

Abstract
Objectives
Death from injury is frequently preventable, but injury remains a leading cause of death in the USA. While evidence-based strategies exist to prevent many types of injuries, effective policies for implementing these strategies at the population level are needed to reduce injury deaths. We identified promising injury prevention policies and evaluated their association with injury death rate (IDR).
Methods
We identified 11 injury prevention policies and accessed data on 2013 state and county IDRs. States were divided into strong, moderate and weak tertiles based on total number of policies in place. Adjusted regression modelling compared the strength of state prevention policies with IDRs at the state level and then at the county level to account for variability within states.
Results
The strength of state prevention policies (tertile) was not significantly associated with IDR in US states. However, counties in strong policy states had a 11.8-point lower IDR compared with those in weak policy states (p=0.001).
Conclusions
States with more injury prevention policies in place have lower rates of death from injury, particularly when evaluated at the county level. Implementing recommended prevention policies holds potential to prevent injury death in the USA.
BACKGROUND
Whether they stem from incident or violence, most injuries are predictable and preventable, and preventing injuries and promoting safety is a core goal of public health. Scientific evidence supports many injury prevention strategies (eg, helmets for cyclists), but the government policies that aim to apply these strategies (ie, laws requiring cyclists to wear helmets) may or may not bring the full benefit of the initial strategy to the whole population. In some cases, these laws may have unintended consequences that reverse the desired effect. Clear evidence that injury prevention policies work is rare, and this lack is a key barrier to wide adoption of these policies.1 We aimed to clarify the relationship between promising injury prevention policies and death from injury at the population level in the setting of real-world implementation and enforcement.
While it would be impossible to measure the myriad injury prevention policies that states could implement, we assessed a sample of policies covering important areas of injury prevention. We evaluated 10 state injury prevention policies highlighted by the Trust for America’s Health in consultation with injury prevention experts in the areas of traffic safety, youth safety, intimate partner violence (IPV) and injury data collection.1 Because gun deaths make up a large proportion of violent injury deaths in the USA, and because gun regulations vary widely among states, we incorporated a summary measure of 25 gun regulations published annually by The Law Center to Prevent Gun Violence, a national organisation that tracks gun laws in every state.2
In addition to covering important areas of injury prevention, we chose to evaluate these policies for three reasons. These policies are promising, but as yet unproven, and are therefore ripe for evaluation. They have proven feasibility, as at least some states have implemented each policy. Lastly, these policies exhibit substantial variability between states, allowing us to make meaningful comparisons. Because each policy has focused aims targeting specific populations, the impact of each policy on the overall injury death rate (IDR) may be so small as to be undetectable. We, therefore, also evaluated a cumulative policy measure derived by summing the policies together.
This paper presents an investigation into 11 state injury prevention policies and IDRs in the USA. Although we expect state policies to have an overall impact on their populations, all states are relatively large and demographically heterogeneous, which may make real differences difficult to discern. Comparing county-level IDRs across states allowed us to assess the impact of state policies on counties with similar demographic and environmental risk factors.
METHODS
Setting, population and study design
We conducted a cross-sectional, ecologic study of injury death in the 50 states of the USA and their county subdivisions. The primary outcomes were state and county IDRs in 2013, and the primary predictors of interest were state injury prevention policies in place in 2013.
Sociodemographic factors that differ among states and counties may affect individuals’ risk of injury and injury death and also a state’s likelihood of adopting injury prevention policies. We, therefore, attempted to balance the effects of sociodemographic variables by including them as confounders in our multivariable regression model. State demographics were included as covariates in the state-level analysis, and county demographics were included in the county-level analysis. Drawing on Haddon’s Injury Matrix,3 we expect the injury prevention policies to act in the pre-event phase on the host (by disincentivising risky behaviour) and on the agent (eg, by making cars and bicycles safer). We also expect some policies to act in the event phase, reducing injuries from a motorcycle crash or a sports concussion.
Sources of injury and demographic data
We collected IDRs for 2013 from the CDC, the agency responsible for monitoring disease and injury in the USA.4 In accordance with CDC policy, counties reporting <10 injury deaths were excluded from analysis.4 We collected state-level and county-level demographics and health factors from the US Census Bureau, the agency which surveys the entire population every decade and subsets of the population annually,5 and the 2013 Robert Wood Johnson Foundation County Health Rankings, which compile state-level and county-level data on health outcomes, behaviours, clinical care and social and economic factors.6 We used the most recent data available prior to 2013, including 2010 census measures when no more recent data were available. We incorporated US Department of Agriculture 2013 rural–urban continuum codes to account for gradations of rurality among counties.7 This study was deemed exempt from review by the University of Pennsylvania Institutional Review Board.
