

Abstract
Introduction
The treatments for which mineral trioxide aggregate (MTA)-based materials can be used in dentistry are expanding. Smaller particle size and easier handling properties have allowed the advent of tricalcium silicate sealers including EndoSequence BC Sealer (Brasseler USA, Savannah, GA), QuickSet2 (Avalon Biomed, Bradenton, FL), NeoMTA Plus (Avalon Biomed), and MTA Fillapex (Angelus, Londrina, Brazil). The objective of this study was to measure the tubule penetration with these sealers using continuous wave (CW) and single-cone (SC) obturation techniques.
Methods
Eighty single-rooted teeth were randomly divided into 8 groups of 10 and obturated with 1 of the previously mentioned sealers mixed with trace amounts of rhodamine using either the CW or SC technique. Teeth were sectioned at 1 mm and 5 mm from the apex and examined under a confocal laser microscope. The percentage of sealer penetration and the maximum sealer penetration were measured.
Results
The tricalcium silicate sealers penetrated tubules as deep as 2000 μm (2 mm). The percentage of sealer penetration was much higher 5 mm from the apex, with many specimens having 100% penetration for both SC and warm vertical techniques. MTA Fillapex, a resin-based sealer with less than 20% MTA particles, had significantly greater tubule penetration with a warm vertical technique versus the SC technique at the 1-mm level.
Conclusions
Within the limitations of this study, the CW and SC techniques produced similar tubule penetration at both the 1-mm and the 5-mm level with the tricalcium silicate sealers BC Sealer, QuickSet2, and NeoMTA Plus.
Keywords: BC Sealer, NeoMTA Plus, QuickSet2, tricalcium silicate sealers, tubule penetration
Mineral trioxide aggregate (MTA) is a versatile and bioactive material that has proven to be an important asset in the endodontic armamentarium (1) for surgical procedures such as root end fillings, perforation repairs, or apexification. MTA has also been used for vital pulp therapy including pulp capping, pulpotomies, and revascularization procedures. More recently, MTA has been developed for use as an endodontic sealer (2).
The original MTA products were difficult to manipulate and relatively coarse, which prevented the achievement of the low film thickness needed for root canal sealers (3). Newer tricalcium silicate products are more suitable for use as a sealer. EndoSequence BC Sealer (Brasseler USA, Savannah, GA) is a single-component sealer that sets in vivo when water diffuses into the sealer. MTA Fillapex (Angelus, Londrina, Brazil) is a 2-component resin-based sealer containing less than 20% MTA filler. NeoMTA Plus and QuickSet2 (Avalon Biomed, Bradenton, FL) kits contain powder and a water-based gel. When the powder to gel ratio is low, a sealer-type consistency is obtained for these 2 materials. These latter 2 products are indicated for sealer and other procedures depending on the consistency chosen by the clinician although QuickSet2 is experimental.
Two techniques are advocated for sealers: a single-cone (SC) obturation technique and a warm vertical condensation (continuous wave [CW]) technique. Studies show that the application of heat (CW technique) may affect the properties of some tricalcium silicate sealers (4, 5). BC Sealer is solely indicated for the SC technique (6). The suitability of the SC and CW compaction techniques has not been compared for the newer sealers like NeoMTA Plus and QuickSet2.
One measure of a sealer's performance is its ability to penetrate the dentinal tubules. De-Deus et al (7) found no correlation between sealer penetration and sealability of obturation materials. However, the penetration of root canal sealer into the dentinal tubules forms a physical barrier (8), improves retention of the root filling (9), and entombs residual bacteria (10). The farther a sealer can penetrate the tubules, the more it can exert its antibacterial effect, if present (11). For instance, BC Sealer and AH Plus (Patterson Dental, Southlake, TX) killed bacteria beyond the penetration of the sealer (11).
