

Abstract
Background
The measurements of coronary diameters, usually obtained by 2-dimentsional echocardiography, play important roles oin the management and follow-up of Kawasaki disease (KD). However, in Taiwan, domestic normgrams and a Z-score calculator for coronary artery diameters are still not available.
Methods
Echocardiography was performed on 412 healthy children younger than 6 years of age. The appropriate exponential regression model was fitted to correspond with body surface area (BSA). The computed Z-scores of all subjects were also tested for normal distribution.
Results
Using the model ln (measurement) = β1 + β2 × ln (BSA), the adjusted R2 values were 0.611 and 0.484 for the models of the left main coronary artery (LMCA) and the right (RCA), respectively. Analysis of computed Z-score distribution showed acceptable goodness of fit for a normal distribution [p = 0.90 (LMCA); p = 0.17 (RCA)].
Conclusions
We have established reference ranges for the coronary artery diameters in Taiwanese children younger than 6 years of age. The regression equations and Z-score calculators for the LMCA and RCA provide an objective determination of coronary dilatation in a large population, which is important for the care and medical management of KD patients in Taiwan.
Keywords: Coronary diameter, Kawasaki disease, Taiwan, Z-score
BACKGROUND
Two-dimensional echocardiography is currently one of the most convenient noninvasive methods to measure various intracardiac structures in children.1,2 Clinical decisions are usually made by comparing echocardiographic measurements with data from a matched normal population.2,3 This is especially important in the treatment and follow-up of patients with Kawasaki disease (KD), the leading cause of acquired coronary artery disease in children.4-6 The incidence and prevalence of KD in Taiwanese children younger than 5 years were 66.9 and 164.9 per 100,000, respectively, the third highest in the world.5 KD is an acute systemic vasculitis typically found in young children, and its diagnosis is based on clinical symptoms and signs such as fever for more than 5 days, conjunctivitis, strawberry tongue, skin rash, swollen palms/soles, and lymphadenopathy. Although coronary involvement is not a necessary requisite for diagnosis of KD, echocardiographic coronary evaluation is recommended by the American Heart Association and the Japanese Ministry of Health and welfare because 15-25% of untreated patients will have coronary arterial lesions (CAL).4,7 The CAL ranged from minimal dilatation to giant aneurysms and are accessed serially by echocardiography, primarily by quantifying internal coronary artery diameters.6,7 Commonly used definitions of coronary involvement have relied on the Japanese Ministry of Health dichotomous criteria. This criteria defines abnormalities as having a maximum internal diameter > 3 mm in children < 5 years of age, or > 4 mm in children 5 years and older, or a segment 1.5 times greater than an adjacent segment, or the presence of luminal irregularity.8 Most studies of genetic and clinical risk factors9,10 associated with CAL in KD patients used this definition. However, regression equations based on measurements from nonfebrile normal children have recently been used to calculate Z-scores based on body surface area,11-13 thus allowing a continuous, rather than dichotomous, measurement of coronary artery involvement. Such normalized Z-scores seem to define a more precise spectrum of CAL and determined the associated risk factors.6,14
Previous studies have validated the use of echography to measure coronary diameters15 and have demonstrated high sensitivity (95%) and specificity (99%) of cardiac sonography for identifying coronary lesions in KD patients.16 However, there are limited echographic studies11-13 in the literature that provide Z-score distribution and calculations for the coronary arteries in children, especially in a Han Chinese population. The purpose of this study was to determine the coronary luminal diameter adjusted for the body size of normal Taiwanese children. Statistical analysis was also carried out to compute the best fit model and regression equations to allow the generation of a Z-score.
METHODS
Patients
All children referred to the pediatric cardiology outpatient clinic of seven hospitals between Jan 2009 and Dec 2012 for systolic murmur or chest pain who underwent complete transthoracic echocardiographic studies were considered for inclusion in this study. Patients were enrolled if they had normal physical examination results (including physiologic murmur) and their echocardiograms were interpreted as normal by the attending cardiologists. Exclusion criteria consisted of the presence of structural heart disease, concurrent fever, ventricular hypertrophy, cardiac manifestation of a systemic disease, or suspicion or history of Kawasaki disease. The height, weight, age and gender of all patients were recorded, and the body surface area (BSA) for each patient was estimated using the formula of Du Bois & Du Bois17 and Mosteller.18
Echocardiography
All patients underwent complete 2-dimensional echocardiographic studies with color flow and spectral Doppler examination. Studies were all performed using iE33 ultrasound system (Philips Medical Systems, Best, the Netherlands) and recorded digitally. The studies were then exported from the institution’s echocardiography server into the Xcelera (Philips Medical Systems, Andover, MA) for analysis and measurement offline.