Injury prevention policies
We evaluated 10 injury prevention policies highlighted by the Trust for America’s Health in consultation with injury prevention experts,1 and a summary measure of 25 gun regulations published annually by the Law Center to Prevent Gun Violence.2 Taken together, these policies cover important areas of injury prevention; are promising but unproven; are feasible for states to implement and exhibit variability across states. The policies we studied are as follows.
Primary seat belt enforcement
Seat belt use is required in every US state except New Hampshire, and seat belts save 12 000 lives each year in the USA.8 With primary enforcement laws, police may stop and ticket drivers for seat belt violations alone. In Florida, seat belt use increased 7% after the switch to primary enforcement.9
Ignition interlock requirement for drunk driving
Alcohol-impaired drivers are involved in 11 000 deaths each year in the USA.1,10 Ignition interlock devices reduce drunk driving recidivism by at least 66%,11,12 but the impact on injury and death is unknown.13
Motorcycle helmet requirement
Per mile travelled, motorcyclists are at 26 times more likely to die in a crash than car occupants,14 and motorcycle helmets reduce this risk by 37%.15 Motorcycle fatalities are 11% lower in the 19 states with helmet laws, but many states repealed their requirements after federal penalties were lifted in 1976 and 1995.15
Booster seat requirement for children under age 8
MVCs are the leading cause of death for children aged 4–8, and booster seats reduce risk of serious injury by 45%.16 One study found that states with booster seat laws had a 25% fewer fatalities in the target age group.17
Bicycle helmet requirement for children
Helmets reduce head injuries by 88% for bicyclists.18 Helmet laws are effective in encouraging helmet use and reducing head injury among children.19
Access to orders of protection for IPV in dating relationships
IPV affects one in three women and one in four men in the USA and causes more than 2000 deaths annually. Court protective orders can decrease violence by up to 60%,20 but are not always available to unmarried people.
Access to orders of protection for teen dating violence
IPV also affects about one in four youth as well, but access to orders of protection is often restricted for teenagers. Comprehensive access is available in only a few states, according to a scoring system that incorporates several facets of access.21
Strict youth sports concussion laws
Repeated head injury poses the greatest risk of severe injury or death after concussion, and policies aimed at preventing youth from playing risky sports after a concussion are growing in the USA. Strict policies require education for youth and parents, removing injured athletes from play and clearance from a health professional before an athlete returns to play.1 These laws are associated with increased healthcare usage, but the effect on injuries is unclear.22
Prescription drug monitoring programmes
Prescription drug abuse has increased over the last two decades, leading to 15 000 overdose deaths per year in the USA.23 To limit the overuse of prescription drugs, many states have implemented monitoring programmes that require clinicians to check a registry for each patient before prescribing a controlled substance, but evidence to support these policies is mixed.24
External cause-of-injury coding
Effective injury prevention requires an understanding of the incidence and outcomes of injuries. Clinicians can record this information using external cause-of-injury codes (E-codes), but this crucial information is often incomplete, with only 23 states meeting the goal of 90% reporting of E-codes.1,25
Gun regulations
States were considered to have strict gun laws if they received a grade of B- or better from the Law Center to Prevent Gun Violence. This summary measure incorporates 25 separate policies that regulate purchase, storage and carrying of guns.2 While there is evidence that certain policies can restrict access to guns,26 literature relating these laws to gun injuries remains limited.27
Statistical analysis
We estimated the impact of individual injury policies on IDR at the state and county level. Given that each policy has the potential to prevent deaths in a narrow population or caused by a particular mechanism, the impact of each policy on the overall IDR might be so small as to be unappreciable, we therefore summed the total number of policies at the state level to estimate their summed impact. We assessed the association of policy total with IDR. The number of policies was totalled for each state, and states were divided into tertiles of policy total, as shown in figure 1. We analysed data at the county level as well as the state level in order to better adjust for the diversity of risk factors distributed unevenly among counties.
Figure 1.