Physical and chemical properties, such as particle size, solubility, viscosity, and surface tension, influence the depth and consistency of the material's dentin tubule penetration (10). Bird et al (12) tested the ability of ProRoot MTA (Dentsply, Tulsa, OK) and Capasio root end filling materials (Avalon Biomed) to penetrate dentin tubules; the calcium aluminosilicate Capasio was superior. Finer particle sizes of tricalcium silicate–based materials are now available. QuickSet2 is a calcium aluminosilicate produced as a derivative of Capasio with similar properties as well as particle size but a modified gel. NeoMTA Plus is a tricalcium silicate material. Each material sets with water but has different solubility reactions before setting. The proprietary gels for both QuickSet2 and NeoMTA impart easy handling properties, and the consistency can be varied for use as an orthograde sealer or a retro filling material. BC Sealer is a tricalcium silicate material that is a premixed product for use as a sealer only and relies on water in the tubules to hydrate and harden the tricalcium silicate (13–16). No study has yet compared tubule penetration of tricalcium silicate–based sealers.
The objective of this study was to measure the tubule penetration with 4 sealers: 1 advocated for use with the CW technique (MTA Fillapex), 1 with the SC technique (BC Sealer), and the other 2 (QuickSet2 and NeoMTA) untested for either obturation techniques. For equivalence, all materials were tested using both the SC and CW techniques.
Materials and Methods
This study was approved as an exempt study by the Institutional Review Board of the Texas A&M University Baylor College of Dentistry, Dallas, Texas, and followed the required guidelines for exempt studies. Eighty single-rooted human teeth with fully formed apices (including bicuspids, canines, and incisors) were collected anonymously from several dental offices (general dentists, oral surgeons, and periodontists) and stored in distilled water until all teeth were accumulated. All teeth were decoronated, and the root was cut to a 12-mm length. The working length was established by subtracting 1 mm from the total root length. Roots were instrumented in a crown-down fashion and then apically enlarged to size 40 using 0.06 taper nickel-titanium rotary instruments (EndoSequence, Brasseler USA).
During instrumentation, the canals were irrigated with ∼1 mL sodium hypochlorite between each instrument using a 30-G side-vented needle to the working length. The final irrigation was 3 mL 17% EDTA for 1 minute followed by 3 mL 6% sodium hypochlorite for 1 minute and a rinse with 5 mL saline for 1 minute. The needle was 1 mm from the apex at the final rinse. Roots were stored in distilled water at room temperature until obturation. Just before obturation, canals were dried with paper points (Brasseler USA). The roots were randomly assigned into 4 groups: BC Sealer, MTA Fillapex, NeoMTA Plus, and QuickSet2. Each group was further subdivided into groups for SC or CW obturation.
The sealers were mixed according to each manufacturer's directions, except for BC Sealer, which required no mixing. A trace amount of rhodamine dye was picked up with an endodontic explorer and mixed into each sealer. For the SC technique, the master cone (size 40/0.06) was used to coat the walls of the canal with sealer. The cone was recoated with sealer and seated in the canal. The cone was seared off at the level of the orifice and lightly condensed with a plugger. For CW, the sealer and cone were seated as in the SC technique, and then the system B unit (SybronEndo, Orange, CA) was used at 200°C to remove the gutta-percha 3 mm short of the working length followed by condensation with a plugger. Backfilling was performed with the Super-Endo Beta Main Unit (B&L Biotech USA, Bala Cynwyd, PA) at 200 ° C followed by condensation with a plugger. All specimens were stored for 2 weeks at 37°C in 100% humidity to allow the sealers to set.
