

Sir,
A 23-year-old man presented with mildly pruritic, small erythematous papules mainly on the face, neck, and trunk. The lesions first appeared on the forehead five years back and progressed to involve other areas of the body. There was no history of prolonged drug intake and family history was noncontributory. On examination, multiple skin-colored to erythematous nonfollicular and follicular papules were seen on the face, neck, and trunk regions [Figures 1–3]. The differential diagnoses of eruptive syringoma, acneiform eruption, and sebaceous hyperplasia were considered. Skin biopsy was done from a lesion on the upper chest. Histopathologic examination revealed mature sweat ducts lined by two layers of cuboidal cells and few having an epithelial elongation of the ducts, the so-called “tadpole” appearance [Figure 4]. Consequently, a diagnosis of generalized eruptive syringoma was made. The patient was started on oral isotretinoin (20 mg/day).
Figure 1.

Multiple skin-colored follicular and nonfollicular papules
Figure 3.

Close-up view of the erythematous papules
Figure 4.
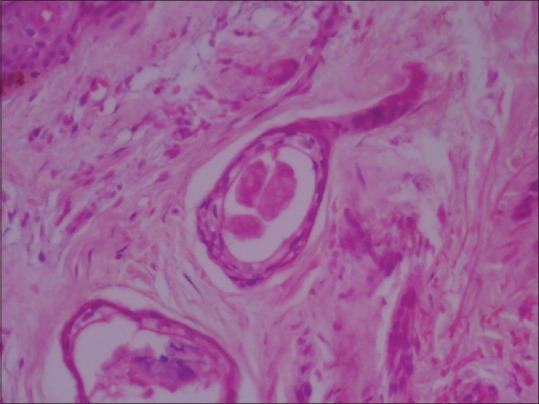
Sweat duct lined by two layers of cuboidal cells and having an epithelial elongation of the ducts, the so-called tadpole appearance (H and E, ×40)
Figure 2.

Multiple papules on the neck and upper chest
First described by Kaposi,[1] syringomas are benign tumors derived from intraepidermal portion of the eccrine sweat ducts.[1,2] Generalized eruptive syringoma is a rare entity and is seen in women mainly during puberty or later. Jacquet and Darier in 1987 first described this variant. Friedman and Butler classified four principal clinical variants of syringoma: A localized form, a familial form, a form associated with Down syndrome, and a generalized form that encompasses multiple and eruptive syringomas.[3] Although several theories have been proposed, the pathogenesis of eruptive syringoma still remains unclear. They usually appear as multiple skin-colored, yellow, brown or pink papules ranging from 1 to 3 mm in size. Most commonly seen on the eyelid and upper cheek, but in the eruptive variant they can appear on axilla, trunk, and genital areas. Some authors have reported the occurrence of syringomas after waxing in the pubic areas. Familial cases of syringomas are also seen. Differential diagnosis includes acneiform eruptions, sebaceous hyperplasia, hidrocystoma, eruptive xanthomas. Histopathological findings are distinct and confirmatory. Treatment is often unsatisfactory; electrodessication, dermabrasion, CO2 laser, topical adapalene, topical tretinoin, and oral retionoids have been used with varied success. Very rarely, tumors may regress later in life. Itchy eruptive syringomas have been reported from India by Verma et al.[4] We report a case of mildly pruritic generalized eruptive syringoma in a 23-year-old man, which could be misdiagnosed as acneiform eruption. Hence eruptive syringoma should be kept in the list of differential diagnosis in such cases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kaposi M. Lymphangioma tuberosum multiplex. In: Fagge CH, editor. Hebra on Diseases of the Skin. Vol. 3. London: New Sydenham Society; 1872. p. 386. [Google Scholar]
- 2.Hashimoto K, DiBella RJ, Borsuk GM, Lever WF. Eruptive hidradenoma and syringoma. Histological, histochemical, and electron microscopic studies. Arch Dermatol. 1967;96:500–19. [PubMed] [Google Scholar]
- 3.Friedman SJ, Butler DF. Syringoma presenting as milia. J Am Acad Dermatol. 1987;16:310–4. doi: 10.1016/s0190-9622(87)70041-3. [DOI] [PubMed] [Google Scholar]
- 4.Verma SB. An unusual case of eruptive syringomas presenting as itchy symmetrical lesions on both forearms in a patient of hyperkeratotic eczema. Indian Dermatology Online J. 2011;2:104–6. doi: 10.4103/2229-5178.86004. [DOI] [PMC free article] [PubMed] [Google Scholar]