

Abstract
Background
Percutaneous coronary intervention (PCI) for anomalous right coronary artery (RCA) arising from the left sinus of Valsalva (LSOV) is a technical challenge due to inadequate guiding catheter support to overcome the acute rightward course of the anomalous RCA. In this study we describe a novel technique for PCI for an anomalous RCA arising from the LSOV.
Methods
Six patient cases with anomalous RCA arising from the LSOV who underwent PCI from January 2001 to January 2014. The Judkins left (JL) guiding catheter tip orientation is modified by manually bending at the distal tip 90° vertically to fit the acute rightward course.
Results
Of the six patients (mean age: 63 ± 16.7 years), the indication for PCI was acute inferior myocardial infarction (MI) in two, recent inferior MI in two, and angina in two of the cases. Three procedures were performed via a transfemoral approach and the other three via a transradial approach. The median duration of the intervention and total procedure time were 44 and 69.5 minutes, respectively. All patients received successful revascularization without complications.
Conclusions
This novel technique is simple, safe and effective with a 100% procedure success rate for PCI for anomalous RCA arising from the LSOV.
Keywords: Anomalous right coronary artery, Left sinus of Valsalva, Percutaneous coronary intervention
INTRODUCTION
Coronary arteries arising from an anomalous origin are uncommon and encountered in only 0.2-1.2% of patients undergoing diagnostic coronary angiography.1 Percutaneous coronary intervention (PCI) for an anomalous right coronary artery (RCA) arising from the left sinus of Valsalva (LSOV) does present a technical challenge. When the anomalous RCA arises below the left sino-tubular ridge, it usually has a slit-like ostium and takes an acute rightward course that precludes the coaxial engagement of most of the currently available guiding catheters. Due to the lack of an adequate backup force for the guiding catheter, it is usually difficult to perform PCI successfully, especially when a totally occluded RCA lesion is present. Previous case reports have described successful PCI procedures with different kinds of guiding catheters such as Amplatz left (AL) or XB catheters. However, only one or two cases of each have been reported.2-7 In this study, we report a novel technique for PCI for an anomalous RCA arising from the LSOV below the left sino-tubular ridge by using a manually modified Judkins left (JL) guiding catheter.
MATERIALS AND METHODS
From January 2001 to January 2014, six patients who underwent PCI for an anomalous RCA arising from the LSOV were included in this study. All these patients had provided informed consent before PCI procedures were performed. When an anomalous RCA arising from the LSOV was noted after diagnostic coronary angiography, and particularly when it was located below the left sino-tubular ridge, this novel technique was used for PCI if the lesion was critical or totally occluded. The conventional JL tip orientation is modified by manually bending at the point approximately 1.25 cm from the distal tip 90° vertically toward the operator for 5 to 10 seconds without using any additional heat source. The operator can repeat this simple modifying process till the distal tip orientation is near vertical to its original plane. This simple procedure changed the distal tip orientation to fit the acute anterior-rightward course of the anomalous RCA (Figure 1). The operator introduced this modified JL catheter and advanced it to the ascending aorta either transfemorally or transradially. Even though the catheter tip might be positioned slightly less vertical after introduction into the aorta, we found that this distal tip orientation could engage the anomalous RCA very coaxially. It should be emphasized that there is no need to use a heat source to shape the distal catheter tip. Because we inspected the distal tip of the JL catheter after PCI procedure, and noted that it could still retain an anterior-rightward orientation.
Figure 1.
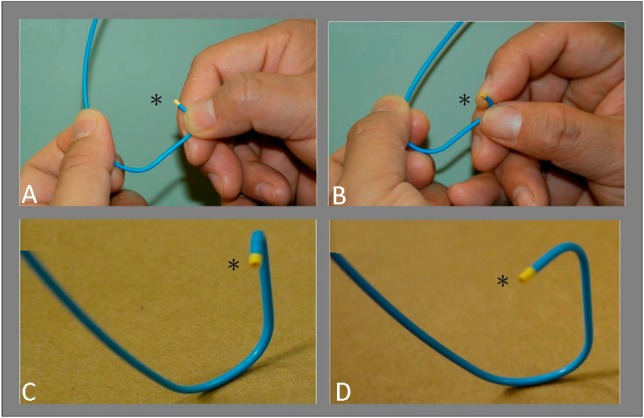
The technique of modifying the distal tip of Judkins catheter. (A) Conventional Judkins left (JL) catheter. (B) Bending the distal tip (*) of the JL catheter 90° vertically. (C) Right-anterior-oblique (RAO) view of the modified JL catheter. (D) Left-anterior-oblique (LAO) view of the modified JL catheter.
