

Abstract
Background
Previous clinical trials have demonstrated the impact of blocking upstream renin-angiotensin-axis with angiotensin converting enzyme inhibitors (ACEIs) on arterial stiffness as evaluated by pulse-wave velocity (PWV). We ran a meta-analysis to evaluate the anti-stiffness effect of powerful downstream angiotensin receptor blockades (ARBs) on peripheral and central arterial stiffness (brachial to ankle, ba-PWV; carotid to femoral, cf-PWV, respectively), using a systematic review to assess the clinical arterial stiffness issues.
Methods
For our study, we searched the PubMed and Cochrane Library databases from inception to June 2013, targeting randomized controlled trials. ARBs along with other antihypertensive agents, ACEIs, calcium channel blockers (CCBs), beta-blockers and diuretics were evaluated to ascertain their comparable effect on ba-PWV and cf-PWV, respectively. A meta-analysis was conducted utilizing the fixed or random effect of the weighted mean change difference between the ARB and comparator groups, depending on the I2 statistic heterogeneity measurement.
Results
In 2 trials treating patients with ARBs (n = 30), the ARBs insignificantly reduced levels of ba-PWV (pooled mean change difference -188, 95% CI -687, 311, p = 0.24 with significant heterogeneity) as compared to other hypertensive agents (ACEIs and CCBs, n = 77). Interestingly, ARBs (n = 20) had a superior capacity to reduce levels of ba-PWV than CCBs (n = 20) in single study results (mean change difference -400, 95% CI -477, -322, p < 0.05). In 7 trials which included a total of 653 patients, treatment with ARBs (n = 308) also insignificantly reduced cf-PWV (pool mean change difference -0.197, 95% CI -0.54, 0.14, p = 0.218) as compared to other anti-hypertensive agents.
Conclusions
Our data suggested that ARBs had a similar effect as other anti-hypertensive agents in reducing ba-PWV and cf-PWV. Upon systematic review, the renin-angiotensin-axis system mechanism seems more significant than the direct vessel dilatation system in anti-arterial stiffness mechanism.
Keywords: Angiotension receptor blockage, Arterial stiffness, Meta-analysis, Systematic review
INTRODUCTION
Arterial stiffness assessment demonstrates the relationship between the stiffness severity of the central carotid and abdominal aorta and higher cardiovascular event rates in many high-risk1-3 and community-based populations.4-6 Several methods were evaluated in clinical trials, and pulse wave velocity (PWV) was considered the gold standard non-invasive method.7 The PWV method was measured by two sites: the waveform travelling distance was divided by the spending time as manifested by the tonometric method.8 Peripheral muscular ba-PWV was assessed by two sites, between the brachial artery and the ankle anterior tibial artery;9 meanwhile, central aortic cf-PWV was evaluated by two sites between the carotid artery and the femoral artery.10
In prior decades, arterial stiffness was strongly related to age, blood pressure and renal function impairment, and aggressive anti-hypertensive treatment was beneficial to arterial resilience beyond blood pressure control.11 The renin-angiotensin-system (RAS) involved the arterial stiffness mechanism and provided the treatment target.12 The angiotensin converting enzyme inhibitors (ACEIs) was the leading choice in anti-stiffness hypertensive treatment strategies.13 However, the adverse coughing effect and the modest blood pressure lowering effect limited the prescription frequency and raised the angiotensin receptor blockades (ARBs), of which there was greater usage than ACEIs in Asian hypertensive patients. The comparative effect of ARB and other hypertensive agents including ACEIs and calcium channel blockers (CCBs) on arterial stiffness is inconclusive in peripheral muscular ba-PWV and central aortic cf-PWV.
In this meta-analysis, we investigated the effect of ARBs compared with other anti-hypertensive agents in two primary ways: to ACEIs and CCBs in peripheral muscular arterial stiffness (ba-PWV), and to ACEIs, CCBs, beta-blockers and diuretics in central arterial stiffness (cf-PWV).
As a result of the meta-analysis, we further briefly reviewed the clinical application of PWV to add the substantial benefit of predicting the outcome in renal disease, coronary arterial disease, heart failure and metabolic syndrome, and the important treatment role of ARB in arterial anti-stiffness mechanism.
METHODS
Search strategy
We reviewed the existing literature primarily researched through PubMed and Cochrane publications. We use the mesh terms and key words “arterial stiffness”, “arterial elasticity”, “pulse wave velocity”, “central hemodynamic blood pressure”, “clinical trial”, “randomized trial”, “hypertensive” and “medical treatment”. We also expanded the search from just reference lists of relevant papers, to avoid missing articles that might be obtained through an internet search. The searching procedure was performed repeatedly by two experienced cardiovascular physicians working independently. We only searching the articles published in English and human-related data (Figure 1).
Figure 1.

Flow diagram. ARBs,angiotensinreceptorblockades; RAAS, renin-angiotensin-aldosterone system.
Inclusion and exclusion criteria
The studies which were eligible to be included in the meta-analysis were the following: Hypertension with arterial stiffness PWV data and treatment with ARBs. Comparable studies and crossover studies were all included but only randomized clinical trials were optimal. Single ARB usage was better, but combination with other anti-hypertensive agents was also included. The articles were divided into peripheral and central groups in terms of ba-PWV and cf-PWV data. We excluded patients with chronic kidney disease, pulmonary hypertension, ocular hypertension, stroke (cerebral infarction), cardiovascular surgery, liver transplantation, endothelial function, pregnancy, invasive measurement, no PWV data, duplicated papers, exercise, diet treatment, Chinese herb medicine, ginseng, ambulatory blood pressure, and not currently taking ARBs medicine. The summary articles were listed in Table 1 and Table 2.