After 2 weeks, the teeth were embedded centrally and vertically in orthodontic resin (Dentsply Caulk, Milford, DE). Specimens were stored in a humidity chamber at room temperature for the remainder of the study (ie, 6–9 weeks). Each root was horizontally sectioned using a diamond blade on an Isomet saw (Buehler, Lake Bluff, IL), removing a 1-mm-thick section at 1 and 5 mm from the root apex. The coronalfacing surface of each section was polished for 10 seconds on each side with each grit, with progressively finer grits of silicon carbide abrasive papers of 800, 1000, and 1200 (Allied High Tech Products, Inc, Compton, CA). The polished sections were imaged using a confocal laser scanning microscope (TCS SP5; Leica, Mannheim, Germany) at 5 × magnification. Photos of each section were evaluated with NIS-Elements Br 3.0 imaging software (Nikon, Tokyo, Japan) using a calibrated measuring tool. The percentage of sealer penetration and the maximum depth of sealer penetration were measured using the methods from Bolles et al (13). For the percentage of sealer penetration, the portions of the canal circumference in which tubule penetration was seen were measured and added, and this length was divided by the total circumference of the canal wall. The maximum depth of sealer penetration was measured directly, from the canal wall to the deepest point at which the sealer was visualized. However, this maximum was not necessarily uniform around the circumference.
The differences between the 1- and 5-mm levels within each group were analyzed using the Wilcoxon signed rank sum test. Data were not normally distributed, so nonparametric tests were performed. The data file was split by technique, and Kruskal-Wallis analysis was used for overall comparisons. A series of Mann-Whitney U tests were used for pair-wise comparisons. The data file was split by sealer, and Mann-Whitney analysis was used to compare the 2 obturation techniques within the sealer groups. Significance for the post hoc tests was adjusted by using the Bonferroni method such that P values <.0125 were considered significant.
Results
The sealer with the rhodamine dye fluoresced red under the confocal laser scanning microscope (Fig. 1).
Figure 1.
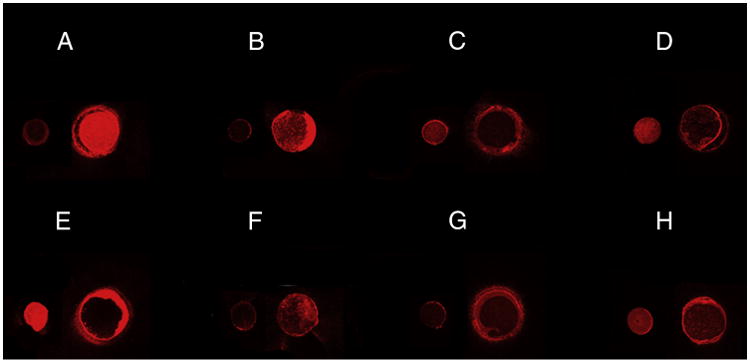
Confocal images of representative sections measured at 1 mm from the apex on the left and 5 mm from the apex on the right for each material. (A) BC Sealer with the SC technique, (B) MTA Fillapex with the SC technique, (C) NeoMTA Plus with the SC technique, (D) QuickSet2 with the SC technique, (E) BC Sealer with the CW technique, (F) MTA Fillapex with the CW technique, (G) NeoMTA Plus with the CW technique, and (H) QuickSet2 with the CW technique.
Sealer Penetration Using the SC Technique
The sealer penetrated both deeper and more evenly around the circumference of the canal at the 5-mm level compared with the 1-mm level (Fig. 1A–D). At 1 mm from the apex, the average maximum depth of penetration for each group was less than 0.2 mm. The range of percentage sealer penetration for each group was 0%–30%, except for BC Sealer, which was between 40% and 50% (Fig. 1A). At 5 mm from the apex, the average maximum sealer penetration for all groups was between 0.3 and 1.5 mm. The average percent of sealer penetration was >80% for all groups, except MTA Fillapex, which was less than 80% (Fig. 1B). MTA Fillapex had the most variable results of all groups at the 5-mm level (Fig. 1B). There was no significant difference for maximum sealer penetration among the sealers when used with the SC technique.
Sealer penetration was significantly higher, both in percentage and depth, at the 5-mm distance from the apex compared with the 1-mm level (Fig. 2). At the 1-mm level, the results were more variable and lower in penetration percentage and depth (Fig. 2A and C). NeoMTA Plus had the deepest and greatest percentage of penetration with the SC technique compared with all other sealers.
