

Abstract
Purpose
Gated single photon emission computed tomography (SPECT) using thallium-201 (Tl-201) has the capacity to evaluate the earlier post-stress (PS) function compared to technetium-99m labeled tracers, and may be more sensitive in detecting transient ventricular dysfunction caused by stress-induced ischemia. The purpose of this study was to assess the prognostic value of functional variables obtained from Tl-201 gated SPECT as a predictor of major adverse cardiac events (MACE).
Methods
Four hundred and thirty-eight subjects who had known or suspected coronary artery disease and underwent clinically indicated dipyridamole-stress electrocardiography-gated Tl-201 SPECT were included in this study. Functional variables, including PS-ejection fraction (EF), PS-end systolic volume (ESV), PS-regional wall motion abnormality (RWA), reversible RWA and EF worsening, were generated to study the correlation with MACE (cardiac death, nonfatal infarction, unstable angina and coronary revascularization).
Results
Sixty-eight of the total 438 patients (15.5%) had MACE during the period of follow-up (a median time of 31 months), including 2 cardiac deaths, 9 non-fatal infarctions, 9 unstable angina and 48 coronary revascularizations. These events occurred significantly more frequently in patients with reversible RWA (28.8% vs. 7.1%, p < 0.0001), EF worsening (34.8% vs. 12.1%, p < 0.0001), PS-RWA (29.9% vs. 11.4%, p < 0.0001) and PS-EF < 45% (27.8% vs. 14.4%, p = 0.034). Using the Cox proportional hazards regression analysis, reversible RWA and EF worsening were two independent predictors of MACE, providing incremental prognostic value over clinical and perfusion-alone information.
Conclusions
The functional assessment with Tl-201 gated SPECT was a useful prognosticator for patients who had known or suspected coronary artery disease.
Keywords: Coronary artery disease, Gated SPECT, Major adverse cardiac events, Tl-201
INTRODUCTION
Electrocardiography (ECG)-gated myocardial perfusion single photon emission computed tomography (SPECT) enables the simultaneous evaluation of perfusion and function of the left ventricle (LV) in a single imaging procedure. This imaging technique was initially validated for technetium-99m labeled tracers1,2 and later proved to be technically sufficient for thallium-201 (Tl-201) tracer even though the imaging procedure is limited by the radiation dosimetry with a relatively lower photon count density.3-5 The advantage of Tl-201 gated SPECT has also been underscored by its capability of obtaining the early post-stress (PS) ventricular function close to vasodilator-stressed peak-hyperemia, which may be more sensitive to discovering functional abnormality as transient ventricular dysfunction for myocardial stunning in response to stress-induced ischemia.6,7
Our early data demonstrated that the early PS LV ejection fraction (EF) measured with Tl-201 gated SPECT was highly correlated with severe coronary artery disease (CAD) as a strong predictor for CAD.8,9 Recently, a similar finding was reported by the study of rubidium-82 myocardial perfusion positron emission tomography (PET) capable of using peak-stress LV function as the CAD predictor.10,11 The same study further reported the incremental value for predicting patient outcome when the assessment of LV function was added to clinical or perfusion-alone information. Hypothetically, the abnormality of LV mechanical contraction obtained during maximized coronary artery dilation with peak-stress imaging should provide the optimal functional information for predicting patient outcome. Whether the functional parameters acquired from early post-stress imaging can generate a similar prognostic value as the peak-stress imaging is still not yet apparent. The purpose of our study was to evaluate if PS functional variables generated by gated Tl-201 SPECT can be a valuable predictor to major adverse cardiac events (MACE) as the endpoint.
MATERIALS AND METHODS
Patients
We retrospectively reviewed 633 consecutive subjects who had known or suspected CAD and were referred for dipyridamole-stress/rest gated Tl-201 myocardial perfusion imaging in the nuclear laboratory of Changhua Christian Hospital for diagnosis and/or risk stratification of CAD. Follow-up was available in 438 patients (69%). The study protocol was approved by the Institutional Review Board of Changhua Christian Hospital.