Table 1. ARBs′ effects on peripheral ba-PWV.
| First author year, country | Population | No | Mean age | F (%) | Treatment (ARB) N | Control group N | Followed up duration | Study method | Masking method | Modality | Before PWV (cm/s) | After PWV/mean difference (cm/s) | Reference |
| Futoshi, 200515 | Hypertension | 31 | 59 ± 5 | 14 (45%) | Valsartan (V) N = 10 | 40 weeks | Randomized comparable | single | ba-PWV volume-plethysmographic, Colin, Japan | 1853 ± 107 | 1615 ± 103 | Eur J Clin Pharmcol 2005;61:353-9 | |
| Japan | Perindopril (P)N = 11 | 1818 ± 137 | 1613 ± 94 | ||||||||||
| Combine (V + P) N = 10 | 1865 ± 101 | 1496 ± 93 | |||||||||||
| Takami, 20039 | Elderly male hypertension | 76 | 71 ± 3 | 0 (%) | ValsartanN = 20 | 12 weeks | Randomized comparable | single | ba-PWV volume-plethysmographic, Colin, Japan | 409 ± 90 | Hypertens Res 2003;26:609-14 | ||
| Japan | TemocaprilN = 20 | 281 ± 99 | |||||||||||
| CilnidipineN = 20 | 209 ± 82 | ||||||||||||
| Nifedipine-CRN = 16 | 9 ± 146 |
ARB, angiotensin receptor blockade; ba-, brachial to ankle; PWV, pulse wave velocity.
Table 2. ARBs′ effects on central cf-PWV.
| First author, year, country | Population | No | Mean age, F (%) | Treatment (ARB) N | Control group N | Followed up duration | Studymethod | Maskingmethod | Modality | Before PWV (m/s) | After PWV (m/s) | SBP | DBP | SBP change | DBP change | Reference |
| Mahmud-A 200223 Ireland | Hypertension | 11 | 57 ± 36 (55%) | Losartan 50 mg, 11 | 4 weeks | Randomize crossover | Single blind | cf-PWV pressure transducer, (complior) and AI (sphygmoCor device) | 11.75 ± 0.64 | 10.35 ± 0.55 | 164 | 94 | 9 | 7 | AJH 2001;15: 1092-5 | |
| hydrochlorthiazide 12.5 mg, 11 | 11.7 ± 0 | 11.52 ± 0 | 167 | 94 | 11 | 5 | ||||||||||
| Mahmud-B 200210 Ireland | Hypertension | 12 | 49 ± 116 (50%) | Valsartan 160 mg, 12 | 4 weeks | Randomize crossover | Single blind | cf-PWV pressure transducer, (complior) | 11.07 ± 0 | 10.04 ± 0 | 157 | 96 | 23 | 10 | AJH 2002;15: 321-5 | |
| Captopril 100 mg, 12 | 11.07 ± 0 | 10.04 ± 0 | 157 | 98 | 19 | 6 | ||||||||||
| Ali 200924 UK | Hypertension | 15 | 65 ± 90 (0%) | Irbesartan 300 mg, 15 | 12 weeks | Randomize crossover | Double blind | cf-PWV pressure transducer, (complior) | 15.1 ± 5 | 13.3 ± 2.6 | 162 | 98 | 28 | 20 | Vascular Health and Risk Management 2009;5:587-92 | |
| Lisinopril 20 mg, 15 | 15.1 ± 5 | 14 ± 4.7 | 162 | 98 | 17 | 14 | ||||||||||
| Vitale 201125 Italy | Newly-diagnosed hypertension | 65 | 52 ± 1223 (35%) | Irbesartan 150 mg (thiazide base), 34 | 8 weeks | Randomize parallel | cf-PWV pressure transducer, (complior) | 11.3 ± 2.2 | 10.06 ± 1.58 | 154 | 99 | 27 | 18 | Internal Journal of Cardiology 2012;155:279-84 | ||
| Nebivolol 5mg (beta-blocker),(thiazide base), 31 | 11.5 ± 1.6 | 10.58 ± 1.27 | 156 | 103 | 29 | 19 | ||||||||||
| Rajzer 200326 Poland | Hypertension | 118 | 53 ± 964 (54%) | Losartan 100 mg, 24 | 24 weeks | Prospective parallel | Open | cf-PWV pressure transducer, (complior) | 11.23 ± 1.67 | 9.55 ± 1.32 | 155 | 91 | 30 | 7 | AJH 2003;16:439-44 | |
| Quinapril 20 mg, 37 | 11.23 ± 1.67 | 10.53 ± 1.05 | 149 | 94 | 27 | 9 | ||||||||||
| Amlodipine 10 mg, 38 | 11.23 ± 1.67 | 10.54 ± 1.67 | 154 | 97 | 41 | 11 | ||||||||||
| Boutouyrie 201027 France | Hypertension | 393 | 57 ± 9.9183 (47%) | Valsartan 160 mg (amlodipine base), 193 | 24 weeks | Randomize parallel | Double blind | cf-PWV pressure transducer, (complior) | 12.5 ± 3 | 11.52 ± 0.18 | 158 | 91 | 13 | 6 | Hypertension 2010;55:1314-22 | |
| Atenolol 100 mg (beta-blocker) (amlodipine base), 200 | 11.9 ± 10.8 | 10.95 ± 0.17 | 156 | 92 | 12 | 7 | ||||||||||
| Rehman 200728 Malaysia | Hypertension | 39 | 52NR | Losartan 50 mg, 19 | 24 weeks | Randomize parallel | Double blind | cf-PWV pressure transducer, (complior) | 12 ± 1.75 | 11.17 ± 1.19 | 151 | 94 | 14 | 8 | AJH 2007;20: 184-9 | |
| Perindopril 4 mg, 20 | 11 ± 1.69 | 10.43 ± 1.22 | 152 | 92 | 18 | 9 |
ARB, angiotensin receptor blockade; cf-, carotid to femoral; DBP, diastolic blood pressure; F, female; PWV, pulse wave velocity; SBP, systolic blood pressure.