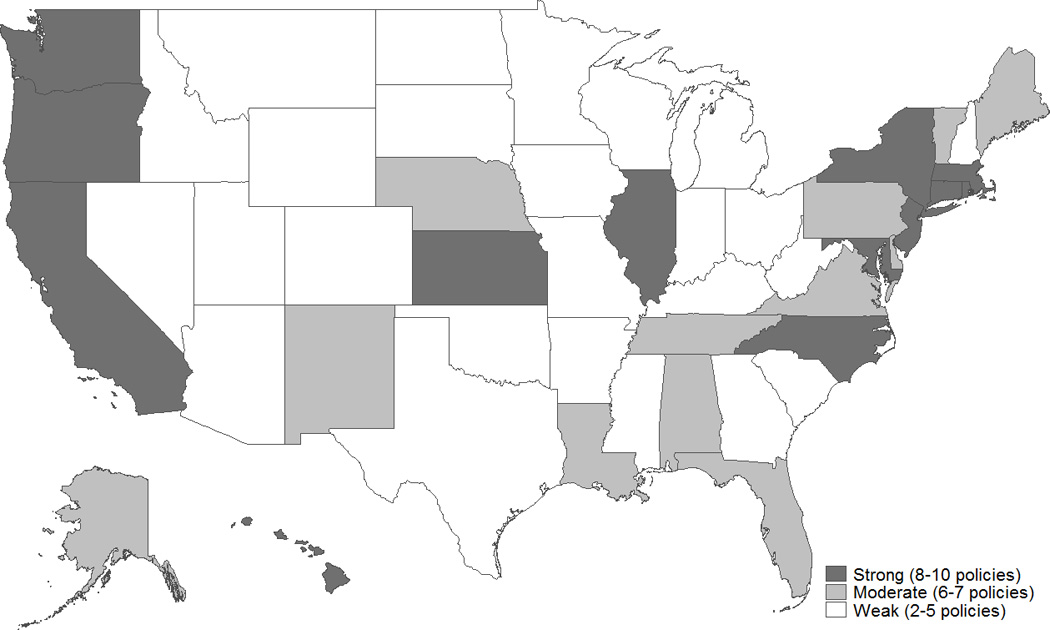
Map of state policy tertiles.
The relationship between policy tertiles and IDRs was first estimated using ordinary least squares regression at the state level. We used a random effects model to perform the county-level analysis, with state policy tertile as the primary predictor and county sociodemographic variables as covariates. The random effects model allowed us to incorporate state characteristics (the policies and tertiles) along with county characteristics. Because county observations within the same state are not independent, we adjusted the SEs by the 50 state clusters.28 To confirm the analysis, data were examined using generalised estimating equations with robust SEs and with generalised linear mixed models, yielding nearly identical results. Because most of the policies evaluated here related to unintentional injury, we conducted a sensitivity analysis limiting the outcome to unintentional injury to check the robustness of our analysis. We used Stata for all analyses (Stata 2013).
RESULTS
The IDR for the USA was 62 per 100 000 people in 2013. State-wide IDRs ranged from 44 to 101 per 100 000. Among counties, the range was 24–351. The range of IDRs among counties within a single state varied from 2 to 299 per 100 000. States were divided into tertiles of policy total. States in the weak policy tertile had a mean of four policies, compared with six in moderate policy states and eight in strong policy states (table 1).
Table 1.
State and county characteristics by policy tertile
| Policy frequency | ||||
|---|---|---|---|---|
| Weak | Moderate | Strong | p Value* | |
| Frequency of injury prevention policies | N=25 | N=12 | N=13 | |
| Primary seat belt enforcement | 11 (44%) | 9 (75%) | 12 (92%) | 0.009 |
| Ignition interlock requirement for drunk driving | 4 (16%) | 5 (42%) | 7 (54%) | 0.043 |
| Motorcycle helmet requirement | 5 (20%) | 6 (50%) | 8 (62%) | 0.027 |
| Booster seat requirement for children under age 8 | 12 (48%) | 8 (67%) | 12 (92%) | 0.026 |
| Bicycle helmet requirement for children | 3 (12%) | 8 (67%) | 11 (85%) | <0.001 |
| Access to orders of protection for IPV in dating relationships | 19 (76%) | 12 (100%) | 13 (100%) | 0.033 |
| Access to orders of protection for teen dating violence | 2 (8%) | 0 (0%) | 4 (31%) | 0.042 |
| Strict youth sports concussion laws | 16 (64%) | 11 (92%) | 13 (100%) | 0.016 |
| Prescription drug monitoring programme | 20 (80%) | 12 (100%) | 12 (92%) | 0.185 |
| External cause-of-injury coding | 9 (36%) | 5 (42%) | 9 (69%) | 0.141 |
| Strict gun regulations | 0 (0%) | 1 (8%) | 9 (69%) | <0.001 |
| State characteristics | ||||
| Median household income ($) | 47646 | 48844 | 55131 | 0.0006 |
| Rural population (%) | 30.5 | 31.6 | 13.8 | 0.0006 |
| White population (%) | 76.6 | 68.8 | 64.4 | 0.0095 |
| Population with some college education (%) | 62.9 | 61.6 | 66.1 | 0.0006 |
| Uninsured population (%) | 17.1 | 16.2 | 13.7 | 0.0599 |