Gated Tl-201 SPECT
Patients fasted at least 4 hours and were asked to abstain from caffeine-containing foods, beverages and medications containing methylxanthine for 24 hours. Dipyridamole was administered intravenously at a rate of 0.14 mg/kg/min for 4 minutes. 111 MBq of Tl-201 was then injected 3 minutes after the end of the dipyridamole infusion. Blood pressure and heart rate were recorded every 1 minute. Aminophylline was given for patients suffering from chest pain, dyspnea, nausea, vomiting, severe bradycardia (heart rate less than 40 bpm), 2nd or 3rd degree atrioventricular block, ST depression, or frequent premature ventricular contractions.
PS and rest gated SPECT were performed 5 minutes and 4 hours after Tl-201 injection in a supine position. A dual-head gamma camera (Millennium MG, GE, Haifa, Israel) equipped with a low-energy/general-purpose collimator was used. Thirty-two projections, with 70s of data collection per projection, were obtained over a 180° arc extending from the 45° right anterior oblique to the 45° left posterior oblique position. A 20% window was centered over the 72 and 167 keV Tl-201 photo-peaks. The acquisition was synchronized with ECG with an acceptance window of 100%, and each projection was divided into 8 images per cardiac cycle. The projection images were acquired into 64 × 64 matrices with a 1.60 acquisition zoom, and were reconstructed by filtered back projection with a Butterworth filter (order 10 and cut-off frequency 0.35 cycle/pixel).
For analysis of gated SPECT, LV was divided into 20 segments, and all segments were scored on a 5-point scale (0, normal; 1, mildly reduced; 2, moderately reduced; 3, severely reduced; and 4, absent uptake). The summed stress score (SSS) and summed rest score (SRS) were the sum of the scores of 20 segments on stress and rest images. SSS < 4 was considered as normal; between 4 to 8, mildly abnormal; between 9 and 13, moderately abnormal; and > 13, severely abnormal.12
Functional variables, including wall motion, LVEF, end-diastolic volume (EDV) and end-systolic volume (ESV), were assessed by automated software (QGS 3.0). Regional function was scored by a 5-point scale: 0, normal; 1, mildly hypokinetic; 2, moderately hypokinetic; 3, severely hypokinetic, and 4, akinetic or dyskinetic.13 SSS for wall motion (SSSWM) and SRS for wall motion (SRSWM) were calculated by adding the scores of 20 segments in the stress and rest gated images, respectively. SDS for wall motion (SDSWM) was derived as the difference between the SSSWM and the SRSWM. SDSWM greater than 2 and SSSWM greater than or equal to 4 were used to define the presence of reversible regional wall motion abnormality (RWA) and PS-RWA, respectively.14 A decrease of ≥ 6% in PS-EF compared to rest-EF were defined as “EF worsening”.7 PS functional variables, including PS-RWA, reversible RWA, EF worsening, PS-EF < 45% and PS-ESV > 70 ml15 were correlated with the primary end point.
Follow-up
Patient follow-up was performed by telephone interview. MACE criteria defined as cardiac death, nonfatal infarction, unstable angina and coronary revascularization (in order of event severities) was used as the primary end point to terminate follow-up. Events were confirmed by hospital admission records. If a patient experienced more than one event during the follow-up period, only the most severe event was counted.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and tested by Student’s t-test. Non-continuous variables were expressed as frequency and percentage and tested by a chi-square test. Cox proportional hazards regression analysis was performed to identify independent predictors of events, and time-to-event analyses were performed by Kaplan-Meier analyses. A p value less than 0.05 was considered significant.