The ostium of an anomalous RCA arising from the LSOV is usually located anteriorly next to the ostium of the left main (LM) artery. The ostium of the LM artery can therefore be used as a useful landmark. When the modified JL catheter tip was close to the LM ostium, the operator rotated the catheter clockwise and advanced it to engage the anomalous RCA orifice coaxially without any difficulty. The operator can gently push the catheter further, so the distal tip will advance deeper and the secondary curve of the JL catheter will contact the aortic wall. Using this method, the modified catheter could provide strong active coaxial support for further interventions as shown in an illustrative case (Figure 2).
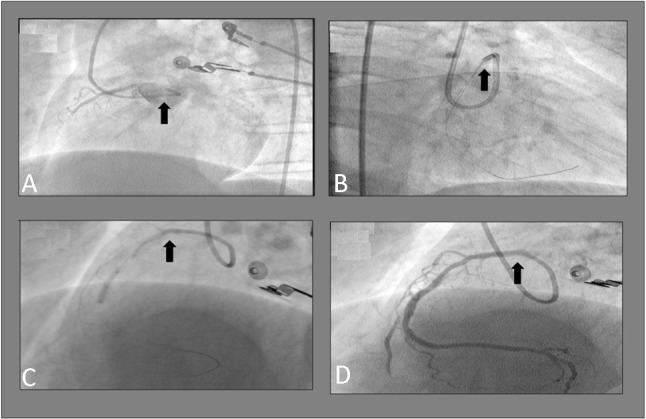
Figure 2.
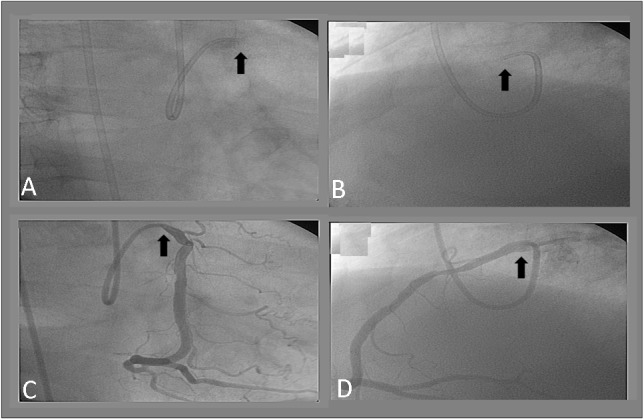
Illustrative case. (A) Coronary angiogram, Right-anterior-oblique (RAO) view before contrast medium injection shows the distal tip (arrow) orientation of the judkins left (JL) catheter. (B) Coronary angiogram, Left-anterior-oblique (LAO) view before contrast medium injection shows the distal tip (arrow) orientation of the JL catheter. (C) Coronary angiogram, RAO view of the anomalous right coronary artery (RCA) demonstrates coaxial engagement (arrow) and the secondary curve of the JL catheter making contact against the aortic wall. (D) Coronary angiogram, LAO view of the anomalous RCA demonstrates coaxial engagement (arrow) and the secondary curve of the JL catheter making contact against the aortic wall.
RESULTS
Our first successful PCI for an anomalous RCA from the LSOV using this technique was performed in 2001. Including this case, we have now performed a total of six successful PCI procedures for an anomalous RCA arising from the LSOV using this technique (Table 1). Four of these six patients were male, with a mean age of 63 ± 16.7 years (range 37 to 85 years). The culprit lesions of five cases were located at the middle segment of the RCA, and the other was located at the distal RCA. Two cases (case 3 and 6) presented with acute inferior wall ST-segment-elevation myocardial infarction (STEMI) and underwent primary angioplasty. The other four cases presented with recent myocardial infarction (two patients) or angina pectoris (two patients) and underwent elective angioplasty. The procedures for three of the cases were performed via a transfemoral approach, and the other three cases were performed via a transradial approach. All of the cases were successfully treated with stent implantation. Among the six cases, the first (case 1) had a totally occluded lesion at the middle segment of the RCA, and every possible guiding catheter including AL, JL, judkins right (JR) and Voda catheters had failed. This patient was finally stented successfully using our novel technique of modifying the distal tip of the JL guiding catheter (Figure 3). We used conventional AL guiding catheters for PCI for the following two cases at the beginning of the procedure (case 2 and 3), and were again unsuccessful due to inadequate guiding catheter support. After using our novel technique, the anomalous RCA could be engaged coaxially with strong active guiding catheter support, and the stenting procedures were then performed easily and successfully (Figure 4 and Figure 5). After the first three successful cases, PCI for the next two elective cases (case 4 and 5) used this novel technique at the beginning of the PCI procedures, and both procedures were performed successfully without any difficulty. The last case (case 6) presented with acute STEMI and underwent primary PCI. The first operator was inexperienced and had great difficulty in gaining adequate support of the guiding catheter. The PCI procedure was successful when an experienced operator used this novel modified technique. However, the door-to-balloon time was longer than 90 minutes.