Statistical analysis
We included randomized clinical trials, which also incorporated parallel-group and cross-over design. The articles were combined in the same meta-analysis with a standard recommendation.14 We calculate the absolute difference of mean changes in ba-PWV and cf-PWV and standard errors by the inverse variance method. Also, unpaired t-test was performed in parallel-groups studies. We ran a sensitivity analysis to measure the contribution of every study to the pooled treatment effect by excluding each study at one time. We then re-ran the meta-analysis model to assess the treatment effect for the remaining studies. A p-value < 0.05 was considered significant. Heterogeneity was calculated by I2 method and essential heterogeneity was defined as > 50%. Random-effects model was performed if I2 value > 50%. Fixed-effects model was then used when studies did not reveal significant heterogeneity. Stata version 11 was performed for the data analysis.
RESULTS
Epidemiology of patients and studies
We comprehensively reviewed 9 randomized control trials with 760 participants from 2002 to 2010 (Table 1 and Table 2). The search identified 182 potentially eligible studies of which 152 studies were excluded by review of title and abstract. Full articles of the remaining 30 studies were collected and evaluated. Finally, 9 studies met our inclusion criteria. In the two trials that evaluated the effects of ARBs on ba-PWV, one compared ARBs with ACEIs or a combination of both drugs; the other compared it with ACEIs and CCBs. In the seven trials that assessed these effects on cf-PWV, four of them compared ARBs with ACEIs, two compared it with beta-blockers, and one compared it with thiazides. The basic demographics of patients were mostly similar between the study groups, with the exception of two studies that focused solely on elderly males (Takami, 2003; Ali, 2009). The mean patient age ranged from 49 to 61 years, and the mean follow-up duration ranged from 4 to 40 weeks.
Ba-PWV measurement
In 2 trials including a total of 107 patients, no significant difference in peripheral ba-PWV reduction was observed with ARBs (n = 30, pooled mean change difference -188, 95% CI -687, 311, p = 0.25 with significant heterogeneity) than other hypertensive agents (ACEIs and CCBs, n = 77). ARBs (n = 20) had comparatively superior effects on peripheral stiffness than CCBs (n = 20) in one study results (mean change difference -400, 95% CI -477, -322, p < 0.05) (Figure 2).
Figure 2.
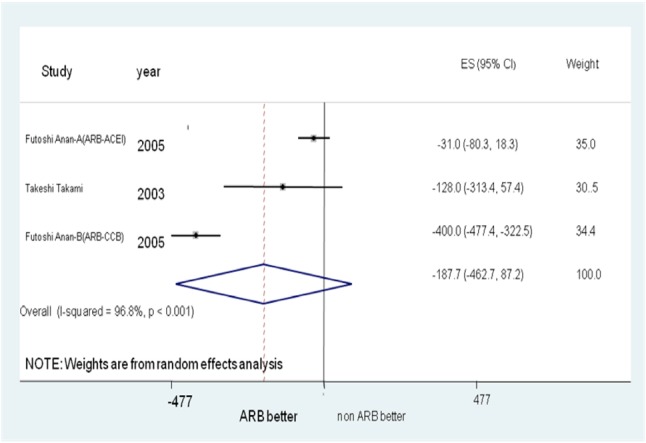
Forest plot of ba-PWV. ba-PWV, Brachial to ankle pulse wave velocity.
Cf-PWV measurement
In 7 trials including a total of 653 patients, treatment with ARBs (n = 308) also insignificantly reduced central cf-PWV (pool mean change difference -0.19, 95% CI -0.54, 0.14, p = 0.21 with insignificant heterogeneity) than other hypertensive agents (ACEIs, CCBs, beta-blockers, and thiazides) (Figure 3).
Figure 3.
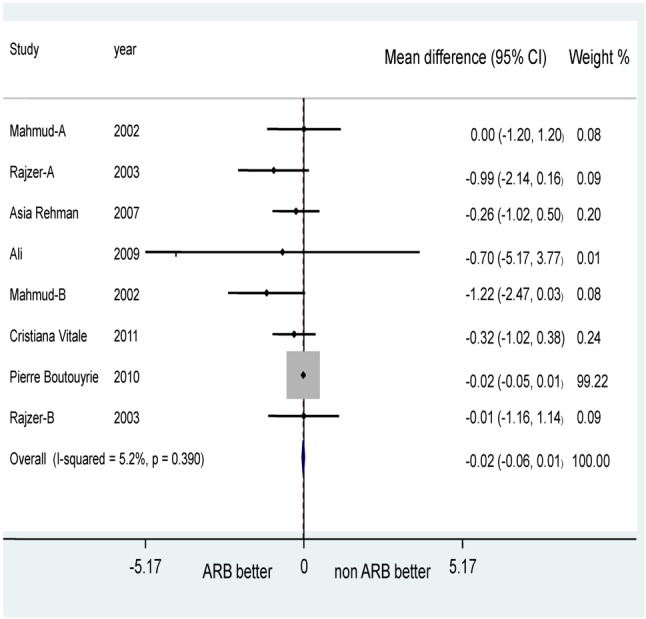
Forest plot of cf-PWV.
Heterogeneity
Heterogeneity was calculated by use of the I2 method and essential heterogeneity was defined as > 50%. The random-effects model was performed if I2 value > 50%, and the fixed-effects model was used when studies did not reveal significant heterogeneity.
