

Abstract
Colonoscopy is an important screening and therapeutic modality for colorectal cancer. Unlike other screening tests, colonoscopy is dependent on pre-procedure bowel preparation. If the bowel preparation is poor, significant pathology may be missed. Many factors are known to improve bowel preparation. This review will highlight those factors that may optimize the bowel preparation, including choice of bowel preparation, grading or scoring of the bowel preparation, special factors that influence preparation, and diet prior to colonoscopy that affects bowel preparation. The aim of the review is to offer suggestions and guide endoscopists on how to optimize the bowel preparation for the patients undergoing colonoscopy.
Keywords: Colonoscopy, bowel preparation, scales, diet
Introduction
Colorectal cancer is one of the top three neoplasms afflicting the global patient population. Over the past decade, colonoscopy has become a heavily used screening test to prevent the development of colon cancer. Although other noninvasive tests are available, such as fecal immunochemical test, fecal occult blood test and CT colonography, colonoscopy offers the advantage of being a diagnostic and therapeutic tool at the same time [1].
The quality of bowel preparation impacts the success of colonoscopy. Optimal bowel preparation leads to decreased procedure time, increased polyp detection, and subsequent increased adenoma detection rate, a popular quality indicator for colonoscopy. A suboptimal bowel preparation can result in small or flat lesions being missed [2], shortened surveillance times [3], significant impediment in progression of colonoscope, increased likelihood of complications, and more sedatives and analgesics being required [4]. Therefore, an enormous amount of research has been performed on improving bowel preparations prior to colonoscopy. In a joint statement in 2006 by the American Society of Colon and Rectal Cancer (ASCRS), American Society of Gastrointestinal Endoscopy (ASGE), and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), a colonoscopy preparation should have the following properties: inexpensive; cleanse the bowels rapidly; and not cause significant patient discomfort or electrolyte imbalances [5]. This is similar to the guidelines published by the European Society of Gastrointestinal Endoscopy [6]. Today, there are essentially three factors that are essential for a good bowel preparation: safe, palatable, and efficacious [1].
Bowel preparation is generally safe for most patients but can be detrimental for patients with co-morbidities if the wrong preparation is utilized on the wrong patient. An example is Fleet Phospho-Soda or magnesium citrate used in patients with renal failure. At present, polyethylene glycol (PEG) is the only recommended bowel preparation in patients with renal failure [7]. As for efficacy, poor bowel preparations have health and financial implications. Suboptimal bowel preparation leads to increased repeat colonoscopy procedures which increases overall health care costs and risk to the patients [8]. Many factors impact efficacy, including variability in the preparation due to patient compliance with the preparation instructions provided, health literacy, and socioeconomic status. Other various confounding factors like use of narcotics, chronic constipation and diabetes, and timing of bowel preparation in relation to colonoscopy also impact efficacy of the preparation. To improve efficacy, splitting the dose of the bowel preparation has become increasingly popular [6,9-12].
An adequate bowel preparation is a combination of multiple factors and essential to identifying and removing pre-cancerous lesions in the colon and rectum. In this review, we will focus on the factors that may optimize bowel preparation prior to colonoscopy, including description of bowel preparation agents, grading scales for bowel preparations, factors that may influence the efficacy of the bowel preparation, impact of restrictive diets on preparation, and timing of preparation with colonoscopy.
Optimizing bowel preparation agents
Many bowel preparations agents are available today. These agents are shown in detail in Table 1. Bowel preparation agents may be classified by multiple ways, including volume administered (low-volume versus high-volume), osmolarity (isotonic versus hypoosmotic versus hyperosmotic), or main active ingredient (PEG, sodium picosulfate, sodium phosphate [NaP]).
Table 1.