Coronary artery measurements
The intraluminal diameters of coronary segments were measured from one inner edge to the other inner edge on each digital study. The left main coronary artery (LMCA) was measured midway between the ostia and the bifurcation of the circumflex coronary artery and the left anterior descending coronary artery (LAD). The right coronary artery (RCA) and LAD were measured 3 to 5 mm distal to their origins in the parasternal short-axis view.19 Each measurement was performed by one cardiologist. For a randomly selected 10% of the subjects, a second sonographer (CE Chang, YM Chang, CA Chen, YC Chen, SN Chiu, JY Hsu, YL Huang, CW Lu, JY Ma, CS Wu, SZ Yeh), who was blinded to the first of readings, measured independently the coronary diameters off-line. The interobserver variability was tested by using intra-class correlation coefficient and comparing readings of the first and second sonographers. A p-value smaller than 0.05 was considered statistically significant.
Data analysis
Previous regression studies6,11,12 showed that an exponential model would offer good fit and yield Z-scores evenly distributed around zero even for smaller children (i.e. BSA smaller than 0.3 m2). Therefore, we selected the following model for the regression analysis [where coronary diameter (CA) equals the measurement coronary diameters, and BSA means body surface area].
ln (CA) = β1 + β2 × ln (BSA)
Then, outliers were identified in each data set of LMCA, RCA and LAD and the model parameters were recalculated. Outliers were considered to be those measurements whose “studentized deleted residual” was > 3 for the model in question. The demographic data are presented as mean and standard deviation (± SD) or as the median and the interquartile range (IQR) for continuous variables, such as age and body weight. Frequencies and percentages were used to describe the categorical variables, and proportionality differences were tested by χ2 analysis.
Z-score goodness of fit to a normal distribution
The Z-score is a standardized score that represents how many standard deviations a value is above or below the population mean in a normally distributed population. Theoretically, Z-scores should be normally distributed. In the current exponential model, we used the Anderson-Darling test20 to measure the goodness of fit of our calculated Z-scores for a normal distribution with a mean of zero and a standard deviation of one. The Anderson-Darling test20 is used to test if a sample of data came from a population with a specific distribution. The test is a one-sided test and the hypothesis that the distribution is of a specific form is rejected if the test statistic, A, is greater than the critical value. The critical values for the Anderson-Darling test are tabulated and formulas have been published for a few specific distributions including normal distributions.20
Comparison with previous equations
Several non-linear formulas for coronary diameters have been earlier reported in studies such as McCrindle et al.,6 Dallaire et al.11 and Olivieri et al.12 We also analyzed Z-scores obtained with our cohort using the three previously published non-linear equations. Z-score boundaries, represented by Z = +2 and -2, for the current equation and three previous equations, were plotted together for easier comparisons.
RESULTS
Demographic data
Between 2009 and 2012, 412 eligible echocardiographic studies were included in our investigation, of which 55.3% were male patients. Of these eligible patients, their weight ranged from 2.1 to 29 kg [mean: 11 kg: standard deviation (SD): 8.1 kg], and the median age was 29.5 months old with a SD of 21.6 months. The body surface area (BSA) of the participants ranged from 0.16-0.98 m2 with a mean of 0.54 m2 (SD: 0.17 m2). The distribution of age and body surface area (BSA) of enrolled subjects is shown in Figure 1(A) and (B), respectively.
Figure 1.