Risk of bias and publication bias
Risk of bias and study quality was evaluated for all of the articles using the Jadad scoring system16 (Table 3). The Jadad score in our study was no more than 2, suggesting a less than excellent study quality. The effect sizes of PWV were plotted against the standard errors through use of Forest plotting (Figure 2 and Figure 3). Publication bias was assessed by the funnel plot method (Supplementary figure).
Table 3. Quality check-up with Jadad scores.
| Risk of bias estimation | ||||||
| Adequate sequence generation | Allocation concealment | Blinding | Adequate report on loss to followed-up | Free of other resources of bias | Jadad score | |
| Mahmud-A23, 2002 | Yes | No | single | No | Yes | 1 |
| Mahmud-B10, 2002 | Yes | No | single | No | Yes | 1 |
| Ali24, 2009 | Yes | NR | double | No | Yes | 2 |
| Vitale25, 2011 | Yes | No | NR | No | Yes | 1 |
| Rajzer26, 2003 | Yes | No | open | No | Yes | 1 |
| Boutouyrie27, 2010 | Yes | No | double | No | Yes | 2 |
| Rehman28, 2007 | Yes | NR | double | No | Yes | 2 |
| Deary33, 2002 | Yes | NR | double | No | Yes | 2 |
| Mackenzie34, 2009 | Yes | NR | double | No | Yes | 2 |
| Futoshi15, 2005 | Yes | No | single | No | Yes | 1 |
| Takami9, 2003 | Yes | No | single | No | Yes | 1 |
Supplementary Figure.
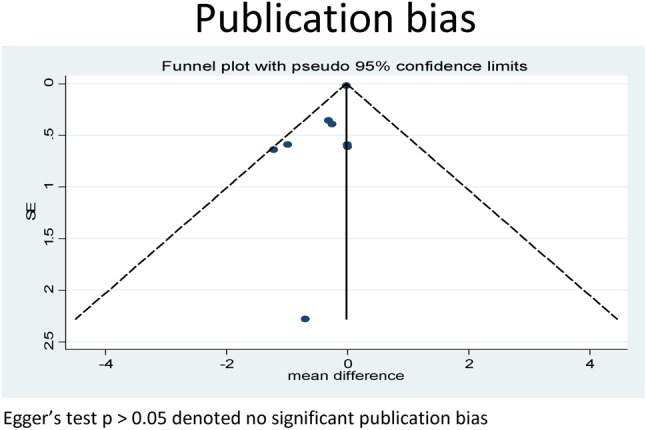
Funnel plot of cf-PWV.
DISCUSSION AND SYSTEMATIC REVIEW
Clinical pulse pressure, arterial stiffness, and PWV
Enthusiasm in the medical community contributing to primary prevention for cardiovascular disease and risk measurement in asymptomatic people had fueled substantial discussion about preventive research. By 1999, peripheral pulse pressure (PP) had become a better predictor for coronary heart disease according to the Framingham Heart Study, and a better predictor for risk of heart failure in the elderly study rather than conventional peripheral arterial blood pressure (BP) measurement.17,18 However, many factors other than PP such as heart rate, cardiac contractility, and venous pressure can influence the value of PP to predict clinical cardiovascular events.19 Apart from the limitation of PP, central pressure is more strongly associated with vascular disease and outcome than brachial pressure.20 Some investigators have suggested a surrogate measure of large artery stiffness with the stroke volume/pulse pressure, which had been shown to be the better prediction marker of all-cause and cardiovascular mortality. But other authors considered the stroke volume/pulse pressure poorly correlated with central PWV.21 Central aortic PWV was a strong predictor of future cardiovascular events and all-cause mortality.22 Meanwhile, central aortic PWV was considered the gold standard method for assessing aortic stiffness and subclinical target organ damage as well.7
PWV and coronary heart disease
Despite the decline of the coronary heart disease (CHD) rate in the United States and major European countries, heart attack event prevention remains a challenge.29 Optimal medical treatment and aggressive revascularization strategy have substantially reduced the mortality rate of acute myocardial infarction and coronary heart disease. Additionally, proper identification of the target population for primary prevention has led to more timely and appropriate intervention treatment. Arterial artery stiffness measured by PWV implying subclinical atherosclerosis had been performed in asymptomatic individuals to predict CHD,30 and to potentially help foresee severe cardiovascular events in patients that underwent percutaneous coronary interventions.31
PWV and chronic renal disease
Cardiovascular events were the leading complication risk in patient with chronic kidney disease (CKD). Vascular dysfunction, comprising carotid intima-medial thickness and aortic arterial stiffness, was the major predictor for fatal and non-fatal cardiovascular events and PWV through the aorta to femoral artery, and was the only arterial index independently associated with cardiovascular outcome in patients with CKD.32 The possible mechanisms associated with higher rate of cardiovascular events in patients with chronic renal disease were disturbed calcium-phosphate metabolism, arterial calcification, anemia and increased systemic inflammatory changes.32 Even in end-stage renal disease (ESRD), Tetsuo et al. found the aortic PWV was a significant predictor for all-cause and cardiovascular mortality after adjusting for other risk factors such as age, gender, C-reactive protein, hematocrit, body mass index and diabetes.35 In a previous study, aging, hypertensive risk factor and renal disease were the most frequently cited impacts on arterial stiffness that often coexisted with decreased carotid distensibility and the presence of calcification and plaques.11
PWV and metabolic syndrome, obesity and diabetes
Metabolic syndrome encompassing dyslipidemia, high blood pressure, increased waist circumference, and impaired glucose metabolism linked to cardiovascular events such as acute myocardial infarction, heart failure, and stroke and death have become the world’s leading heath burden.36 However, the magnitude of metabolic syndrome (which can vary with the number of components of the syndrome presentation) may not predict metabolic risk in an African man in the United States.37 Alternatively, vascular compliance assessment with arterial stiffness may be the appropriate avenue of evaluation, focusing on cardio-metabolic syndrome.38 By 1997, Lehmann disclosed that diabetic patients show increased arterial stiffness in young age compared to a non-diabetic group. Arterial stiffness was considered to be an important and robust predictor for cardiovascular events for glucose intolerance and diabetes patients.3,39 At least one investigator suggested an association between obesity and arterial stiffness in young and older adults.40 However, the long-term effect of weight-reduction in cardiovascular event was ambiguous in secondary prevention and thus necessitates additional investigation in the future.41