RESULTS
Clinical characteristics
The patients were followed for a median time of 31 months (minimum: 28 months; maximum: 37 months). In the total 438 patients, 68 patients (15%) had MACE (2 cardiac deaths, 9 nonfatal infarctions, 9 unstable an-ginas and 48 coronary revascularizations). The clinical characteristics of patients are shown in Table 1. The patients with MACE were more often male, with a history of myocardial infarction and/or prior coronary revascularization. No significant difference was observed between patients with and without MACE in age and the frequency of hypertension, diabetes, hyperlipidemia, family history of CAD and smoking status.
Table 1. Clinical characteristics.
| Event-free | MACE | p value | |
| Age | 68 ± 11 | 69 ± 12 | 0.449 |
| Male | 188 (51) | 48 (71) | 0.003 |
| Hypertension | 225 (61) | 46 (68) | 0.286 |
| Diabetes | 115 (31) | 23 (34) | 0.655 |
| Hyperlipidemia | 148 (40) | 32 (47) | 0.665 |
| Family History | 49 (13) | 11 (16) | 0.518 |
| Smoking | 101 (27) | 17 (25) | 0.855 |
| Hx of MI | 16 (4) | 8 (12) | 0.013 |
| Hx of PCI/CABG | 28 (8) | 12 (18) | 0.008 |
Values are mean ± standard deviation or n (%).
CABG, coronary artery bypass grafting; Hx, history; MACE, major adverse cardiac events; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Functional variables and outcome
Perfusion and functional parameters of patients with and without MACE are shown in Table 2. Briefly, the patients with MACE had higher SSS, SRS, SSSWM and SRSWM; larger LVEDV and LVESV; and lower LVEF. Table 3 shows the probability of events at various time points as stratified by the functional variables. The patients with reversible RWA, EF worsening, PS-RWA and PS-EF < 45% were significantly more likely to have MACE than those without. The frequency of MACE was not significantly different between patients with and without PS-ESV > 70 ml. On Cox hazards regression analysis (Table 4), MACE were independently predicted by the severity of perfusion abnormality (SSS) [odds ratio (OR), 1.10; 95% confidence interval (CI), 1.05-1.15], the presence of reversible RWA (OR, 2.96; 95% CI, 1.41-6.20) and EF worsening (OR, 2.25; 95% CI, 1.05-4.84). Figure 1 depicts the Kaplan-Meier estimates of the cumulative probability free of MACE for patient with no or mild perfusion abnormality (SSS < 8), and the patients with reversible RWA and EF worsening were still significantly more likely to have MACE than those without.
Table 2. erfusion and functional parameters of patients with and without MACE.
| Event-free | MACE | p value | |
| SSS | 2.2 ± 5.1 | 9.5 ± 10.2 | < 0.0001 |
| SRS | 0.9 ± 3.6 | 3.4 ± 5.9 | 0.001 |
| SSSWM | 5.3 ± 10.6 | 14.2 ± 13.9 | < 0.0001 |
| SRSWM | 6.8 ± 10.2 | 12.3 ± 13.8 | 0.003 |
| LVEDV | 64.5 ± 31.0 | 78.8 ± 44.8 | 0.014 |
| LVESV | 25.6 ± 26.1 | 38.3 ± 43.2 | 0.022 |
| LVEF | 65.6 ± 13.5 | 57.5 ± 14.9 | < 0.0001 |
Values are mean ± standard deviation or n (%).
LVEDV, left ventricular end-diastolic volume; LVEF, LV ejection fraction; LVESV, LV end-systolic volume; MACE, major adverse cardiac events; SRS, summed rest score; SRSWM, SRS for wall motion; SSS, summed stress score; SSSWM, SSS for wall motion.