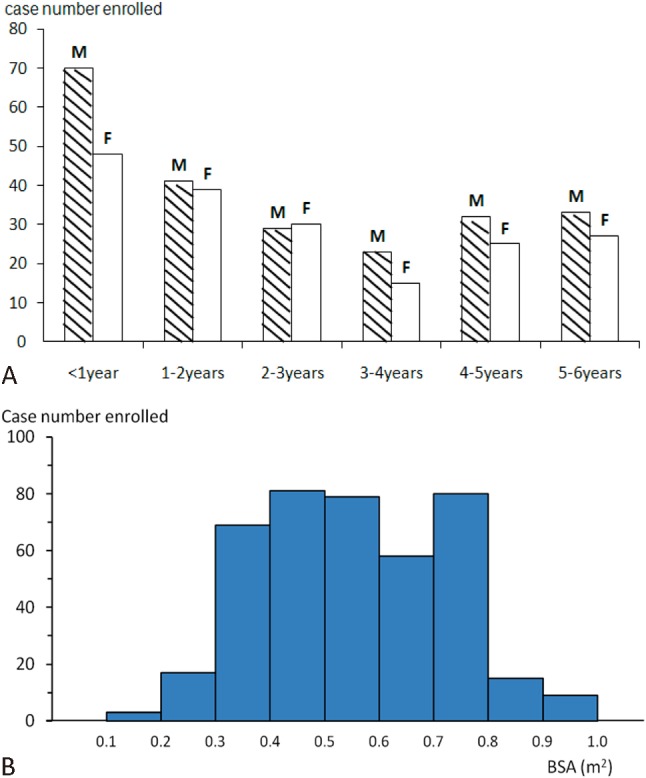
Distribution of (A) age and (B) body surface area of the enrolled children.
Of the 412 studies, 13 studies were excluded (all had missing data either for height or weight). Coronary artery measurements of 399 LMCA, 399 RCA and 191 LAD were enrolled for modeling. The measurability of LAD was relatively low (46.8%). Coronary diameters were then modeled with BSA. Exponential models were fitted, and outlier data were then eliminated (3 of LMCA and 2 of RCA) and the model parameters were recalculated based on the measurements of 396 LMCA, 397 RCA and 191 LAD. Parameter estimates, R2 (squared correlation coefficient), and Anderson-Darling statistical tests for the final models are presented in Table 1.
Table 1. Final regression analysis using exponential model.
| n | R2 | Beta_1 | Beta_2 | MSE | A-Statistic | p-value | |
| RCA | 397 | 0.4838 | -1.6603 | 0.3768 | 0.0533 | 0.1886 | 0.9011 |
| LMCA | 396 | 0.611 | -1.4381 | 0.4182 | 0.0341 | 0.5379 | 0.1671 |
| LAD | 191 | 0.3985 | -1.7163 | 0.4093 | 0.0948 | 1.1472 | 0.0052 |
ln (CA) = β1 + β2 × ln (BSA).
A-statistic, The Anderson-Darling test statistic; BSA, body surface area; CA, coronary diameter; LAD, left anterior descending coronary artery; LMCA, left main coronary artery; MSE, mean standard error; R2, squared correlation coefficient; RCA, right coronary artery.
Calculation and goodness of fit of Z-score
To obtain the Z-score for a given coronary measurement, we first used the values of mean square error, β1 and β2 corresponding to the examined coronary segment. The Z-score value was then calculated from the following equation:
Z-score = [ln (CA) - β1 - β2 × ln (BSA)]/standard error
Then we used the Anderson-Darling test18 to measure the goodness of fit of our calculated Z-score for a normal distribution. The P values for coronary diameters of LMCA, RCA and LAD were 0.90, 0.17 and 0.005 respectively, which indicated no significant departure from normal distribution except for the LAD measurements. Scatterplots of Z-scores of RCA, LMCA and LAD diameters versus body surface area are shown in supplement Figure 1. Z-score (+2.5) boundaries of LMCA and RCA are also shown in Table 2.
Table 2. Z-score (+2.5) boundaries of LMCA and RCA diameters in Taiwanese children younger than 6 years old.
| BSA (m2) | LMCA (mm) | RCA (mm) |
| 0.2 | 1.9215 | 1.8458 |
| 0.25 | 2.1095 | 2.0077 |
| 0.3 | 2.2766 | 2.1505 |
| 0.35 | 2.4282 | 2.2791 |
| 0.4 | 2.5677 | 2.3967 |
| 0.45 | 2.6974 | 2.5055 |
| 0.5 | 2.8189 | 2.6069 |
| 0.55 | 2.9335 | 2.7023 |
| 0.6 | 3.0423 | 2.7923 |
| 0.65 | 3.1458 | 2.8778 |
| 0.7 | 3.2449 | 2.9593 |
| 0.75 | 3.3399 | 3.0372 |
| 0.8 | 3.4312 | 3.112 |
| 0.85 | 3.5193 | 3.1839 |
| 0.9 | 3.6045 | 3.2532 |
| 0.95 | 3.6869 | 3.3202 |
| 1 | 3.7669 | 3.3849 |
BSA, body surface area; LMCA, left main coronary artery; RCA, right coronary artery.