PWV and preserved EF heart failure
Heart failure, a major and virtually skyrocketing public health problem of epidemic proportion, comprising cardiac abnormal contraction, unmet oxygen demand of peripheral tissue, pulmonary congestion and volume overload, was the leading cause of epidemic hospitalization and associated with approximately 45% of post-discharge mortality and readmission within 3 months.42,43 Despite drug and device interventional treatment, the clinical outcome of heart failure has remained suboptimal.44 Many investigators have agreed that the increasing percentage of preserved ejection fraction heart failure within an aging society has become an important epidemic problem now and in the near future.43 In earlier Japanese and European studies, arterial stiffness was considered a risk factor for both atherosclerosis and diastolic heart failure.45,46 A coupling of ventricular-arterial stiffness encompassed mechanical interaction of the systemic and coronary flow balance, regulating endothelial function and smooth muscle tone.47,48 B-type natriuretic peptide (BNP) is comparable to N-terminal pro-BNP in predicting heart function in compensated renal dysfunction.49 A treatment-guide by B-type BNP and heart echocardiography parameter has already proven useful in clinical practice.50,51 However, the combination of arterial stiffness, cardiac contractility with diastolic function and biochemical marker may offer additional prediction power for cardiovascular events in clinical settings.48,52
Pulse pressure, PWV in hypertension pharmacology and therapy mechanism
Arterial stiffness was the consequence of progressive arterial dilatation and degeneration of the arterial wall along with aging process and increasing systolic pressure. Furthermore, peripheral brachial systolic pressure underestimated the rising in systolic pressure in the aorta and left ventricle, thus conferring differing vessel dilatation effect of anti-hypertensive drugs.53 In addition to the effects of advancing years and hypertensive status on arterial wall elasticity, some evidence of atherosclerosis has further amplified these hardening effects in the distributed compliance model of arterial circulation, thus implying statin utility in elevated pulse pressure and arterial stiffness.54 In previous studies, anti-hypertensive agents were divided into two categories: one group involved interference with the RAS system, endothelial NO synthase system and the α-adducin systems; the other group related to the aging process with elastin, collagen and telomere length, both supplying the protective effect in terms of gene polymorphisms.12,13 In clinical treatment of arterial stiffness, the effect of vasodilator drugs could directly relax smooth muscle in the arterial medial and indirectly respond to the dilatation and increased compliance of small muscular arteries.55 The treatment strategy in hypertension with congestive heart failure aims to increase arterial compliance, and lower pressure afterload with pulse pressure and reverse progression of the left ventricular and arterial wall hypertrophy.55 Based on the HOPE and LIFE trials, inhibitors of the renin-angiotensin system may carry the better protective effect in minimizing cardiovascular outcome. Results of the REASON and CAFÉ trials suggested that beta-blocker (atenolol) usage was inferior to perindopril, indapamide and amlodipine in terms of central blood pressure lowering effect.56
ARBs comparing with ACEIs
ACEIs have played the upstream role in the renin-angiotensin-axis system, and ARBs have taken the downstream part. Previous studies demonstrated ACEIs had a beneficial arterial anti-stiffness effect which was independent of blood pressure change.57 The mechanism of how ACEIs improve arterial compliance was based on the ability to suppress angiotensin II and increase bradykinin. ACEIs also inhibited the nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and reduced oxidative stress in the vascular tissue, implying a cardiovascular protective effect.58 However, bradykinin tended to induce cough as an adverse effect and made the use of ACEIs intolerable in many Asian patients. Some investigators considered the endothelium dysfunction by ARBs, but this was not a consensus opinion.59 In terms of balancing an effective anti-stiffness impact with a blood pressure lowering effect, our results showed that ARBs binding to angiotensin II type 1 receptor were similar to ACEIs.
ARBs comparing with CCBs
In an earlier study, despite the fact that CCBs (amlodipine) had a significant central blood pressure lowering effect with ARBs (valsartan), the anti-stiffness effect was no different between the two groups, and the CCBs coincided with a high prevalence of peripheral edema in post-menopausal women.60 This suggested that the ARBs anti-stiffness effect was independent of central hemodynamic change. In our results, we calculated that the direct comparison effect in meta-analysis in peripheral muscular arterial stiffness and ARBs was better than CCBs in single study data. CCBs was the direct vasodilatation agent which effected central hemodynamic change, ARBs played a similar role in the renin-angiotensin-axis system leading to vessel wall anti-hypertrophic change.38
STRENGTH AND LIMITATIONS
The strength of our meta-analysis is its incorporated robust literature search including randomized clinical trials. However, after exclusions were applied, few studies were included in our final meta-analysis project (less than 10 articles). Second, most of the articles we referenced were lower quality publications intended for small audiences, where there was less double-blinding and fewer long-term followed-up results. Third, we were only able to include published data. Fourth, we worked with the study-level data rather than the patient-level data, and may approximate to biased measurement upon meta-analyses. In addition, we tried to contact the authors of the underlying articles for missing data, but received no replies to our requests.