Table 3. The outcome as stratified by functional variables.
| Cumulative probability of events | |||||
| n (%) | 30 Days | 1 Yr | 2 Yrs | p value | |
| n (%) | 30 Days | 1 Yr | 2 Yrs | p value | |
| Reversible RWA (-) | 268 (62.2%) | 2 (0.7%) | 10 (3.7%) | 19 (7.1%) | < 0.0001 |
| Reversible RWA (+) | 170 (38.8%) | 11 (6.5%) | 36 (21.2%) | 49 (28.8%) | |
| EF worsening (-) | 372 (84.9%) | 8 (2.2%) | 29 (7.8%) | 45 (12.1%) | < 0.0001 |
| EF worsening (+) | 66 (15.1%) | 5 (7.6%) | 17 (25.8%) | 23 (34.8%) | |
| PS-RWA (-) | 341 (77.9%) | 6 (1.8%) | 22 (6.5%) | 39 (11.4%) | < 0.0001 |
| PS-RWA (+) | 97 (22.1%) | 7 (7.2%) | 24 (24.7%) | 29 (29.9%) | |
| PS-EF < 45% (-) | 402 (91.2%) | 11 (2.7%) | 39 (9.7%) | 58 (14.4%) | 0.034 |
| PS-EF < 45% (+) | 36 (8.8%) | 2 (5.6%) | 7 (19.4%) | 10 (27.8%) | |
| PS-ESV < 70 ml (-) | 403 (92%) | 12 (3%) | 40 (9.9%) | 60 (14.9%) | 0.212 |
| PS-ESV < 70 ml (+) | 35 (8%) | 1 (2.9%) | 6 (17.1%) | 8 (22.9%) |
Values are n (%).
EF, ejection fraction; ESV, end-systolic volume; MACE, major adverse cardiac events; PS, post-stress; RWA, regional wall motion abnormality.
Table 4. Cox proportional hazards regression analysis of functional, perfusion and historical variables.
| OR | 95% CI | p value | |
| Reversible RWA | 2.96 | 1.41-6.20 | 0.0041 |
| EF worsening | 2.25 | 1.05-4.84 | 0.0374 |
| PS-RWA | 1.02 | 0.46-2.23 | 0.97 |
| PS-EF < 45% | 0.35 | 0.11-1.06 | 0.064 |
| SSS | 1.1 | 1.05-1.15 | < 0.0001 |
| Hx of MI | 1.75 | 0.61-5.02 | 0.2951 |
| Hx of PCI/CABG | 1.29 | 0.54-3.12 | 0.5625 |
CABG, coronary artery bypass grafting; EF, ejection fraction; Hx, history; MI, myocardial infarction; PCI, percutaneous coronary intervention; PS, post-stress; RWA, regional wall motion abnormality; SSS, summed stress score.
Figure 1.
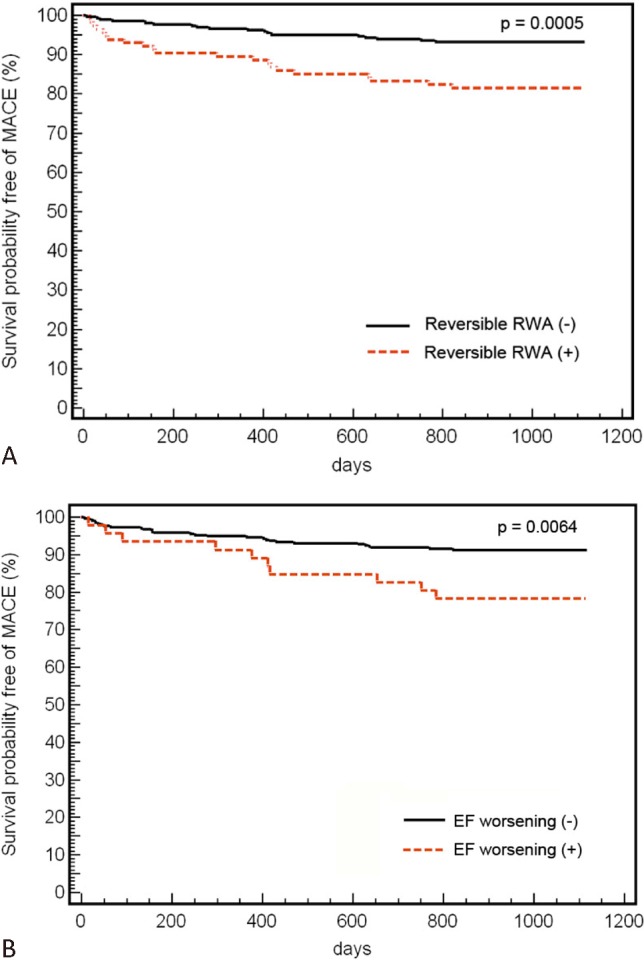
Cumulative major adverse cardiac event (MACE)-free survival for patients with no/mild perfusion abnormality as stratified by (A) reversible regional wall motion abnormality (RWA) and (B) ejection fraction (EF) worsening.