Figure 2.
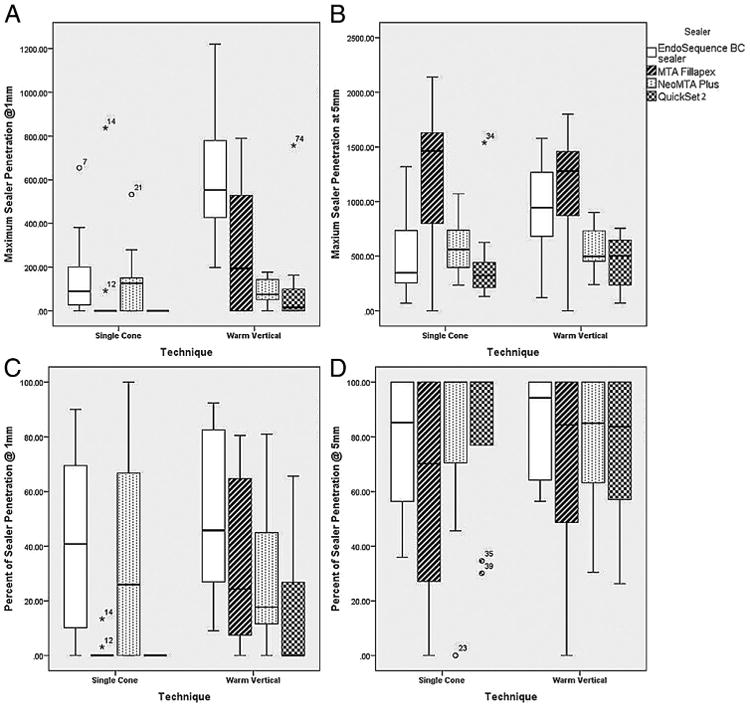
(A) Maximum sealer penetration at 1 mm. (B) Maximum sealer penetration at 5 mm. (C) Percentage of sealer penetration at 1 mm. (D) Percentage of sealer penetration at 5 mm.
MTA Fillapex had the numerically lowest mean sealer penetration circumferentially and the greatest range in percentage of sealer penetration with the SC technique compared with all other groups at the 5-mm level although this was not statistically different (Fig. 2D). BC Sealer had significantly more and deeper sealer penetration circumferentially than MTA Fillapex or QuickSet2 at the 1-mm level (Fig. 2A). NeoMTA Plus had the widest range of sealer penetration circumferentially, with the mean lying between BC Sealer and MTA Fillapex/QuickSet2 (Fig. 2A).
Sealer Penetration with CW
The sealers penetrated both deeper and more evenly around the circumference of the canal at the 5-mm level compared with the 1mm level (Fig. 1). At 1 mm from the apex, the average maximum depth of penetration for each group was less than 0.2 mm, except for BC Sealer, which was greater than this with the CW technique (Fig. 1E).
The range of percentage sealer penetration for each group was 0%– 30%, except for BC Sealer, which was between 40% and 50% with CW (Fig. 1E). At 5 mm from the apex, the average maximum sealer penetration for all groups was between 0.3 and 1.5 mm. The average percent of sealer penetration was >80% for all groups. MTA Fillapex had the most variable results of all groups at the 5-mm level with the CW technique (Fig. 1F).
Sealer penetration was significantly higher, both in percentage and depth, at the 5-mm distance from the apex compared with the 1-mm level with the CW technique (Fig. 2). At the 1-mm level, the results were more variable and lower in penetration percentage and depth (Fig. 2A and C).
NeoMTA Plus had the widest range of sealer penetration circumferentially, with the mean lying between BC Sealer and MTA Fillapex/QuickSet2 (Fig. 2A). Within the CW group, BC Sealer had significantly deeper and greater sealer penetration circumferentially than QuickSet2 (Fig. 2A and C).