CONCLUSIONS
Our data implied ARBs were similar to other anti-hypertensive agents in reducing ba-PWV and cf-PWV. Upon systematic review, the renin-angiotensin-axis system mechanism seemed to play a more important role than direct vessel dilatation system in anti-arterial stiffness mechanism, and ARBs improved arterial resilience independent of central hemodynamic change.
REFERENCES
- 1.Gerard GM, London JB, Pannier B, et al. Arterial wave reflections and survival in end-stage renal failure. Hypertension. 2001;38:434–438. doi: 10.1161/01.hyp.38.3.434. [DOI] [PubMed] [Google Scholar]
- 2.Blacher J, Guerin AP, Pannier B, et al. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension. 2001;38:938–942. doi: 10.1161/hy1001.096358. [DOI] [PubMed] [Google Scholar]
- 3.Cruickshank K, Riste L, Anderson SG, et al. Aortic pulse-wave elocity and its relationship to mortality in diabetes and glucose intolerance: an integrated index of vascular function? Circulation. 2002;106:2085–2090. doi: 10.1161/01.cir.0000033824.02722.f7. [DOI] [PubMed] [Google Scholar]
- 4.Willum-Hansen T, Staessen JA, Torp-Pedersen C, et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation. 2006;113:664–670. doi: 10.1161/CIRCULATIONAHA.105.579342. [DOI] [PubMed] [Google Scholar]
- 5.Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study of atherosclerosis: objectives and design. Am J Epidemiol. 2002;156:871–881. doi: 10.1093/aje/kwf113. [DOI] [PubMed] [Google Scholar]
- 6.Sutton-Tyrrell K, Najjar SS, Boudreau RM, et al. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation. 2005;111:3384–3390. doi: 10.1161/CIRCULATIONAHA.104.483628. [DOI] [PubMed] [Google Scholar]
- 7.Kullo IJ, Malik AR. Arterial ultrasonography and tonometry as adjuncts to cardiovascular risk stratification. J Am Coll Cardiol. 2007;49:1413–1426. doi: 10.1016/j.jacc.2006.11.039. [DOI] [PubMed] [Google Scholar]
- 8.Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588–2605. doi: 10.1093/eurheartj/ehl254. [DOI] [PubMed] [Google Scholar]
- 9.Takami T, Shigemasa M. Efficacy of various antihypertensive agents as evaluated by indices of vascular stiffness in elderly hypertensive patients. Hypertens Res. 2003;26:609–614. doi: 10.1291/hypres.26.609. [DOI] [PubMed] [Google Scholar]
- 10.Mahmud A, Feely J. Effect of angiotensin ii receptor blockade on arterial stiffness: beyond blood pressure reduction. Am J Hypertens. 2002;15:1092–1095. doi: 10.1016/s0895-7061(02)02982-5. [DOI] [PubMed] [Google Scholar]
- 11.Benetos A, Waeber B, Izzo J, et al. Influence of age, risk factors, and cardiovascular and renal disease on arterial stiffness: clinical applications. Am J Hypertens. 2002;15:1101–1108. doi: 10.1016/s0895-7061(02)03029-7. [DOI] [PubMed] [Google Scholar]
- 12.Van Bortel LM, Struijker-Boudier HA, Safar ME. Pulse pressure, arterial stiffness, and drug treatment of hypertension. Hypertension. 2001;38:914–921. doi: 10.1161/hy1001.095773. [DOI] [PubMed] [Google Scholar]
- 13.Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107:2864–2869. doi: 10.1161/01.CIR.0000069826.36125.B4. [DOI] [PubMed] [Google Scholar]
- 14.Elbourne DR, Altaman DG, Higgins JP, et al. Meta-analysis invloving cross-over trials: methodological issues. Int J Epidemiol. 2002;31:140–149. doi: 10.1093/ije/31.1.140. [DOI] [PubMed] [Google Scholar]
- 15.Futoshi A, Takahashi N, Ooie T, et al. Effects of valsartan and perindopril combination therapy on left ventricular hypertrophy and aortic arterial stiffness in patients with essential hypertension. Eur J Clin Pharmacol. 2005;61:353–359. doi: 10.1007/s00228-005-0931-8. [DOI] [PubMed] [Google Scholar]
- 16.Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clinical Trials. 1996;17:1–12. doi: 10.1016/0197-2456(95)00134-4. [DOI] [PubMed] [Google Scholar]
- 17.Franklin SS, Khan SA, Wong ND, et al. Is pulse pressure useful in predicting risk for coronary heart disease? The Framingham Heart Study. Circulation. 1999;100:354–360. doi: 10.1161/01.cir.100.4.354. [DOI] [PubMed] [Google Scholar]
- 18.Staessen JA, Thijs L, Fagard R, et al. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. JAMA. 1999;282:539–546. doi: 10.1001/jama.282.6.539. [DOI] [PubMed] [Google Scholar]
- 19.Boutouyrie P, Troeano AI, Asmar R, et al. Aortic stiffness is an independent predictor of primary coronary events in Hypertensive patients. Hypertension. 2002;39:10–15. doi: 10.1161/hy0102.099031. [DOI] [PubMed] [Google Scholar]
- 20.Roman MJ, Devereux RB, Kizer JR, et al. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the Strong Heart Study. Hypertension. 2007;50:197–203. doi: 10.1161/HYPERTENSIONAHA.107.089078. [DOI] [PubMed] [Google Scholar]