Figure 2 and Figure 3 show example images of a patient with remarkably reversible RWA and EF worsening, but a near-normal perfusion image on gated Tl-201 SPECT. The patient later was found to have severe and extensive coronary artery disease and was referred for coronary artery bypass graft surgery.
Figure 2.

Example images of a 79-year-old male patient with suspected coronary artery disease referred for dipyridamole-stress/rest gated Tl-201 myocardial perfusion SPECT for diagnosis and risk stratification. The short-axis, vertical long-axis and horizontal long-axis perfusion images of stress (upper column) and rest (lower column) showed only minimally reversible perfusion abnormality (near-normal) in apical anterior segment of left ventricular myocardium.
Figure 3.
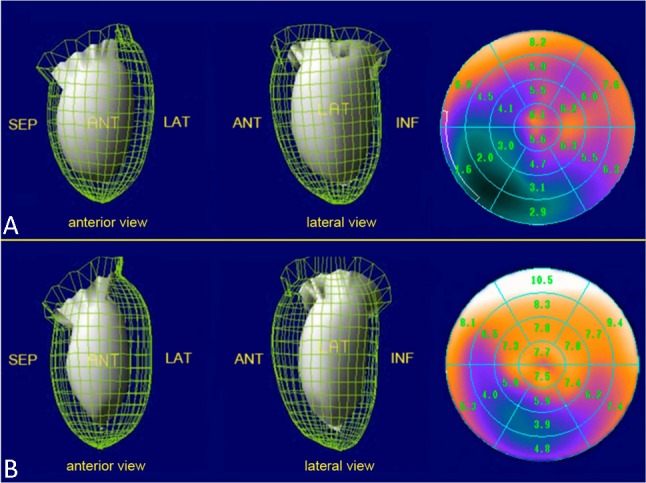
Example post-stress (A) and rest (B) functional 3D (left and middle rows) and quantitative (right row) images by Tl-201 gated SPECT from the same patient in Figure 2. Stress-induced worsening of regional wall motion (reversible RWA) was observed in septum and inferior walls. The ejection fraction (EF) of post-stress and rest were 55% and 70%, respectively (worsening EF). Unstable angina developed subsequently and invasive coronary angiography showed triple-vessel disease. The patient was sent for coronary artery bypass graft surgery.
DISCUSSION
In comparison with Tc-99m-labeled tracers, Tl-201 has some physical drawbacks, including lower photon energy, longer half-life and limited injection dose with a higher radiation burden to the patient. However, Tl-201 remains the most widely used tracer for myocardial perfusion imaging (MPI) in many developed or developing Asian countries because the simplicity of a single dose injection for stress/rest imaging with the ability to assess myocardial viability when necessary.5 Other explanations as to why Tl-201 remains a preferable tracer include lower cost per patient dose with a relatively lower radiation burden to nuclear medicine personnel compared with Tc99m-labled tracers. Over the last few decades, Tl-201 MPI had established its role in diagnosis, risk stratification and prognostic assessment for cardiac events based on perfusion information;16 however, the independent prognostic value of the functional variable obtained from Tl-201 gated SPECT was still not reported. The findings in our study could provide sufficient evidence to support the role of Tl-201 gated SPECT to better predict patient outcomes.