| Unemployed population (%) | 7.1 | 6.8 | 8.3 | 0.0511 |
| Population <18 years (%) | 24.0 | 22.8 | 22.7 | 0.0544 |
| Population ≥65 years (%) | 13.9 | 14.5 | 14.0 | 0.6069 |
| Per cent of MVCs involving alcohol | 32.7 | 33.5 | 34.0 | 0.8206 |
| County characteristics | N=1340 | N=519 | N=466 | |
| Median household income ($) | 44118 | 44615 | 50643 | <0.0001 |
| Rural counties (%) | 61.6 | 47.0 | 43.1 | <0.0001 |
| White population (%) | 79.0 | 74.7 | 75.1 | <0.0001 |
| Population with some college education (%) | 54.5 | 52.6 | 60.2 | <0.0001 |
| Uninsured population (%) | 18.4 | 17.4 | 15.3 | <0.0001 |
| Unemployed population (%) | 7.9 | 7.7 | 9.2 | <0.0001 |
| Population <18 years (%) | 23.6 | 22.3 | 22.4 | <0.0001 |
| Population ≥65 years (%) | 15.7 | 16.4 | 16.0 | 0.0067 |
| Per cent of MVCs involving alcohol | 30.7 | 33.4 | 32.9 | <0.0001 |
χ2 test was used for categorical variables; analysis of variance was used for continuous variables. IPV, intimate partner violence.
State-level analysis
State-level adjusted and unadjusted IDRs are summarised in table 2. In unadjusted analysis, each additional point of policy total (ie, each additional policy) was associated with a 3.1-point lower IDR on average (95% CI −4.6 to −1.6; p<0.001). After adjusting for state demographics, each additional policy was associated with a 0.9-point lower IDR (95% CI −2.5 to 0.8; p=0.279) In unadjusted analysis, the IDR was 57 per 100 000 population in strong policy states, 72 in moderate policy states and 73 in weak policy states (p=0.0001). After adjusting for state-level demographics, moderate policy states had a 0.8-point lower IDR and strong policy states had a 4.0-point lower IDR compared with weak policy states, but this difference was not statistically significant. The four policies with a statistically significant association with IDRs in unadjusted analysis were the booster seat requirement, strict youth concussion law, the data reporting metric and strict gun regulations. No policy was associated with a statistically significant difference in IDR after adjustment nor was any demographic factor.
Table 2.
State-level regression analysis
| Unadjusted | Adjusted | |||||
|---|---|---|---|---|---|---|
| Coefficient | 95% CI | p Value | Coefficie | 95% CI | p Value | |
| Injury prevention policies | ||||||
| Primary seat belt enforcement | −4.2 | −11.5 to 3.2 | 0.261 | −3.5 | −9.6 to 2.5 | 0.247 |
| Ignition interlock requirement for drunk driving | −4.3 | −11.9 to 4.6 | 0.256 | 1.4 | −4.4 to 7.2 | 0.631 |
| Motorcycle helmet requirement | −5.0 | −12.2 to 2.3 | 0.172 | −3.3 | −9.1 to 2.5 | 0.255 |
| Booster seat requirement for children under age 8 | −8.4 | −15.4 to −1.3 | 0.021 | −0.4 | −6.8 to 6.0 | 0.901 |
| Bicycle helmet requirement for children | −5.1 | −12.2 to 2.0 | 0.152 | −0.6 | −6.8 to 5.7 | 0.851 |
| Access to orders of protection for IPV in dating relationships | −0.9 | −11.9 to 0.1 | 0.865 | 3.3 | −4.8 to 11.4 | 0.416 |