Table 1. Clinical summary of 6 cases undergoing successful percutaneous coronary intervention (PCI) of the anomalous right coronary artery (RCA) arising from the left sinus of Valsalva (LSOV) .
| Case no. | Age | Sex | Intervention date | Initial presentation | Occlusion site/severity | Access route | Size and type of guiding catheter | Diagnostic angiography duration (mins) | Intervention duration (mins) | Total procedure duration (mins) |
| 1 | 46 | Male | 2001/9/5 | Recent inf wall MI | Middle RCA 100% | Femoral artery | 6F JL | 22 | 67 | 89 |
| 2 | 56 | Male | 2002/4/12 | Recent inf wall MI | Middle RCA 100% | Radial artery | 6F JL | 8 | 43 | 51 |
| 3 | 37 | Male | 2009/12/29 | Acute inf wall MI | Middle RCA 100% | Femoral artery | 6F JL | 65 | 18 | 83 |
| 4 | 85 | Female | 2011/5/3 | Angina pectoris | Middle RCA 80% | Radial artery | 5F JL | 11 | 45 | 56 |
| 5 | 79 | Female | 2013/1/22 | Angina pectoris | Distal RCA 99% | Radial artery | 6F JL | 9 | 39 | 48 |
| 6 | 75 | Male | 2013/4/15 | Acute inf wall MI | Middle RCA 100% | Femoral artery | 6F JL | 44 | 52 | 96 |
Inf, inferior; JL, Judkins-left catheter; MI, myocardial infarction; RCA, right coronary artery.
Figure 3.
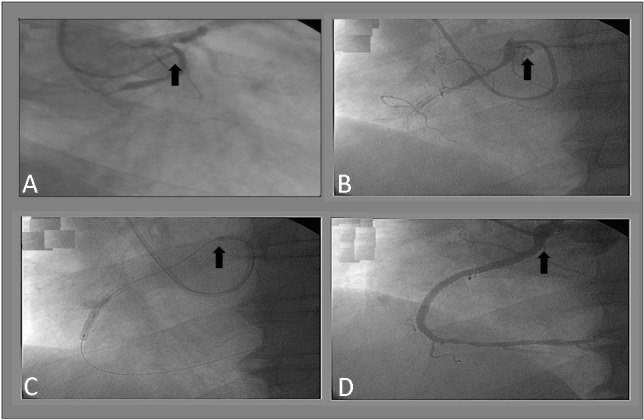
Case 1 coronary angiograms. (A) Amplatz left (AL) guiding catheter (arrow) failed to engage the anomalous right coronary artery (RCA) coaxially (RAO view). (B) The modified Judkins left (JL) catheter (arrow) engaged the anomalous RCA coaxially (LAO view). (C) With the secondary curve making contact with the aortic wall, PCI was successfully performed with this modified JL guiding catheter (LAO view). (D) The final angiogram showed successful PCI (LAO view).
Figure 4.
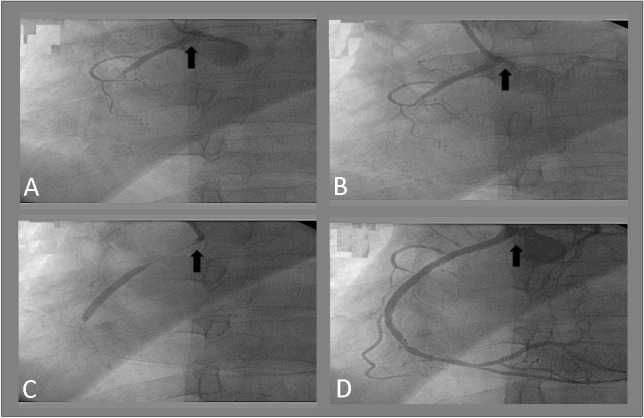
Case 2 coronary angiograms. (A) The right coronary artery (RCA) was engaged with a conventional Judkins left (JL) catheter (arrow). (B) The guidewire was unable to cross the lesion due to the non-coaxially engaged JL guiding catheter (arrow) with inadequate guiding catheter support (LAO view). (C) After modifying the JL catheter, engagement was coaxial (arrow) and the guidewire successfully crossed the totally occluded lesion (LAO view). (D) The final angiogram showed successful PCI (LAO view).