Sharir et al. first studied the prognostic values of PS-LV function and volume measurements with Tc-99m sestamibi gated SPECT, and found that functional variables added incremental value in predicting cardiac death and cardiac death or nonfatal myocardial infarction (MI) for the patient group with PS-EF < 45% and PS-ESV > 70 ml.15 In our study, there were only 2 cardiac deaths (about 3%) in the total of 68 MACE, which made it impractical to separate cardiac death as an independent event from other MACE events. Travin et al. also studied the prognostic value of Tc-99m sestamibi gated SPECT in a larger patient population, and further clarified that abnormal PS-EF was a significant predictor for cardiac death, but not for nonfatal MI.16 Our data demonstrated a similar result of PS-EF (p = 0.034) and PS-ESV (p = 0.212) for MACE, which may also suggest that PS-EF and PS-ESV obtained from Tl-201 gated SPECT might not be predictive for MACE other than cardiac death. In addition, the same study from Travin et al.16 also showed that the cumulative cardiac event rate (cardiac death and MI) was significantly higher in patients with PS-RWA than those without PS-RWA, and this trend could also be observed in the subgroup with even normal PS-EF. In our study, a remarkable difference (p < 0.0001) in MACE between patients with and without PS-RWA was also observed to consistently imply that PS-RWA (a marker of regional LV function) can be a more sensitive marker of damaged and/or jeopardized myocardium than abnormal PS-EF (a marker of global LV function).
Johnson et al. demonstrated that “myocardial stunning”, defined as prolonged global and/or regional myocardial dysfunction after stress-induced ischemia, may be manifested as transient PS decline of LVEF (EF worsening) or new PS-RWA (reversible RWA) on stress/rest gated SPECT with Tc99m-labeled tracers.17 However, most of the ischemic stunning transiently resolves during the first 30 to 60 minutes after stress;18 thus hypothetically, the earlier gated SPECT image acquisition post stressing patient is started, the greater the likelihood that functional variables will detect myocardial stunning.9,10 For earlier imaging to capture functional abnormality close to peak-stress, Tl-201 gated SPECT can be a more desirable protocol than Tc99m-labeled gated SPECT protocol, where generally 45-60 minutes passed prior to imaging. In our laboratory, the stress image acquisition for Tl-201 gated SPECT normally starts within 5 minutes after peak-stress tracer injection. Klein et al. had studied the effect of dipyridamole-stress on LV function in CAD and found that dipyridamole is able to induce true ischemia and result in EF worsening and reversible RWA, with the effect lasting between 10 and 25 minutes.19 Therefore earlier imaging with Tl-201 gated SPECT may be a more ideal diagnostic tool than Tc-99m labeled tracers for the purpose of evaluating ischemic stunning.
Dorbala et al. first studied the prognostic value of dipyridamole-stress ECG-gated Rb-82 PET MPI. That study’s protocol started image acquisition within 2 minutes of tracer injection, and they found that LVEF reserve (stress minus rest LVEF) yielded incremental value over clinical, historical and perfusion information in predicting cardiac death or nonfatal MI and all-cause death.11 In our study, a remarkable difference in MACE was also observed between the patients with and without EF worsening (34.8% vs. 12.1%, p < 0.0001) or reversible RWA (28.8% vs. 7.1%, p < 0.0001). Furthermore, reversible RWA and EF worsening were found to be two independent predictors of MACE over clinical and historical information, and a greater hazard than perfusion abnormality. For those patients who had normal perfusion or only mild perfusion abnormalities, they were clinically considered low risk for cardiac event12 or capable of being managed with medical therapy alone.20 However, the survival probability free of MACE for this patient population was still significantly worsened in subgroup patients with reversible RWA or EF worsening, compared to those without reversible RWA or EF worsening. This finding reflected the limitation of MPI, where a balanced reduction of myocardial blood flow can occur in severe two-vessel or triple-vessel disease that possibly manifest normal perfusion or less severe perfusion abnormality in images, yet can lead to an underestimation of CAD. Figure 2 and Figure 3 show an example of a patient with near-normal perfusion but worsening myocardial function due to balanced ischemia.