- 21.Woodman RJ, Kingwell BA, Beilin LJ, et al. Assessment of central and peripheral arterial stiffness: studies indicating the need to use a combination of techniques. Am J Hypertens. 2005;18:249–260. doi: 10.1016/j.amjhyper.2004.08.038. [DOI] [PubMed] [Google Scholar]
- 22.Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction ot cardiovascular events and all-cause mortality with arterial stiffness. J Am Coll Cardiol. 2010;55:1318–1327. doi: 10.1016/j.jacc.2009.10.061. [DOI] [PubMed] [Google Scholar]
- 23.Mahmud A, Feely J. Reduction in arterial stiffness with angiotensin II antagonist is comparable with and additive to ACE inhibition. Am J Hypertens. 2002;15:321–325. doi: 10.1016/s0895-7061(01)02313-5. [DOI] [PubMed] [Google Scholar]
- 24.Ali K, Rajkumar C, Fantin F, et al. Irbesartan improves arterial compliance more than lisinopril. Vasc Health Risk Manag. 2009;5:587–592. doi: 10.2147/vhrm.s5690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vitale C, Marazzi G, Iellamo F, et al. Effects of nebivolol or irbesartan in combination with hydrochlorothiazide on vascular functions in newly-diagnosed hypertensive patients: the NINFE study. International Journal of Cardiology. 2012;155:279–284. doi: 10.1016/j.ijcard.2011.10.099. [DOI] [PubMed] [Google Scholar]
- 26.Rajzer M, Klocek M, Kawecka-Jaszcz K. Effect of amlodipine, quinapril, and losartan on pulse wave velocity and plasma collagen markers in patients with mild-to-moderate arterial hypertension. Am J Hypertens. 2003;16:439–444. doi: 10.1016/s0895-7061(03)00052-9. [DOI] [PubMed] [Google Scholar]
- 27.Boutouyrie P, Achouba A, Trunet P, et al. Amlodipine-valsartan combination decreases central systolic blood pressure more effectively than the amlodipine-atenolol combination: the EXPLOR study. Hypertension. 2010;55:1314–1322. doi: 10.1161/HYPERTENSIONAHA.109.148999. [DOI] [PubMed] [Google Scholar]
- 28.Rehman A, Ismail SB, Naing L, et al. Reduction in arterial stiffness with angiotensin II antagonism and converting enzyme inhibition. A comparative study among malay hypertensive subjects with a known genetic profile. Am J Hypertens. 2007;20:184–189. doi: 10.1016/j.amjhyper.2006.07.015. [DOI] [PubMed] [Google Scholar]
- 29.Wilson PW, D'Agostino RB, Levy D, et al. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97:1837–1847. doi: 10.1161/01.cir.97.18.1837. [DOI] [PubMed] [Google Scholar]
- 30.Weber T, Auer J, O’rourke MF, et al. Increased arterial wave reflections predict severe cardiovascular events in patients undergping percutaneous coronry interventions. Eur Heart J. 2005;26:2657–2663. doi: 10.1093/eurheartj/ehi504. [DOI] [PubMed] [Google Scholar]
- 31.Simon A, Chironi G, Levenson J. Comparative performance of subclinical atherosclerosis tests in predicting coronary heart disease in asymptomatic individuals. Eur Heart J. 2007;28:2967–2971. doi: 10.1093/eurheartj/ehm487. [DOI] [PubMed] [Google Scholar]
- 32.Zoungas S, Cameron JD, Kerr PG, et al. Association of carotid intima-medial thickness and indices of arterial stiffness with cardiovascular disease outcomes in CKD. Am J Kidney Dis. 2007;50:622–630. doi: 10.1053/j.ajkd.2007.07.012. [DOI] [PubMed] [Google Scholar]
- 33.Deary AJ, Schumann AL, Murfet H, et al. Influence of drugs and gender on the arterial pulse wave and natriuretic peptide secretion in untreated patients with essential hypertension. Clin Sci (Lond) 2002;103:493–499. doi: 10.1042/cs1030493. [DOI] [PubMed] [Google Scholar]
- 34.Mackenzie IS, McEniery CM, Dhakam Z, et al. Comparison of the effects of antihypertensive agents on central blood pressure and arterial stiffness in isolated systolic hypertension. Hypertension. 2009;54:409–413. doi: 10.1161/HYPERTENSIONAHA.109.133801. [DOI] [PubMed] [Google Scholar]
- 35.Shoji T, Emoto M, Shinohara K, et al. Diabetes mellitus, aortic stiffness, and cardiovascular mortality in end-stage renal disease. J Am Soc Nephro. 2001;12:2117–2124. doi: 10.1681/ASN.V12102117. [DOI] [PubMed] [Google Scholar]
- 36.Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 37.Ukegbu UJ, Castillo DC, Knight MG, et al. Metabolic syndrome does not detect metabolic risk in African men living in the U.S. Diabetes Care. 2011;34:2297–2299. doi: 10.2337/dc11-1055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ganne S, Winer N. Vascular compliance in the cardiometabolic syndrome. J Cardiometab Syndr. 2008;3:35–39. doi: 10.1111/j.1559-4572.2008.05630.x. [DOI] [PubMed] [Google Scholar]
- 39.Cernes RZ, Zimlichman R, Shargorodsky M. Arterial elasticity in cardiovascular disease: focus on hypertension, metabolic syndrome and diabetes. Ady Cardiol. 2008;45:65–81. doi: 10.1159/000115188. [DOI] [PubMed] [Google Scholar]