Comparison of SC Versus CW
At the 5-mm level, there was no significant difference in percentage of sealer penetration between the CW or SC technique between any of the sealers (Fig. 2D). However, significantly deeper sealer penetration occurred at the 5-mm level for both BC Sealer and MTA Fillapex over QuickSet2 when used with the CW technique compared with the SC technique (Fig. 2B).
The resin-based MTA Fillapex had significantly greater percentage of sealer penetration with the CW technique than the SC technique at 1 mm (Fig. 2C). BC Sealer had significantly deeper penetration with CW versus SC at the 1-mm level (Fig. 2A). The CW technique produced more and deeper sealer penetration than the SC technique at the 1-mm level for every sealer except NeoMTA Plus, which had a deeper and greater percentage of penetration with the SC technique. The differences between the CW and SC techniques were not statistically significant for NeoMTA Plus or QuickSet2.
The range of percentage sealer penetration for each group was 0%–30%, except for BC Sealer, which was between 40% and 50% for both the CW and SC techniques (Fig. 1A and E). NeoMTA Plus performed similarly for both obturation techniques (Fig. 1C and G) as did QuickSet2 (Fig. 1D and H). More outliers were measured for the SC technique than the CW technique at both levels and for all sealers.
Discussion
Dentin tubules are smaller at the apex and larger toward the crown (17), and the tubule diameter at the pulpal wall is variable, ranging between 2.0 and 3.2 μm (18). To achieve tubule penetration, the particle size of the material must be smaller than the tubule diameter; the larger the tubule, the deeper a particle can penetrate. Tubule penetration of retrogradely placed ProRoot MTA and Capasio has been compared via scanning electron microscopy (12). ProRoot MTA was found to have no penetration into the dentinal tubules, whereas approximately half of the Capasio samples had dentinal tubule penetration that generally increased with the distance from the resected surface (12). The particle size of Capasio is half that of ProRoot MTA, with a mean particle size of 5.3 μm. It is reasonable to assume then that because the particles for BC Sealer are <1 μm in diameter (19), they will be well suited for tubule penetration.
In the current study, the lesser penetration in the sections taken 1 mm from the apex can be attributed to smaller tubules nearer the apex, and the small particle size of BC Sealer explains why it penetrated the deepest at this level. Overall, all of the tricalcium silicate–based sealers showed greater than 80% sealer penetration circumferentially at the 5-mm level for both techniques. No differences were measured for the percent of sealer penetration for either technique at the 1-mm level for the tricalcium silicate–based sealers. However, MTA Fillapex had significantly less sealer penetration circumferentially at the 1-mm level when used with the SC technique versus the CW technique, perhaps because of its resin matrix.
NeoMTA Plus and BC Sealer had a greater percentage of sealer penetration than QuickSet2 at the 1-mm level although this was not statistically significant. This may be a reflection of the differences in their chemical composition (silicates vs aluminates) as well as the shorter working time of QuickSet2. One mixture of sealer was used to obturate all 20 canals in sequence; therefore, the QuickSet2 sealer may have started setting by the time the final roots were obturated. This may account for the outliers that had little tubule penetrance circumferentially relative to the other QuickSet2 specimens at the 5-mm level.
One difference among these sealers is that MTA Fillapex shrinks 0.7% during setting, whereas the BC Sealer expands slightly (<0.1%), which may provide superiority for the latter when used with the SC technique (20). As yet, no study has looked at the change in dimensions on setting for NeoMTA Plus or QuickSet2. BC Sealer has been indicated for use with the SC technique, which is a fast and efficient means of obturation. Other sealers have traditionally been advocated for use with a technique that allows a minimal thickness because of their high propensity to shrink and dissolution in fluids (21). The results of this study agree with the manufacturer's recommendations that MTA Fillapex performs better with the CW technique than the SC technique, with significantly higher circumferential penetration of sealer with the CW technique. Similar tubule penetration was achieved for all the other sealers with both techniques. Even though BC Sealer is recommended for use with the SC technique, it achieved greater penetration with the CW technique.