Interobserver variability
Interobserver variability were assessed in 41 patients (age: 6 months~5.5 years, median 2.4 years old). The interobserver reliability, assessed by using intra-class correlation coefficient, was 0.81, 0.85 and 0.66 for the measurements of LMCA, RCA and LAD, indicating a strong consistency in the LMCA and RCA measurements and a moderate to strong consistency in the LAD readings. Interobserver differences were 0.21 ± 0.11 mm in the LMCA, 0.19 ± 0.13 mm in the RCA and 0.19 ± 0.11 mm in the LAD.
Gender effect
No significant difference of BSA was noted between gender groups (p = 0.36). Additionally, stepped regression analysis also showed no significant independent effect of gender on the coronary diameters (data not shown). Consequently, gender-specific models were not further developed to avoid a decrease in statistical power.
Effect of BSA-estimation formula
Although the original BSA estimation proposed by Du Bois and Du Bois et al.15 is widely used, other enhanced formulas, like Mosteller’s formula,16 have been developed for infants and younger children. Regression results from LMCA were compared when using different BSA-estimation methods, Mosteller’s equation and Du Bois & Du Bois’s method. The Z-scores obtained were very similar and misclassification was observed for only 0.2% of subjects classified as abnormal (Z > 2.5) for BSA using the Du Bois & Du Bois’s method, but normal with BSA from Mosteller’s equation.
Comparison with previous equations
We analyzed Z-scores obtained with our cohort using three previously published non-linear equations.6,11,12 Figure 2(A) and (B) demonstrates the LMCA and RCA cutoffs of Z = -2 and Z = +2 for the current and previous equations.6,11,12 Visually, the data from our study correlated very closely with those of McCrindle et al. in RCA diameters, and with Dallaire et al. in the LMCA diameters. Results of the Anderson-Darling tests on the BSA-dependent Z-scores of LMCA and RCA, generated from any equations of the current study, McCrindle et al. or Dallaire et al., are shown in Table 3. Only the regression equations from our study did not yield significant departure from normality in the measurement of LMCA and RCA diameters (p > 0.05).
Figure 2.
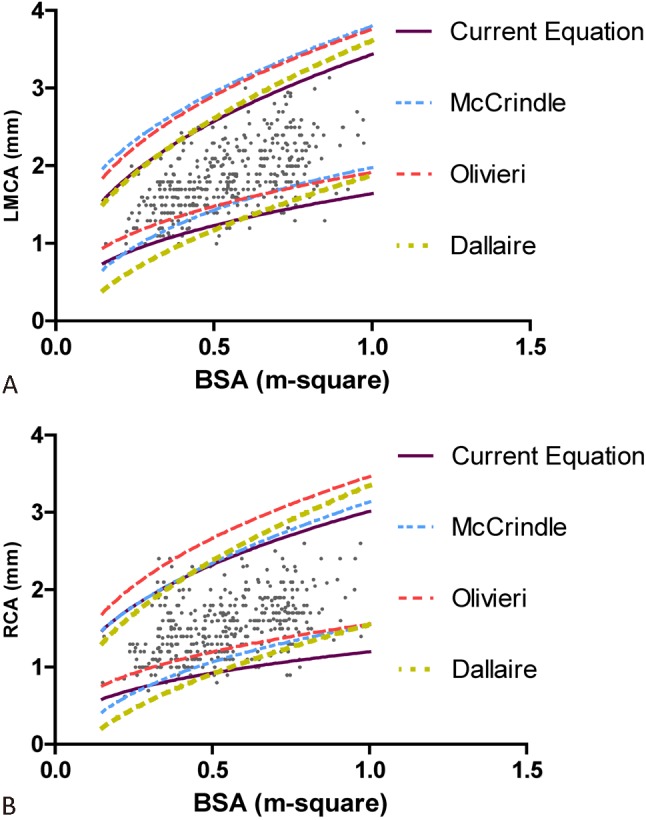
Z-score boundaries of the current and previous equations for (A) the left main coronary artery (LMCA) and (B) right coronary artery (RCA) against BSA.