| Access to orders of protection for teen dating violence | −4.8 | −15.7 to 6.1 | 0.382 | −2.4 | −10.5 to 5.7 | 0.554 |
| Strict youth sports concussion laws | −10.2 | −18.7 to −1.8 | 0.019 | −2.3 | −9.0 to 4.4 | 0.486 |
| Prescription drug monitoring programme | 2.3 | −8.7 to 13.3 | 0.675 | 3.9 | −3.6 to 11.4 | 0.302 |
| External cause-of-injury coding | −7.8 | −14.7 to −1.0 | 0.025 | −2.3 | −7.7 to 3.1 | 0.396 |
| Strict gun regulations | −17.9 | −25.2 to −10.6 | <0.001 | −2.8 | −13.4 to 7.8 | 0.600 |
| Weak | 0 | ref | 0 | ref | ||
| Moderate | −0.7 | −8.1 to 6.7 | 0.844 | −0.8 | −7.4 to 5.9 | 0.822 |
| Strong | −16.2 | −23.4 to −9.0 | <0.001 | −4.0 | −12.4 to 4.3 | 0.337 |
| State characteristics | ||||||
| Median household income (z score) | −7.0 | −10.0 to −4.0 | <0.0001 | 0.1 | −4.3 to 4.6 | 0.950 |
| Rural population (%) | 0.5 | 0.3 to 0.7 | <0.0001 | 0.3 | 0.0 to 0.6 | 0.055 |
| White population (%) | 0.2 | 0.0 to 0.4 | 0.075 | 0.2 | −0.1 to 0.4 | 0.163 |
| Population with some college education (%) | −1.2 | −1.8 to −0.5 | 0.001 | −0.8 | −1.7 to 0.1 | 0.071 |
| Uninsured population (%) | 1.0 | 0.3 to 1.8 | 0.005 | 0.7 | −0.2 to 1.6 | 0.107 |
| Unemployed population (%) | −1.1 | −3.2 to 1.0 | 0.289 | −0.6 | −3.1 to 1.8 | 0.617 |
| Population <18 years (%) | 0.1 | −2.0 to 1.8 | 0.945 | 0.4 | −2.5 to 3.4 | 0.772 |
| Population ≥65 years (%) | 1.4 | −0.7 to 3.5 | 0.196 | 0.9 | −2.1 to 4.0 | 0.533 |
| Per cent of MVCs involving alcohol | 0.3 | −0.3 to 0.88 | 0.333 | 0.4 | −0.1 to 0.9 | 0.089 |
Policy coefficients are adjusted for state characteristics. Adjusted coefficients for each state characteristic are drawn from the model using policy tertiles.
IPV, intimate partner violence.
County-level analysis
Counties reporting <10 injury deaths for the year were excluded from analysis as required by the CDC.4 These 815 counties are home to 1.9% of the US population, leaving 2325 counties for analysis. Adjusting for state clustering but not for county-level risk factors, each additional policy was associated with a 3.9-point lower IDR (95% CI −5.8 to −2.0; p<0.001). Counties in moderate policy states had a 1.2-point lower IDR and counties in strong policy states had a 19.3-point lower IDR on average than low policy states (p=0.810 and p<0.001, respectively; table 3). After adjusting for county-level demographics and prevalence of alcohol use, each additional policy was associated with a 2.6-point lower in IDR (95% CI −4.5 to −0.7; p=0.008), and counties in moderate policy states had a 0.5-point lower IDR and counties in strong policy states had an 11.8-point lower IDR on average than low policy states (p=0.936 and 0.001, respectively). Although we hypothesised that high-risk counties, including low income and rural counties, would benefit disproportionately, no significant interaction was found between county income or rurality and policy tertile.
Table 3.