The major limitation of our study was that the follow-up rate was only modest (69%). The patients lost to follow-up were mainly female, younger, healthier, and had lower pretest probability of CAD with no previous history of MI or PCI/CABG. The absence of this patient population might cause a higher total event rate than the normal clinical setting in our hospital. In addition, the total number of cardiac deaths (n = 2) and nonfatal MI (n = 11) in the total of 91 events among 68 patients was too small to further perform separate statistical analysis for cardiac death, nonfatal MI, or other events as the endpoint.
CONCLUSIONS
The “early” post-stress functional variables obtained from ECG-gated Tl-201 myocardial perfusion SPECT, including reversible regional wall motion abnormality, ejection fraction worsening, post stress regional wall motion abnormality and post-stress ejection fraction < 45% were prognostic indicators for patients with known or suspected CAD. However, reversible regional wall motion abnormality and ejection fraction worsening, as the result of regional and global left ventricle manifestations of ischemic stunning, were the most powerful markers for predicting MACE, even in patients with normal perfusion or only mild perfusion abnormality on MPI. An extended study to enroll a larger number of patients is warranted to further clarify the prognostic values of these functional variables corresponding with different end points of patient outcome.
REFERENCES
- 1.Germano G, Kiat H, Kavanagh PB, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med. 1995;36:2138–2147. [PubMed] [Google Scholar]
- 2.Germano G, Erel J, Lewin H, et al. Automatic quantitation of regional myocardial wall motion and thickening from gated technetium-99m sestamibi myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol. 1997;30:1360–1367. doi: 10.1016/s0735-1097(97)00276-3. [DOI] [PubMed] [Google Scholar]
- 3.Germano G, Erel J, Kiat H, et al. Quantitative LVEF and qualitative regional function from gated thallium-201 perfusion SPECT. J Nucl Med. 1997;38:749–754. [PubMed] [Google Scholar]
- 4.Cwajg E, Cwajg J, He ZX, et al. Gated myocardial perfusion tomography for the assessment of left ventricular function and volumes: comparison with echocardiography. J Nucl Med. 1999;40:1857–1865. [PubMed] [Google Scholar]
- 5.Hung GU, Hsia CH, Yang PT, et al. Performance of thallium-201 electrocardiography-gated myocardial perfusion single photon emission computed tomography to assess left ventricular function. Kaohsiung J Med Sci. 2005;21:203–211. doi: 10.1016/S1607-551X(09)70189-5. [DOI] [PubMed] [Google Scholar]
- 6.Santiago JF, Heiba SI, Jana S, et al. Transient ischemic stunning of the myocardium in stress thallium-201 gated SPET myocardial perfusion imaging: segmental analysis of myocardial perfusion,wall motion and wall thickening changes. Eur J Nucl Med Mol Imaging. 2002;29:979–983. doi: 10.1007/s00259-002-0824-3. [DOI] [PubMed] [Google Scholar]
- 7.Hung GU, Lee KW, Chen CP, et al. Relationship of transient ischemic dilation in dipyridamole myocardial perfusion imaging and stress-induced changes of functional parameters evaluated by Tl-201 gated SPECT. J Nucl Cardiol. 2005;12:268–275. doi: 10.1016/j.nuclcard.2005.03.004. [DOI] [PubMed] [Google Scholar]
- 8.Hung GU, Chen CP, Yang KT. Incremental value of ischemic stunning on the detection of severe and extensive coronary artery disease in dipyridamole Tl-201 gated myocardial perfusion imaging. Int J Cardiol. 2005;105:108–110. doi: 10.1016/j.ijcard.2004.11.018. [DOI] [PubMed] [Google Scholar]