Table 3. Results (p-value) of Anderson-Darling test on Z-scores generated from the current and three previously reported equations.
| LMCA | RCA | |
| Current | 0.9011 | 0.1671 |
| McCrindle et al. | 0.0247 | 0.0354 |
| Olivieri et al. | 0.0285 | 0.0078 |
| Dallaire et al. | 0.5366 | 0.0477 |
LMCA, left main coronary artery; RCA, right coronary artery.
DISCUSSION
We present novel regression equations and Z-score calculators for digital echocardiographic measurements of coronary arteries in a large group of the Han Chinese people. Pediatric coronary Z-scores are critical for managing children with KD. It has been increasingly recognized that dichotomous criteria based on absolute size is npt always reliable,7,21,22 and classification of coronary abnormalities on the basis of Z-score has already been proposed.14 Furthermore, the data from our study correlated closely with those of McCrindle et al. only in the RCA diameters, and with Dallaire et al. only in the LMCA diameters. These results suggest that we do need our own Z-score calculators in Taiwan to accurately reflect the Han Chinese population.
The initial recommendations for coronary dilatation and aneurysms, issued by the Ministry of Health and Welfare in Japan, defined coronary abnormalities as an internal lumen diameter ≥ 3 mm in a child less than 5 years old, or ≥ 4 mm in a child 5 years of age or older. Based on the growth chart used in Taiwan,23 the 97th percentile of body height and weight for a 5-year-old child were 118.7 cm and 24.4 kg, respectively. Application of these data into the current Z-score calculator showed all Z-scores exceeded 3.0 when diameters of LMCA, RCA and LAD were set as 4 mm. Using a 4.5-year-old child in the 97th percentile for body weight and height, the Z-score readings with LMCA of 3 mm (Z = 1.73) and LAD of 3 mm (Z = 2.1) were diametrically opposite to that of RCA (Z = 2.53). Such phenomenon reflected the non-differentiation among LMCA, LAD and RCA for the Japanese dichotomous criteria of coronary dilatation.
In the study of Dallaire et al., the square root model was also demonstrated to be good for the development of the Z-score calculator. To explore if any other regression models provide better fit for measurements in this study, we also developed the linear additive, power, logarithmic and square root models, and then applied the Anderson-Darling tests to these models. However, all of these models showed a significant depart from normality in RCA diameters (p = 1.1 × 10-3 for the linear model; p = 1.0 × 10-3 for the power model; p = 7.1 × 10-4 for the logarithmic model; p = 9.2 × 10-4 for the square root model).
Our study applied an exponential approximation incorporating BSA as the independent variable and provided an acceptable fit. BSA is a familiar reference standard for pediatricians and pediatric cardiologists to correct individual biometric variations, and a function of both height and weight. Thus, one could argue that several calculators were available to estimate BSA. In the current study, we deduced the regression with Du Bois & Du Bois’ and Mosteller’s formulas, with similar results.
We used exponential transformation to address heteroscedasticity, similar to that process proposed by Olivieri et al.11 Exponential transformation has been widely used to stabilize variance of biological variables, but such an artificial transformation often introduces data distortion and carries the associated risk when introduced by back-transformation from the logarithmic scale. Such a distortion might be one explanation for the departure of Z-scores of LAD measurements from a normal distribution. Another reason for the distortion of LAD diameters from normal distribution might be caused by the relatively low measurability of LAD compared with those of LMCA and RCA (191/412 vs. 399/412 and 399/412). Particularly in infants with BSA smaller than 0.4 m2, the measurability of LAD decreased to 33.3% (32/95), which was significantly lower than that in the remaining enrolled participants (159/317, p = 4.7 × 10-3). Therefore, we suggest the application of Z-score calculator to the measurements of LAD diameters be carefully undertaken, especially in younger patients.