County-level regression analysis
| Unadjusted | Adjusted* | |||||
|---|---|---|---|---|---|---|
| Coefficie | 95% CI | p Value | Coefficient | 95% CI | p Value | |
| Injury prevention policies | ||||||
| Primary seat belt enforcement | −9.2 | −18.4 to 0.0 | 0.050 | −10.9 | −18.6 to −3.1 | 0.006 |
| Ignition interlock requirement for drunk driving | 1.5 | −8.5 to 11.5 | 0.769 | 3.9 | −5.5 to 13.3 | 0.412 |
| Motorcycle helmet requirement | −7.7 | −16.2 to 0.9 | 0.078 | −7.0 | −14.0 to 0.1 | 0.052 |
| Booster seat requirement for children under age 8 | −12.8 | −21.1 to −4.4 | 0.003 | −9.4 | −17.4 to −1.3 | 0.022 |
| Bicycle helmet requirement for children | −11.7 | −20.1 to −3.3 | 0.007 | −8.5 | −15.3 to −1.8 | 0.013 |
| Access to orders of protection for IPV in dating | −6.0 | −19.7 to 7.8 | 0.395 | −2.8 | −17.5 to 11.9 | 0.709 |
| Access to orders of protection for teen dating | −2.6 | −14.7 to 9.5 | 0.669 | −0.5 | −11.5 to 10.5 | 0.934 |
| Strict youth sports concussion laws | −4.8 | −15.5 to 6.0 | 0.384 | −0.6 | −9.4 to 10.6 | 0.907 |
| Prescription drug monitoring programme | 5.7 | −2.8 to 14.3 | 0.189 | 6.2 | 1.4 to 10.9 | 0.011 |
| External cause-of-injury coding | −8.0 | −16.5 to 0.5 | 0.066 | −5.8 | −12.9 to 1.4 | 0.113 |
| Strict gun regulations | −23.9 | −31.3 to 16.4 | <0.001 | −12.6 | −19.2 to −6.0 | <0.001 |
| Weak | 0 | ref | 0 | ref | ||
| Moderate | −1.2 | 11.1 to 8.8 | 0.819 | −0.5 | −12.0 to 11.1 | 0.936 |
| Strong | −19.3 | −27.6 to −11.0 | <0.001 | −11.8 | −18.6 to −5.0 | 0.001 |
| County characteristics | ||||||
| Median household income (z score) | −12.9 | −15.0 to −10.9 | <0.001 | −5.9 | −8.4 to −3.5 | <0.001 |
| Rural county | 22.3 | 18.6 to 26.0 | <0.001 | 5.6 | 2.2 to 9.1 | 0.001 |
| White population (%) | 0.1 | −0.1 to 0.3 | 0.248 | 0.1 | 0.0 to 0.2 | 0.184 |
| Population with some college education (%) | −1.0 | −1.2 to −0.8 | <0.001 | −0.2 | −0.4 to 0.0 | 0.038 |
| Uninsured population (%) | 1.4 | 0.5 to 2.4 | 0.003 | −0.1 | −0.6 to 0.4 | 0.709 |
| Unemployed population (%) | 1.9 | 0.5 to 3.2 | 0.008 | 1.1 | 0.0 to 2.2 | 0.045 |
| Population <18 years (%) | −0.5 | −1.6 to 0.6 | 0.359 | 1.1 | 0.3 to 2.0 | 0.010 |
| Population ≥65 years (%) | 2.7 | 2.0 to 3.4 | <0.001 | 2.4 | 1.7 to 3.1 | <0.001 |
| Per cent of MVCs involving alcohol | 0.2 | 0.0 to 0.4 | 0.041 | 0.2 | 0.1 to 0.3 | 0.003 |
Policy coefficients are adjusted for county characteristics. Adjusted coefficients for each county characteristic are drawn from the model using policy tertiles.
IPV, intimate partner violence.
The results of a sensitivity analysis limiting the outcome to unintentional injury were very similar at the state and county levels to those reported here, and are excluded for brevity. An additional 288 counties were excluded from this analysis due to unintentional injury counts of <10. A sensitivity analysis excluding policies with low variation: the youth concussion policy, the teen dating policy and the prescription drug monitoring programme policy yielded similar results.
DISCUSSION
States with a greater policy presence regarding injury prevention had lower rates of death from injury. The results of the state-level analysis were small and did not achieve statistical significance. The county-level analysis allowed for more nuance, enabling a more precise adjustment and comparison, and revealed larger, statistically significant effects. When we examined county-level IDRs and adjusted for county-level risk factors, we found that counties located in strong policy states had lower rates of death from injury than counties in moderate or weak policy states.
While many injury prevention strategies are based on scientific evidence, from wearing a seat belt while driving to staying out of the game after a sports concussion, the policies that states can use to attempt to apply these strategies to their populations are themselves largely unproven. Well-intentioned policies may have minimal or even adverse consequences depending on dissemination, enforcement and unintended consequences.29
Our results represent the real-world implementation of these policies, not the ideal or maximum effect of the injury prevention strategies that the policies promote. Likewise, these results represent the association of these policies with the most severe outcome, injury death and not the more common outcome of nonfatal injuries or the total impact on the population. Given that each policy addresses only one aspect of injury prevention and often has a narrow target population, we might expect that the impact of any individual policy would be obscured at the level of the overall IDR. We, therefore, summed the policies together to assess their cumulative impact. While we cannot recommend that states adopt any one of these policies over another, therefore, we believe our findings support both this suite of policies and states’ continuing efforts to use policy mechanisms to reduce death from injury.