Figure 5.
Case 3 coronary angiograms. (A) A conventional Judkins left (JL) guiding catheter (arrow) failed to engage the right coronary artery (RCA) for this patient with acute STEMI undergoing primary PCI (LAO view). (B) Using the novel technique by modifying the distal tip orientation of the JL guiding catheter (arrow), the engagement was coaxial (RAO view). (C) Deep intubation of the RCA with the modified JL guiding catheter (arrow) providing strong support (LAO view). (D) The final angiogram showed successful primary PCI results. Arrow indicates the coaxial engagement (LAO view).
The diagnostic angiography duration (defined as the period from the beginning of the procedure to baseline RCA angiography) ranged from 8 to 65 minutes (median 16.5 minutes). The intervention duration (defined as the period from the baseline RCA angiography to the end of the PCI procedure) ranged from 18 to 103 minutes (median 44 minutes). The total procedure time ranged from 51 to 139 minutes (median 69.5 minutes). The diameter of the guiding catheter was 6 French in five patients, and 5 French in one patient. There were no procedure-related complications, including catheter-induced coronary ostial dissection, catheter fracture or kinked catheter.
DISCUSSION
The incidence of an anomalous RCA arising from the LSOV is very low, ranging from 0.02-0.17% of diagnostic coronary angiograms.1 Although the incidence rate is very low, any experienced interventional cardiologist who performs many PCI procedures may well expect to encounter at least one case of an anomalous RCA arising from the LSOV. Interventional cardiologists therefore need to be cognizant of a PCI technique for an anomalous RCA arising from the LSOV, especially when these cases present with acute inferior STEMI. In this study, case 6 presented with acute STEMI, and the operator was inexperienced in handling such cases and took a considerable amount of time to engage the anomalous RCA, which is crucial for primary PCI. Therefore, it is very important for interventional cardiologists to be aware of the possibility of an anomalous RCA, and to know how to treat these patients successfully. Knowledge of the congenital variations of the RCA orifice can help in the selection of an appropriate guiding catheter for coronary intervention. If the orifice of the anomalous RCA arising from the left aortic root is above the sino-tubular ridge, PCI can be performed without too much difficulty with an AL-type guiding catheter.8,9 However, if the ostium of the anomalous RCA is below the sino-tubular ridge within the LSOV, the anomalous RCA will take an acute rightward course. In this situation, poor guiding catheter support can be expected due to the non-coaxial engagement of most currently available guiding catheters. Moreover, because the backup force of a guiding catheter always depends on the secondary curve of the guiding catheter sitting stably on the contralateral aortic wall, most currently available guiding catheters are unable to sit in a stable position for cases with an anomalous RCA arising from the LSOV. Whenever an anomalous RCA arising from the LSOV is identified, our novel technique can be used to gain strong guiding catheter support, which is the key factor of success for these cases. We believe any certified interventional cardiologist will learn this technique quickly after performing one or two cases. The most important concept of our technique is modifying the distal tip orientation of the JL catheter to fit the anterior-rightward course of the anomalous RCA. One useful tip to successfully engage the anomalous RCA is always using the ostium of the LM artery as a landmark. The operator advances this modified catheter to the level close to LM ostium and then rotates clockwise and advances it. This simple maneuver will engage the anomalous RCA orifice coaxially. In our series, we were able to engage every anomalous RCA using our novel technique without any difficulty. We also observed that once the operator had learned the technique, the procedure could be performed in a similar manner to a routine PCI procedure with an acceptable procedural time. Most importantly, all of our cases were treated successfully with no procedural complications.
Several single-case or two-case reports of PCI for an anomalous RCA arising from the LSOV have been reported. Among these reports, AL, JL, XB and Voda guiding catheters were used successfully; however, none of these catheters were specifically designed for this situation.2-6 The Leya catheter, a modified AL guiding catheter with a right-angled tip, was designed specifically for PCI for an anomalous RCA from the LSOV.7 However, we only had a total of six cases of an anomalous RCA from the LSOV during the past 13 years, with an incidence of less than 0.1%. The likelihood of using a Leya catheter is therefore very low, and this catheter is not available in many catheterization laboratories. On the other hand, the JL guiding catheter is universally available in every catheterization laboratory. Treating these rare but difficult cases is therefore more practical using our novel technique.