This study did not examine the interface between the gutta-percha and the dentin wall. A recent in vitro study found that MTA Plus had significantly less bond strength when used with the CW technique compared with the SC technique and primarily failed via mixed cohesive/adhesive failure. In the same study, the bond strength for BC Sealer was less when used with the CW versus the SC technique (5). Those authors attributed the differences to possible changes from the heat of the CW technique (5).
Almost all of the outliers for the percentage of sealer penetration and maximum sealer penetration were for the SC technique. This variability may be attributed to variations in the canal shape from round to oval. Celikten et al (22) found a significant difference in the number of voids between the apical and coronal thirds of canals obturated with the SC technique and attributed this to variations in root canal morphology. Some practitioners suggest using accessory cones for oval-shaped canals when using the SC technique to increase the hydraulic force in all directions to push the sealer into the tubules.
Conclusion
The tricalcium silicate–containing sealers penetrated tubules as deep as 2 mm. The percentage of sealer penetration was much higher 5 mm from the apex, with many specimens having 100% penetration for both the SC and CW techniques. MTA Fillapex, a resin-based sealer with less than 20% MTA particles, had significantly greater tubule penetration circumferentially with the CW technique versus its use with the SC technique at the 1-mm level. Within the limitations of this study, the CW and SC techniques produced similar tubule penetration at both the 1-mm and the 5-mm level with the tricalcium silicate–containing sealers BC Sealer, QuickSet2, and NeoMTA Plus.
Acknowledgments
The authors thank Connie Tillberg for her assistance in specimen preparation.
Supported by the NIH/NIDCR (grant no. R43DE020204-01A1).
Dr Primus is the owner of Primus Consulting, Bradenton, Florida, and provided the NeoMTA and QuickSet2 tested in this study. She is also the principal investigator for the grant that supported this research.
Footnotes
The authors deny any conflicts of interest related to this study.
References
- 1.Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review–part III: clinical applications, drawbacks, and mechanism of action. J Endod. 2010;36:400–13. doi: 10.1016/j.joen.2009.09.009. [DOI] [PubMed] [Google Scholar]
- 2.Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25:197–205. doi: 10.1016/S0099-2399(99)80142-3. [DOI] [PubMed] [Google Scholar]
- 3.Soheilipour E, Kheirieh S, Madani M, et al. Particle size of a new endodontic cement compared to Root MTA and calcium hydroxide. Iran Endod J. 2009;4:112–6. [PMC free article] [PubMed] [Google Scholar]
- 4.Camilleri J. Sealers and warm gutta-percha obturation techniques. J Endod. 2015;41:72–8. doi: 10.1016/j.joen.2014.06.007. [DOI] [PubMed] [Google Scholar]
- 5.DeLong C, He J, Woodmansey KF. The effect of obturation technique on the push-out bond strength of calcium silicate sealers. J Endod. 2015;41:385–8. doi: 10.1016/j.joen.2014.11.002. [DOI] [PubMed] [Google Scholar]
- 6.Candeiro GT, Correia FC, Duarte MA, et al. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J Endod. 2012;38:842–5. doi: 10.1016/j.joen.2012.02.029. [DOI] [PubMed] [Google Scholar]
- 7.De-Deus G, Brandao MC, Leal F, et al. Lack of correlation between sealer penetration into dentinal tubules and sealability in nonbonded root fillings. Int Endod J. 2012;45:642–51. doi: 10.1111/j.1365-2591.2012.02023.x. [DOI] [PubMed] [Google Scholar]