We recognise several limitations in our approach. We cannot establish a causal relationship between policy implementation and reduction in deaths. It is possible that the policies we studied are a proxy for other state policies or that represent a picture of a state safety culture, which is at the root of both policy implementation and lower IDRs. We cannot ensure against reverse causality, as in some cases, states may have enacted policies in response to particular local challenges. This dynamic may explain the positive association seen between prescription drug monitoring programmes and IDR. We evaluated a set of policies recommended by an assembly of experts drawing on scientific evidence in important areas of injury prevention, but the list is necessarily incomplete. Other, more effective, policies may exist. We evaluated the impact of state policies on states and counties, but could not account for local laws, which may affect county outcomes, or for differences in enforcement between or within states. In particular, low-income counties may have fewer resources for enforcement, and rural counties may experience special enforcement challenges due to low population density. These factors could have attenuated the increased effect we expected to see in these high-risk counties. Lastly, in this cross-sectional study, we cannot assess effect of time on policy impact. Policy implementation may be followed by a diffusion period and a time lag to maximum impact, reducing the apparent impact of recently implemented policies. Conversely, initial enthusiasm about a new policy may wane over time, leading to diminished enforcement and impact. In addition, coming policies may be known in advance, leading to anticipatory effects. These aspects of injury prevention policies deserve further, rigorous study to enable truly effective, evidence-based policy making.
CONCLUSIONS
States with more injury prevention policies in place have lower rates of death from injury, particularly when evaluated at the county level. State legislators can use policy to prevent injury in their states. The policies examined here deserve further consideration in those states that have not yet implemented them. Further studies of injury prevention should continue to investigate strategies to prevent injury at the individual level and aim to identify the policies that can most effectively deploy these strategies to the population.
What is already known on the subject
-
▸
Injury remains a leading cause of death in the USA.
-
▸
State injury prevention policies have the potential to reduce risk of injury and death for large populations.
-
▸
Individual state policies are based on varying levels of evidence, and evaluation of policy impact remains challenging.
What this study adds
Increased numbers of state injury policies are associated with lower rates of death from injury at the county level.
Acknowledgments
The authors thank Laura Cutilletta of the Law Center to Prevent Gun Violence for assistance in obtaining and interpreting state gun regulation data.
Footnotes
Contributors: EJK and DJW jointly designed the study. EJK was primarily responsible for data acquisition and analysis with input from DJW. EJK drafted the manuscript. Both authors contributed critical revision of the manuscript and approved the final version.
Competing interests: None declared.
Ethics approval: This study was deemed exempt from review by the University of Pennsylvania Institutional Review Board.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: This study was conducted using publicly available data, which are accessible to all interested parties.
REFERENCES
- 1.Trust for America’s Health, Robert Wood Johnson Foundation. The facts hurt: a state-by-state injury prevention policy report. Washington DC: 2013. [Google Scholar]
- 2.Law Center to Prevent Gun Violence. Scorecard: Why Gun Laws Matter; 2013. [accessed 25 Sep 2015]. http://gunlawscorecard.org. [Google Scholar]
- 3.Haddon W. Advances in the epidemiology of injuries as a basis for public policy. Public Health Reports. 1980;95:411–421. [PMC free article] [PubMed] [Google Scholar]
- 4.US Centers for Disease Control and Prevention. Compressed Mortality File 1999– 2013 on CDC WONDER Online Database, released October 2014. [accessed 2 Apr 2015]; http://wonder.cdc.gov/cmf-icd10.html.
- 5.United States Census Bureau. [accessed 9 Feb 2015]; http://www.census.gov.
- 6.County health rankings and roadmaps: building a culture of health, county by county. A Robert Wood Johnson Foundation program. [accessed 8 Feb 2015]; http://www.countyhealthrankings.org. [Google Scholar]
- 7.US Department of Agriculture. Rural-urban continuum codes. [accessed 9 Feb 2015]; http://www.ers.usda.gov/data-products/rural-urban-continuum-codes/.aspx.