Types of colon cleansing agents available
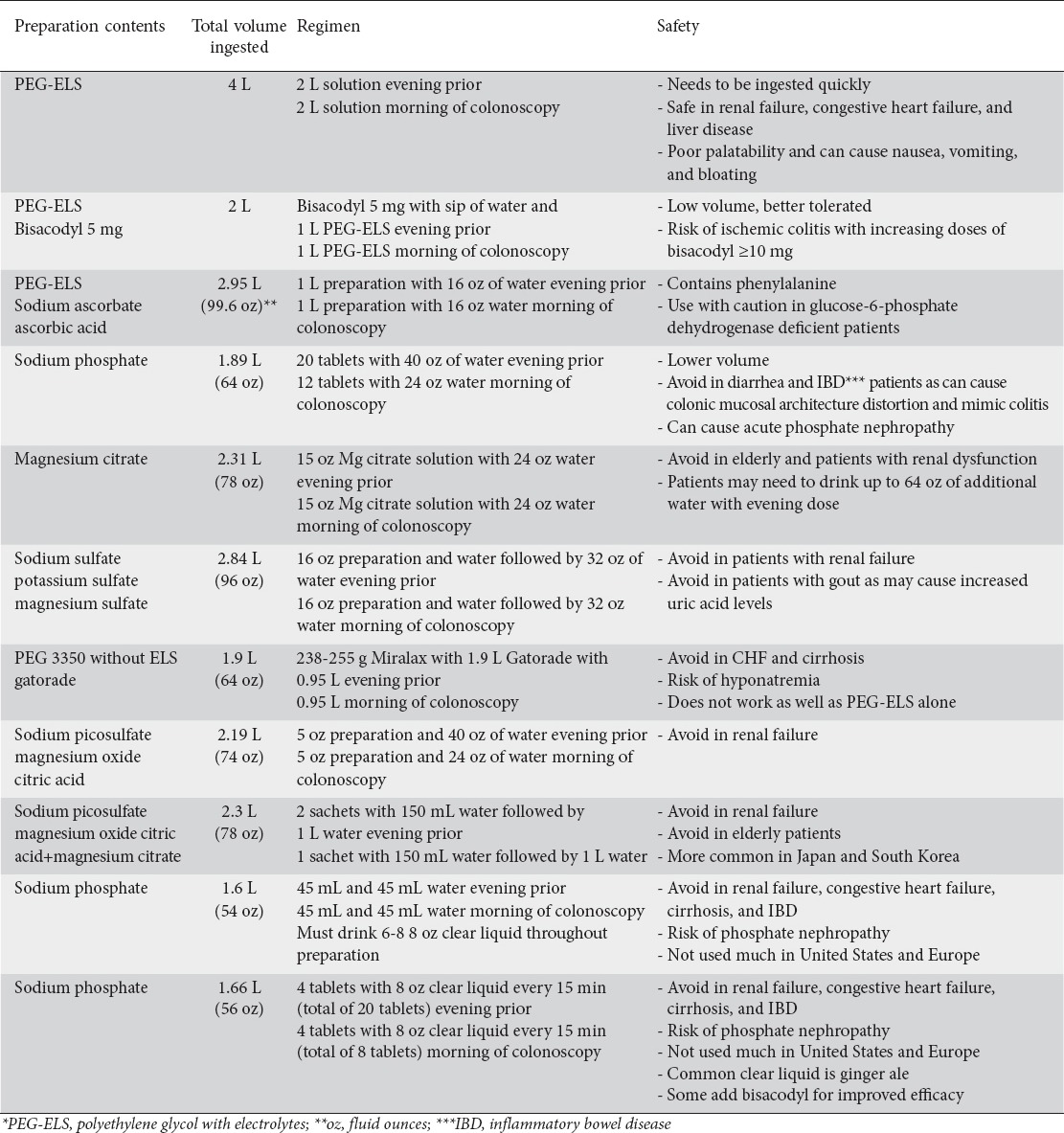
Over the past decade, the volume of preparation seems to be the focus as patients complain about drinking an entire 4 L or 1 gallon of PEG with electrolytes (PEG-ELS). This volume issue has been challenging and has led to the use of low-volume (2 L) of PEG-ELS with an adjunct, such as senna, magnesium citrate, magnesium sulfate, magnesium oxide, mannitol, enema, olive oil, castor oil, bisacodyl, cisapride, domperidone, ascorbic acid, alverine citrate, lubiprostone, simethicone, probiotic, metoclopramide, mosapride, simethicone, or sodium ascorbate [1,13-16]. Large-scale randomized controlled trials have compared low-volume preparations to 4 L PEG-ELS with little to no head-to-head comparisons. A meta-analysis of six randomized controlled trials comparing low-volume PEG-ELS and bisacodyl to 4 L PEG-ELS showed no difference in efficacy but did reveal improvement in side effects [15]. Another meta-analysis of nine randomized controlled trials comparing low-volume PEG-ELS and ascorbic acid to traditional 4 L PEG-ELS demonstrated similar bowel preparation efficacy but no difference in side effects [16]. Furthermore, most of these adjunctive agents have not gained widespread use due to side effects. Bisacodyl can cause abdominal cramping [17] and ischemic colitis, especially dose of ≥ 10 mg [18,19]. Magnesium citrate is contraindicated in patients with renal failure with isolated case reports of inducing ischemic colitis [20]. Low-volume PEG-ELS with ascorbic acid cannot be administered to patients with glucose-6-phosphate deficiency as the accompanying ascorbic acid can induce hemolysis [21]. Besides volume, osmolarity also plays a major role.