- 40.Wildman RP, Mackey RH, Bostom A, et al. Measure of obesity are associated with vascular stiffness in young and older adults. Hypertension. 2003;42:468–473. doi: 10.1161/01.HYP.0000090360.78539.CD. [DOI] [PubMed] [Google Scholar]
- 41.Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. J Am Coll Cardiol. 2009;53:1925–1932. doi: 10.1016/j.jacc.2008.12.068. [DOI] [PubMed] [Google Scholar]
- 42.Writing Group M, Lloyd-Jones D, Adams RJ, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. doi: 10.1161/CIRCULATIONAHA.109.192667. [DOI] [PubMed] [Google Scholar]
- 43.Tang WH, Francis GS. The year in heart failure. J Am Coll Cardiol. 2008;52:1671–1678. doi: 10.1016/j.jacc.2008.08.026. [DOI] [PubMed] [Google Scholar]
- 44.Bueno H, Ross JS, Wang Y, et al. Trends in length of stay and short-term outcomes among medicare patients hospitalized for heart faiure, 1993-2006. JAMA. 2010;303:2141–2147. doi: 10.1001/jama.2010.748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Yambe M, Tomiyama H, Hirayama Y, et al. Arterial stiffness as a possible risk factor for both atherosclerosis and diastolic heart failure. Hypertens Res. 2004;27:625–631. doi: 10.1291/hypres.27.625. [DOI] [PubMed] [Google Scholar]
- 46.Kang S, Fan HM, Li J, et al. Relationship of arterial stiffness and early mild diastolic heart failure in general middle and aged population. Eur Heart J. 2010;31:2799–2807. doi: 10.1093/eurheartj/ehq296. [DOI] [PubMed] [Google Scholar]
- 47.Kass DA. Ventricular arterial stiffening: integrating the pathophysiology. Hypertension. 2005;46:185–193. doi: 10.1161/01.HYP.0000168053.34306.d4. [DOI] [PubMed] [Google Scholar]
- 48.Marti CN, Gheorghiade M, Kalogeropoulos AP, et al. Endothelial dysfunction, arterial stiffness, and heart failure. J Am Coll Cardiol. 2012;60:1455–1469. doi: 10.1016/j.jacc.2011.11.082. [DOI] [PubMed] [Google Scholar]
- 49.Luchner A, Hengstenberg C, Löwel H, et al. Effect of compensated renal dysfunction on approved heart failure markers:direct comparison of brain natriuretic peptide (BNP) and N-terminal pro-BNP. Hypertension. 2005;46:118–123. doi: 10.1161/01.HYP.0000170140.36633.8f. [DOI] [PubMed] [Google Scholar]
- 50.Lester SJ, Tajik AJ, Nishimura RA, et al. Unlocking the mysteries of diastolic function: deciphering the Rosetta Stone 10 years later. J Am Coll Cardiol. 2008;51:679–689. doi: 10.1016/j.jacc.2007.09.061. [DOI] [PubMed] [Google Scholar]
- 51.Maisel AS, Daniels LB. Breathing not properly 10 years later. J Am Coll Cardiol. 2012;60:277–282. doi: 10.1016/j.jacc.2012.03.057. [DOI] [PubMed] [Google Scholar]
- 52.Goto T, Ohte N, Fukuta H, et al. Relationship between effective arterial elastance, total vascular resistance, and augmentation index at the ascending aorta and left ventricular diastolic function in older women. Circ. 2013;77:123–129. doi: 10.1253/circj.cj-12-0733. [DOI] [PubMed] [Google Scholar]
- 53.O'Rourke M. Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension. Hypertension. 1990;15:339–347. doi: 10.1161/01.hyp.15.4.339. [DOI] [PubMed] [Google Scholar]
- 54.Dart AM, Kingwell BA. Pulse pressure - a review of mechanisms and clinical relevance. J Am Coll Cardiol. 2001;37:975–984. doi: 10.1016/s0735-1097(01)01108-1. [DOI] [PubMed] [Google Scholar]
- 55.Laurent S, Kingwell B, Bank A, et al. Clinical applications of arterial stiffness: therapeutics and pharmacology. Am J Hypertens. 2002;15:453–458. doi: 10.1016/s0895-7061(01)02329-9. [DOI] [PubMed] [Google Scholar]
- 56.Agabiti-Rosei E, Mancia G, O'Rourke MF, et al. Central blood pressure measurements and antihypertensive therapy: a consensus document. Hypertension. 2007;50:154–160. doi: 10.1161/HYPERTENSIONAHA.107.090068. [DOI] [PubMed] [Google Scholar]
- 57.Mallareddy M PC, Peixoto AJ. Effect of angiotension-converting enzyme inhibitors on arterial stiffness in hypertension: systemic review and meta-analysis. J Clin Hypertens (Greenwich) 2006;8:398–403. doi: 10.1111/j.1076-7460.2006.05418.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Shahin Y, Khan JA, Chetter I. Angiotensin converting enzyme inhibitors effect on arterial stiffness and wave reflections: a meta-analysis and meta-regression of randomised controlled trials. Atherosclerosis. 2012;221:18–33. doi: 10.1016/j.atherosclerosis.2011.12.005. [DOI] [PubMed] [Google Scholar]
- 59.Watanabe T, Barker TA, Berk BC. Angiotensin II and the endothelium: diverse signals and effects. Hypertension. 2005;45:163–169. doi: 10.1161/01.HYP.0000153321.13792.b9. [DOI] [PubMed] [Google Scholar]
- 60.Hayoz D, Zappe DH, Meyer MA, et al. Changes in aortic pulse wave velocity in hypertensive postmenopausal women: comparison between a calcium channel blocker vs angiotensin receptor blocker regimen. J Clin Hypertens (Greenwich) 2012;14:773–778. doi: 10.1111/jch.12004. [DOI] [PMC free article] [PubMed] [Google Scholar]