- 9.Hung GU, Lee KW, Chen CP, et al. Worsening of left ventricular ejection fraction induced by dipyridamole on Tl-201 gated myocardial perfusion imaging predicts significant coronary artery disease. J Nucl Cardiol. 2006;13:225–232. doi: 10.1007/BF02971247. [DOI] [PubMed] [Google Scholar]
- 10.Dorbala S, Vangala D, Sampson U, et al. Value of vasodilator left ventricular ejection fraction reserve in evaluating the magnitude of myocardium at risk and the extent of angiographic coronary artery disease: a 82Rb PET/CT study. J Nucl Med. 2007;48:349–358. [PubMed] [Google Scholar]
- 11.Dorbala S, Hachamovitch R, Curillova Z, et al. Incremental prognostic value of gated Rb-82 positron emission tomography myocardial perfusion imaging over clinical variables and rest LVEF. JACC Cardiovasc Imaging. 2009;2:846–854. doi: 10.1016/j.jcmg.2009.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hachamovitch R, Berman DS, Shaw LJ, et al. Incremental prognostic value of myocardial perfusion single photon emission computed tomography for the prediction of cardiac death:differential stratification for risk of cardiac death and myocardial infarction. Circulation. 1998;97:535–543. doi: 10.1161/01.cir.97.6.535. [DOI] [PubMed] [Google Scholar]
- 13.Sharir T, Berman DS, Waechter PB, et al. Quantitative analysis of regional motion and thickening by gated myocardial perfusion SPECT: normal heterogeneity and criteria for abnormality. J Nucl Med. 2001;42:1630–1638. [PubMed] [Google Scholar]
- 14.Petix NR, Sestini S, Marcucci G, et al. Can the reversible regional wall motion abnormalities on stress gated Tc-99m sestamibi SPECT predict a future cardiac event? J Nucl Cardiol. 2005;12:20–31. doi: 10.1016/j.nuclcard.2004.09.017. [DOI] [PubMed] [Google Scholar]
- 15.Sharir T, Germano G, Kavanagh PB, et al. Incremental prognostic value of post-stress left ventricular ejection fraction and volume by gated myocardial perfusion single photon emission computed tomography. Circulation. 1999;100:1035–1042. doi: 10.1161/01.cir.100.10.1035. [DOI] [PubMed] [Google Scholar]
- 16.Sharir T, Bacher-Stier C, Dhar S, et al. Identification of severe and extensive coronary artery disease by postexercise regional wall motion abnormalities in Tc-99m sestamibi gated single-photon emission computed tomography. Am J Cardiol. 2000;86:1171–1175. doi: 10.1016/s0002-9149(00)01206-6. [DOI] [PubMed] [Google Scholar]
- 17.Johnson LL, Verdesca SA, Aude WY, et al. Postischemic stunning can affect left ventricular ejection fraction and regional wall motion on poststress gated sestamibi tomograms. J Am Coll Cardiol. 1997;30:1641–1648. doi: 10.1016/s0735-1097(97)00388-4. [DOI] [PubMed] [Google Scholar]
- 18.Ambrosio G, Betocchi S, Pace L, et al. Prolonged impairment of regional contractile function after resolution of exercise-induced angina. Evidence of myocardial stunning in patients with coronary artery disease. Circulation. 1996;94:2455–2464. doi: 10.1161/01.cir.94.10.2455. [DOI] [PubMed] [Google Scholar]
- 19.Klein HO, Ninio R, Eliyahu S, et al. Effects of the dipyridamole test on left ventricular function in coronary artery disease. Am J Cardiol. 1992;69:482–488. doi: 10.1016/0002-9149(92)90990-g. [DOI] [PubMed] [Google Scholar]
- 20.Hachamovitch R, Hayes SW, Friedman JD, et al. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003;107:2900–2907. doi: 10.1161/01.CIR.0000072790.23090.41. [DOI] [PubMed] [Google Scholar]