There are other methods for improving guiding catheter support such as the deep-seated guiding catheter technique, using a large-caliber guiding catheter (such as 7 or 8 French), the buddy wire technique, or using an over-the-wire balloon system, as well as new instruments such as a ST01TM catheter (Terumo, Japan) or a GuideLinerTM catheter (Vascular Solutions, Inc., Minnesota, USA) with the mother-and-child technique.10 Using a stiffer wire or buddy wire can provide more support, however this may push the tip of the guiding catheter away from the RCA ostium and preclude a good quality of angiography. When using our novel technique, 6 French or 5 French JL catheter is recommended. Compared to a 7 French catheter, 6 French or 5 French catheters can be shaped more easily and the chances of catheter-related complications are reduced when deep intubation is needed. In our experience, we have never needed to use mother-and-child, buddy wire, or anchoring balloon techniques because our method provides excellent guiding catheter support. Previous reports of successful PCI for an anomalous RCA arising from the LSOV are limited to one or two cases, and, to the best of our knowledge, the current study is the largest reported series to date. Our proposed technique is easy and safe, and uses a catheter that is universally available. This technique can be used via either a transfemoral or transradial approach and even in an emergency situation such as acute STEMI. We strongly suggest that when a rare case of an anomalous RCA arising from the LSOV is encountered, this novel technique is the best option.
CONCLUSIONS
The key determinant for successful PCI of an anomalous RCA arising from the LSOV is adequate guiding catheter support by coaxial engagement of the RCA. Our novel technique is simple, safe and effective with a 100% procedure success rate for PCI for an anomalous RCA arising from the LSOV in this study.
DISCLOSURE STATEMENT
All the authors report no financial relationships or conflicts of interest regarding the content herein.
REFERENCES
- 1.Kimbiris D, Iskandrian AS, Segal BL. Anomalous aortic origin of coronary arteries. Circulation. 1978;58:606–615. doi: 10.1161/01.cir.58.4.606. [DOI] [PubMed] [Google Scholar]
- 2.Sarkar K, Sharma SK, Kini AS. Catheter selection for coronary angiography and intervention in anomalous right coronary arteries. J Interv Cardiol. 2009;22:234–239. doi: 10.1111/j.1540-8183.2009.00463.x. [DOI] [PubMed] [Google Scholar]
- 3.Azzarelli S, Amico F, Giacoppo M, et al. Primary coronary angioplasty in a patient with anomalous origin of the right coronary artery from the left sinus of Valsalva. J Cardiovasc Med. 2007;8:943–945. doi: 10.2459/JCM.0b013e328012b0e7. [DOI] [PubMed] [Google Scholar]
- 4.Cohen MG, Tolleson TR, Peter RH, et al. Successful percutaneous coronary intervention with stent implantation in anomalous right coronary arteries arising from the left sinus of Valsalva:a report of two cases. Catheter Cardiovasc Interv. 2002;55:105–108. doi: 10.1002/ccd.10062. [DOI] [PubMed] [Google Scholar]
- 5.Praharaj TK, Ray G. Percutaneous transluminal coronary angioplasty with stenting of anomalous right coronary artery originating from left sinus of Valsalva using the Voda guiding catheter:a report of two cases. Indian Heart J. 2001;53:79–82. [PubMed] [Google Scholar]
- 6.Chakraborty B, Chan CN, Tan A. Percutaneous transluminal coronary angioplasty of an anomalous right coronary artery arising from a separate ostium in the left sinus of Valsalva. A case report. Angiology. 1995;46:629–632. doi: 10.1177/000331979504600711. [DOI] [PubMed] [Google Scholar]
- 7.Qayyum U, Leya F, Steen L, et al. New catheter design for cannulation of the anomalous right coronary artery arising from the left sinus of Valsalva. Catheter Cardiovasc Interv. 2003;60:382–388. doi: 10.1002/ccd.10650. [DOI] [PubMed] [Google Scholar]
- 8.Charney R, Spindola-Franco H, Grose R. Coronary angioplasty of anomalous right coronary arteries. Cathet Cardiovasc Diagn. 1993;29:233–235. doi: 10.1002/ccd.1810290312. [DOI] [PubMed] [Google Scholar]
- 9.Ceyhan C, Tekten T, Onbasili AO. Primary percutaneous coronary intervention of anomalous origin of right coronary artery above the left sinus of Valsalva in a case with acute myocardial infarction. Coronary anomalies and myocardial infarction. J Cardiovasc Imaging. 2004;20:293–297. doi: 10.1023/b:caim.0000041946.61659.a6. [DOI] [PubMed] [Google Scholar]
- 10.Yumoto K, Aoki H, Shirai Y, et al. Successful coronary stenting in anomalous right coronary artery by using an inner catheter with mother and child technique under multislice CT guidance. Cardiovasc Interv Ther. 2013;28:106–110. doi: 10.1007/s12928-012-0124-1. [DOI] [PubMed] [Google Scholar]