- 8.Kokkas AB, Boutsioukis A, Vassiliadis LP, Stavrianos CK. The influence of the smear layer on dentinal tubule penetration depth by three different root canal sealers: an in vitro study. J Endod. 2004;30:100–2. doi: 10.1097/00004770-200402000-00009. [DOI] [PubMed] [Google Scholar]
- 9.White RR, Goldman M, Lin PS. The influence of the smeared layer upon dentinal tubule penetration by plastic filling materials. J Endod. 1984;10:558–62. doi: 10.1016/S0099-2399(84)80100-4. [DOI] [PubMed] [Google Scholar]
- 10.Mamootil K, Messer HH. Penetration of dentinal tubules by endodontic sealer cements in extracted teeth and in vivo. Int Endod J. 2007;40:873–81. doi: 10.1111/j.1365-2591.2007.01307.x. [DOI] [PubMed] [Google Scholar]
- 11.Wang Z, Shen Y, Haapasalo M. Dentin extends the antibacterial effect of endodontic sealers against Enterococcus faecalis biofilms. J Endod. 2014;40:505–8. doi: 10.1016/j.joen.2013.10.042. [DOI] [PubMed] [Google Scholar]
- 12.Bird DC, Komabayashi T, Guo L, et al. In vitro evaluation of dentinal tubule penetration and biomineralization ability of a new root-end filling material. J Endod. 2012;38:1093–6. doi: 10.1016/j.joen.2012.04.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bolles JA, He J, Svoboda KK, et al. Comparison of Vibringe, EndoActivator, and needle irrigation on sealer penetration in extracted human teeth. J Endod. 2013;39:708–11. doi: 10.1016/j.joen.2013.01.006. [DOI] [PubMed] [Google Scholar]
- 14.De-Deus G, Gurgel Filho ED, Ferreira CM, et al. Intratubular penetration of root canal sealers. Pesqui Odontol Bras. 2002;16:332–6. doi: 10.1590/s1517-74912002000400009. [DOI] [PubMed] [Google Scholar]
- 15.Kara Tuncer A, Unal B. Comparison of sealer penetration using the EndoVac irrigation system and conventional needle root canal irrigation. J Endod. 2014;40:613–7. doi: 10.1016/j.joen.2013.11.017. [DOI] [PubMed] [Google Scholar]
- 16.Kouvas V, Liolios E, Vassiliadis L, et al. Influence of smear layer on depth of penetration of three endodontic sealers: an SEM study. Endod Dent Traumatol. 1998;14:191–5. doi: 10.1111/j.1600-9657.1998.tb00836.x. [DOI] [PubMed] [Google Scholar]
- 17.Garberoglio R, Brannstrom M. Scanning electron microscopic investigation of human dentinal tubules. Arch Oral Biol. 1976;21:355–62. doi: 10.1016/s0003-9969(76)80003-9. [DOI] [PubMed] [Google Scholar]
- 18.Cleghorn BM, Goodacre CJ, Christie WH. Morphology of teeth and their root canal systems. In: Ingle JI, Bakland LK, Baumgartner JC, editors. Ingle's Endodontics. 6th. Hamilton, ON: PMPH USA, Ltd; 2008. pp. 151–221. [Google Scholar]
- 19.Camilleri J. Mineral Trioxide Aggregate in Dentistry: From Preparation to Application. 1st. Berlin: Springer-Verlag; 2014. [Google Scholar]
- 20.Zhou HM, Shen Y, Zheng W et al. Physical properties of 5 root canal sealers. J Endod. 2013;39:1281–6. doi: 10.1016/j.joen.2013.06.012. [DOI] [PubMed] [Google Scholar]
- 21.Kontakiotis EG, Wu MK, Wesselink PR. Effect of sealer thickness on long-term sealing ability: a 2-year follow-up study. Int Endod J. 1997;30:307–12. doi: 10.1046/j.1365-2591.1997.00087.x. [DOI] [PubMed] [Google Scholar]
- 22.Celikten B, Uzuntas CF, Orhan AI, et al. Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: an in vitro micro-CT study. Scanning. 2015 Jul 30; doi: 10.1002/sca.21249. http://dx.doi.org/10.1002/sca.21249 [Epub ahead of print] [DOI] [PubMed]