- 8.US Department of Transportation National Highway Traffic Safety Administration. Crash Stats: lives saved in 2012 by restraint use and minimum drinking age laws. Washington DC: National Highway Traffic Safety Administration Center for Statistics and Analysis; 2013. DOT HS 811 851. [Google Scholar]
- 9.Kahn CA. National Highway Traffic Safety Administration. Impact of implementing a primary seat belt enforcement law in Florida: a case study. Ann Emerg Med. 2013;62:182–183. [Google Scholar]
- 10.US Centers for Disease Control and Prevention. Vital signs: alcohol-impaired driving among adults— United States, 2010. MMWR. 2011;60:1351–1356. [PubMed] [Google Scholar]
- 11.Bjerre B. Primary and secondary prevention of drink driving by the use of alcolock device and program: Swedish experiences. Accid Anal Prev. 2005;37:1145–1152. doi: 10.1016/j.aap.2005.06.020. [DOI] [PubMed] [Google Scholar]
- 12.Willis C, Lybrand S, Bellamy N. Alcohol ignition interlock programmes for reducing drink driving recidivism. Cochrane Database Syst Rev. 2004;(4):CD004168. doi: 10.1002/14651858.CD004168.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Elder RW, Voas R, Beirness D, et al. Effectiveness of Ignition interlocks for preventing alcohol-impaired driving and alcohol-related crashes: a community guide systematic review. Am J Prev Med. 2011;40:362. doi: 10.1016/j.amepre.2010.11.012. [DOI] [PubMed] [Google Scholar]
- 14.US Department of Transportation National Highway Traffic Safety Administration. 2012 Data: motorcycles. Washington DC: National Highway Traffic Safety Administration Center for Statistics and Analysis; 2014. DOT HS 812 035. [Google Scholar]
- 15.Houston DJ, Richardson LE., Jr Motorcycle safety and the repeal of universal helmet laws. AJPH. 2007;97:2063–2069. doi: 10.2105/AJPH.2006.094615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Arbogast KB, Jermakian JS, Kallan MJ, et al. Effectiveness of belt positioning booster seats: an updated assessment. Pediatrics. 2009;124:1281–1286. doi: 10.1542/peds.2009-0908. [DOI] [PubMed] [Google Scholar]
- 17.Mannix R, Fleegler E, Meehan WP, et al. Booster seat laws and fatalities in children 4 to 7 years of age. Pediatrics. 2012;130:996–1002. doi: 10.1542/peds.2012-1058. [DOI] [PubMed] [Google Scholar]
- 18.Thompson DC, Rivara FP, Thompson R. Helmets for preventing head and facial injuries in bicycling. Cochrane Database Syst Rev. 2000;(2):CD001855. doi: 10.1002/14651858.CD001855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Macpherson A, Spinks A. Bicycle helmet legislation for the uptake of helmet use and prevention of head injuries. Cochrane Database Syst Rev. 2008;(3):CD005401. doi: 10.1002/14651858.CD005401.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Holt VL, Kernic MA, Wolf ME, et al. Do protection orders affect the likelihood of future partner violence and injury? Am J Prev Med. 2003;24:16–21. doi: 10.1016/s0749-3797(02)00576-7. [DOI] [PubMed] [Google Scholar]
- 21.Break the Cycle. 2010 State Law Report Cards: a National Survey of Teen Dating Violence Laws. Los Angeles, CA: Break the Cycle; 2010. [accessed Feb 2015]. http://www.breakthecycle.org/state-law-report-cards. [Google Scholar]
- 22.Gibson TB, Herring SA, Kutcher JS, et al. Analyzing the effect of state legislation on health care utilization for children with concussion. JAMA Pediatr. 2015;169:163–168. doi: 10.1001/jamapediatrics.2014.2320. [DOI] [PubMed] [Google Scholar]
- 23.Centers for Disease Control and Prevention (CDC) Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60:1487–1492. [PubMed] [Google Scholar]
- 24.Paulozzi LJ, Kilbourne EM, Desai HA. Prescription drug monitoring programs and death rates from drug overdose. Pain Med. 2011;12:747–754. doi: 10.1111/j.1526-4637.2011.01062.x. [DOI] [PubMed] [Google Scholar]
- 25.National Center for Injury Prevention and Control. Recommended actions to improve external-cause-of-injury coding in state-based hospital discharge and emergency department data systems. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2009. [Google Scholar]
- 26.Vernick JS. Policies to prevent firearm trafficking. Inj Prev. 2007;13:78. doi: 10.1136/ip.2007.015487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hahn RA, Bilukha O, Crosby A, et al. Firearms laws and the reduction of violence: a systematic review. Am J Prev Med. 2005;28:40–71. doi: 10.1016/j.amepre.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 28.Wears RL. Advanced statistics: statistical methods for analyzing cluster and cluster-randomized data. Acad Emerg Med. 2002;9:330–340. doi: 10.1111/j.1553-2712.2002.tb01332.x. [DOI] [PubMed] [Google Scholar]
- 29.Carpenter CS, Stehr M. Intended and unintended consequences of youth bicycle helmet laws. J Law Econ. 2011;54:305. [Google Scholar]