Previous studies24 used computed tomography (CT) to establish reference curve and linear formulas for the coronary diameters in infants and children. The results appeared satisfactory and also demonstrated no significant difference in the coronary arterial size between the genders. However, patient exposure to radiation and contrast media during CT examinations are issues of ongoing concern. Furthermore, coronary artery examinations and measurements should be repeated at the acute stage and 2 weeks, 6-8 weeks, 6 months and 12 months after onset of KD. One dose of CT radiation in KD children may be unremarkable, but the repeated and accumulated exposure of radiation and contrast medium may be harmful. Echocardiography is currently a preferred tool to do the biometrical measurements for all cardiac structures, especially in children.
Limitations
Our study had the following limitations. First, the number of echocardiographic examinations enrolled was relatively small, especially for the measurements of LAD. Therefore, the small number of cases may result in the deviation of statistical assumption. An independent large cohort of healthy children should be further studied to validate the current regression equation, decrease the deviation from normality and raise the feasibility of comparisons with the current Japanese dichotomous criteria. Second, we only did measurements on the LMCA, proximal LAD and proximal RCA. We didn’t assess the remaining coronary segments such as mid-RCA and proximal LCX.17 Future large-scale advanced echocardiographic studies should be performed based on the standard method recommended by the Japan Kawasaki Disease Society.17
CONCLUSIONS
In conclusion, we have established reference ranges for coronary artery diameters in Taiwanese children. The regression equations and Z-score calculators for the LMCA and RCA provide an objective determination of coronary dilatation, which is important in patients with Kawasaki disease.
SUPPLEMENT
Supplement Figure 1.

Scatterplots of Z-scores of right coronary artery (RCA) (A), left main coronary artery (LMCA) (B) and left anterior descending artery (LAD) (C) diameters versus body surface area (BSA).
REFERENCES
- 1.Henry WL, Gardin JM, Ware JH. Echocardiographic measurements in normal subjects from infancy to old age. Circulation. 1980;62:1054–1061. doi: 10.1161/01.cir.62.5.1054. [DOI] [PubMed] [Google Scholar]
- 2.Pettersen M, Du W, Skeens M, Humes RA. Regression equations for calculation of z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents:an echocardiographic study. J Am Soc Echocardiogr. 2008;21:922–934. doi: 10.1016/j.echo.2008.02.006. [DOI] [PubMed] [Google Scholar]
- 3.Capannari TE, Daniels SR, Meyer RA, et al. Sensitivity, specificity and predictive value of two-dimensional echocardiography in detecting coronary artery aneurysms in patients with Kawasaki disease. J Am Coll Cardiol. 1986;7:355–360. doi: 10.1016/s0735-1097(86)80505-8. [DOI] [PubMed] [Google Scholar]
- 4.JCS Joint Working Group. Guidelines for Diagnosis and Management of Cardiovascular Sequelae in Kawasaki Disease (JCS 2008, Digest Version) Circ J. 2010;74:1989–2020. doi: 10.1253/circj.cj-10-74-0903. [DOI] [PubMed] [Google Scholar]
- 5.Huang SK, Lin MT, Chen HC, et al. Epidemiology of Kawasaki disease:prevalence from national database and future trends projection by system dynamics modeling. J Pediatr. 2013;163:126–131. doi: 10.1016/j.jpeds.2012.12.011. [DOI] [PubMed] [Google Scholar]
- 6.McCrindle BW, Li JS, Minich LL, et al. Coronary artery involvement in children with Kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation. 2007;116:174–179. doi: 10.1161/CIRCULATIONAHA.107.690875. [DOI] [PubMed] [Google Scholar]
- 7.Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the committee on rheumatic fever, endocarditis and Kawasaki disease, council on cardiovascular disease in the young, American Heart Association. Pediatrics. 2004;114:1708–1733. doi: 10.1542/peds.2004-2182. [DOI] [PubMed] [Google Scholar]
