral artery: Three case reports. J Korean Neurosurg Soc. 2007;42:342–5. doi: 10.3340/jkns.2007.42.4.342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jagetia A, Kumar PN, Sinha S, Sharma A. Saccular bilobed aneurysm of an azygos anterior cerebral artery. J Clin Neurosci. 2007;14:777–9. doi: 10.1016/j.jocn.2006.02.005. [DOI] [PubMed] [Google Scholar]
- 4.Topsakal C, Ozveren MF, Erol FS, Cihangiroglu M, Cetin H. Giant aneurysm of the azygos pericallosal artery: Case report and review of the literature. Surg Neurol. 2003;60:524–33. doi: 10.1016/s0090-3019(03)00319-7. [DOI] [PubMed] [Google Scholar]
- 5.Bapuraj JR, Ojili V, Khandelwal N, Kaza RK, Shanbhogue AK, Chabbra R. Case series: Saccular aneurysm of the azygos anterior cerebral artery: Report of 2 cases and review of literature. Indian J Radiol Imaging. 2007;17:153–5. [Google Scholar]
- 6.Binatli Ö, Özer F, Aydin M, Çiçek E, Binatli Y. Azygos anterior cerebral artery aneurysm with concomittant vascular anomaly: Case report. World J Neurosci. 2013;3:49–51. [Google Scholar]
- 7.Kanemoto Y, Tanaka Y, Nonaka M, Hironaka Y. Giant aneurysm of the azygos anterior cerebral artery – Case report. Neurol Med Chir (Tokyo) 2000;40:472–5. doi: 10.2176/nmc.40.472. [DOI] [PubMed] [Google Scholar]
- 8.Seferi A, Alimehmeti R, Rroji A, Petrela M. Saccular trilobed aneurysm of azygos anterior cerebral artery. World J Clin Cases. 2015;3:377–80. doi: 10.12998/wjcc.v3.i4.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yoneda H, Suzuki M, Ishihara H, Koizumi H, Nomura S, Fujii M. A case of thrombosed giant aneurysm of the azygos anterior cerebral artery: Clipping under monitoring of motor evoked potentials of the lower extremities. Neurol Med Chir (Tokyo) 2014;54:205–10. doi: 10.2176/nmc.cr2012-0343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ryu B, Sato S, Yamaguchi K, Abe K, Ottomo D, Okada Y. Azygos anterior cerebral artery aneurysm in a patient with Noonan syndrome. No Shinkei Geka. 2013;41:773–7. [PubMed] [Google Scholar]
- 11.Yamanaka K, Ishihara M, Nakajima S, Yamasaki M, Yoshimine T. Coil embolization of a traumatic intracranial aneurysm of the distal part of the azygos anterior cerebral artery followed up for 4 years. Neurol Med Chir (Tokyo) 2011;51:572–5. doi: 10.2176/nmc.51.572. [DOI] [PubMed] [Google Scholar]
- 12.Kaspera W, Ladzinski P, Slowinski J, Kopera M, Tomalski W, Slaska-Kaspera A. Blood flow velocity in the arteries of the anterior cerebral artery complex in patients with an azygos anterior cerebral artery aneurysm: A transcranial color-coded sonography study. Clin Neurol Neurosurg. 2009;111:63–8. doi: 10.1016/j.clineuro.2008.08.007. [DOI] [PubMed] [Google Scholar]
- 13.Sarikaya B, Oksuz E, Deniz FE, Firat MM. Endovascular treatment of a ruptured aneurysm at a very rare location. Distal azygos anterior cerebral artery. Interv Neuroradiol. 2008;14:457–60. doi: 10.1177/159101990801400413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Saponiero R, Toriello A, Locatelli G, Pugliese ND, Napoli AN, Napoli M, et al. Distal anterior cerebral artery aneurysms: Endovascular or surgical treatment? A case report. Neuroradiol J. 2008;21:251–4. doi: 10.1177/197140090802100217. [DOI] [PubMed] [Google Scholar]
- 15.Chen CY, Hsieh SC, Choi WM, Chiang PY, Chien JC, Chan WP. Computed tomography angiography in detection and characterization of ruptured anterior cerebral artery aneurysms at uncommon location for emergent surgical clipping. Clin Imaging. 2006;30:87–93. doi: 10.1016/j.clinimag.2005.09.022. [DOI] [PubMed] [Google Scholar]
- 16.Fujimoto Y, Yamanaka K, Nakajima Y, Yoshimura K, Yoshimine T. Ruptured aneurysm arising from the proximal end of an azygos anterior cerebral artery – Case report. Neurol Med Chir (Tokyo) 2004;44:242–4. doi: 10.2176/nmc.44.242. [DOI] [PubMed] [Google Scholar]
- 17.Mori K, Kasuga C, Nakao Y, Yamamoto T, Maeda M. Intracranial pseudoaneurysm due to rupture of a saccular aneurysm mimicking a large partially thrombosed aneurysm (“ghost aneurysm”): Radiological findings and therapeutic implications in two cases. Neurosurg Rev. 2004;27:289–93. doi: 10.1007/s10143-004-0336-7. [DOI] [PubMed] [Google Scholar]
- 18.Dietrich W, Reinprecht A, Gruber A, Czech T. De novo formation and rupture of an azygos pericallosal artery aneurysm. Case report. J Neurosurg. 2000;93:1062–4. doi: 10.3171/jns.2000.93.6.1062. [DOI] [PubMed] [Google Scholar]