- 8.Ayusawa M, Sonobe T, Uemura S, et al. Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition) Pediatr Int. 2005;47:232–234. doi: 10.1111/j.1442-200x.2005.02033.x. [DOI] [PubMed] [Google Scholar]
- 9.Lin MT, Wang JK, Yeh JI, et al. Clinical implication of the C Allele of the ITPKC gene SNP rs28493229 in Kawasaki disease:association with disease susceptibility and BCG scar reactivation. Pediatr Infect Dis J. 2011;30:148–152. doi: 10.1097/INF.0b013e3181f43a4e. [DOI] [PubMed] [Google Scholar]
- 10.Lin MT, Hsu CL, Taiwan Pediatric CV Group, et al. A genome-wide association analysis identifies novel susceptibility loci for coronary arterial lesions in patients with Kawasaki disease. Transl Res. 2013;161:513–515. doi: 10.1016/j.trsl.2013.02.002. [DOI] [PubMed] [Google Scholar]
- 11.Olivieri L, Arling B, Friberg M, Sable C. Coronary artery Z score regression equations and calculators derived from a large heterogeneous population of children undergoing echocardiography. J Am Soc Echocardiogr. 2009;22:159–164. doi: 10.1016/j.echo.2008.11.003. [DOI] [PubMed] [Google Scholar]
- 12.Dallaire F, Dahdah N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J Am Soc Echocardiogr. 2011;24:60–74. doi: 10.1016/j.echo.2010.10.004. [DOI] [PubMed] [Google Scholar]
- 13.Ogata S, Tremoulet AH, Sato Y, et al. Coronary artery outcomes among children with Kawasaki disease in the United States and Japan. Int J Cardiol. 2013;168:3825–3828. doi: 10.1016/j.ijcard.2013.06.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Manlhiot C, Millar K, Golding F, McCrindle BW. Improved classification of coronary artery abnormalities based only on coronary artery z-scores after Kawasaki disease. Pediatr Cardiol. 2010;31:242–249. doi: 10.1007/s00246-009-9599-7. [DOI] [PubMed] [Google Scholar]
- 15.Hildick-Smith DJ, Shapiro LM. Transthoracic echocardiographic measurement of coronary artery diameter: validation against quantitative coronary angiography. J Am Soc Echocardiogr. 1998;11:893–897. doi: 10.1016/s0894-7317(98)70009-4. [DOI] [PubMed] [Google Scholar]
- 16.Hiraishi S, Misawa H, Takeda N, et al. Transthoracic ultrasonic visualisation of coronary aneurysm, stenosis, and occlusion in Kawasaki disease. Heart. 2000;83:400–405. doi: 10.1136/heart.83.4.400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Du Bois D, Du Bois EF. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition. 1989;5:303–311; discussion 312-3. [PubMed] [Google Scholar]
- 18.Mosteller RD. Simplified calculation of body-surface area. N Engl J Med. 1987;317:1098. doi: 10.1056/NEJM198710223171717. [DOI] [PubMed] [Google Scholar]
- 19.Fuse S, Kobayashi T, Arakaki Y, et al. Standard method for ultrasound imaging of coronary artery in children. Pediatr Int. 2010;52:876–882. doi: 10.1111/j.1442-200X.2010.03252.x. [DOI] [PubMed] [Google Scholar]
- 20.Stephens MA. EDF statistics for goodness of fit and some comparisons. J Am Stat Assoc. 1974;69:730–737. [Google Scholar]
- 21.Kobayashi T, Saji T, Otani T, et al. Efficacy of immunoglobulin plus prednisolone for prevention of coronary artery abnormalities in severe Kawasaki disease (RAISE study): a randomised,open-label,blinded-endpoints trial. Lancet. 2012;379:1613–1620. doi: 10.1016/S0140-6736(11)61930-2. [DOI] [PubMed] [Google Scholar]
- 22.Crystal MA, Manlhiot C, Yeung RS, et al. Coronary artery dilation after Kawasaki disease for children within the normal range. Int J Cardiol. 2009;136:27–32. doi: 10.1016/j.ijcard.2008.04.019. [DOI] [PubMed] [Google Scholar]
- 23.Chen W, Chang MH. New growth charts for Taiwanese children and adolescents based on World Health Organization standards and health-related physical fitness. Pediatr Neonatol. 2010;51:69–79. doi: 10.1016/S1875-9572(10)60014-9. [DOI] [PubMed] [Google Scholar]
- 24.Chen SJ, Lee WJ, Lin MT, et al. Coronary artery diameters in infants and children with congenital heart disease as determined by computed tomography. Am J Cardiol. 2007;100:1696–1701. doi: 10.1016/j.amjcard.2007.07.016. [DOI] [PubMed] [Google Scholar]