PEG-based preparations are isosmotic, being osmotically balanced with non-fermentable electrolytes. PEG-based solutions have an excellent safety profile with the minimal electrolyte shifts, making it favorable to be used most commonly. PEG-ELS is the favored colonic preparation for inflammatory bowel disease patients as it does not induce histologic changes in the colonic mucosa [22]. However, approximately 15% of the patient population being administered PEG-ELS are unable to tolerate it due to unpleasant taste, large volume, or nausea [23]. PEG-ELS solutions have a large volume that can predispose the patient to abdominal fullness and cramping, aspiration pneumonia in rare instances, colitis, pancreatitis [24], and Mallory-Weiss tears from forceful vomiting [25]. Therefore, other preparations have been conceived to limit the negative qualities of PEG-ELS. Miralax (PEG 3350 without electrolytes) (Merck, New Jersey, USA) mixed with Gatorade (a sports drink) (PepsiCo, Illinois, USA) is one of these preparations that is commonly used.
Miralax-Gatorade is a bowel preparation with a lesser volume. However, when PEG 3350 powder without electrolytes (Miralax) is mixed with 64 ounces of a sports drink (Gatorade), the result is a hypoosmotic solution [26]. At this time, despite its common use around the United States, this solution is not Food and Drug Administration (FDA)-approved for colonoscopy preparation. Furthermore, a meta-analysis of five randomized controlled trials in 2014 revealed the Miralax-Gatorade preparation was inferior to PEG-ELS in satisfactory bowel preparations (OR 0.65; 95% CI: 0.43-0.98; P=0.04) [27]. In addition, isolated cases of hyponatremia have been reported, likely due to electrolyte shifts with the hypoosmotic solution [28-32]. Given these electrolyte shifts, the Miralax-Gatorade preparation is not recommended for patients with congestive heart failure or advanced liver disease with ascites [33]. Due to these issues with electrolyte shifts and hyponatremia, hyperosmotic agents have been studied as well.
Hyperosmotic agents include NaP, magnesium citrate, sodium sulfate, and sodium picosulfate. These preparations act by osmotically increasing intraluminal fluid content resulting in fecal material evacuation. The NaP comes in tablet form with many tablets ingested with ample amount of water or as a solution. It is extremely important that patients maintain adequate hydration while undergoing NaP bowel preparation. The NaP bowel regimen has been shown to be an effective bowel preparation when compared to 4 L PEG-ELS regimen, except for more nausea and vomiting [34]. The safety profile of NaP limits its widespread use. Most notable but rare side effect associated with its use is acute phosphate nephropathy, which is deposition of calcium phosphate crystals in the renal tubules resulting in irreversible kidney damage [35-39]. Acute phosphate nephropathy can occur even in patients with normal renal function and also in patients with preexisting renal disease, especially those who are using diuretics or angiotensin converting enzyme inhibitors. Therefore, this preparation should be avoided in these patients [36,40]. The FDA in the United States has issued a black box warning pertaining to the risk of acute phosphate nephropathy associated with NaP in elderly and patients with preexisting renal disease. Other adverse effects include hyperphosphatemia, electrolyte imbalances, colonic mucosal damage, and grand-mal seizures [41]. Although NaP solution is limited in the United States and Europe [1,5,6], it is still used in Japan and other countries [42-44]. Due to the potential adverse effects of NaP, other sodium derivatives have been evaluated, such as sodium sulfate and sodium picosulfate.
Sodium sulfate is taken as a split-dose with 16 fluid ounces being taken the night before and 16 fluid ounces taken in the morning of the procedure. The total volume of sodium sulfate preparation is 96 fluid ounces, which is mildly less than 4 L PEG-ELS. Unlike Miralax-Gatorade solution, sodium sulfate has not been shown to cause major electrolyte abnormalities or intravascular fluid shifts. However, sodium sulfate has not been fully evaluated in patients with significant co-morbidities including congestive heart failure, renal disease, or cirrhosis. Therefore, it is best to avoid this preparation in these patients [45]. On the other hand, the newest agent in the hyperosmotic category is a combination of sodium picosulfate and magnesium oxide, a lower volume preparation of a total of 74 fluid ounces. Sodium picosulfate acts as a stimulant laxative while magnesium oxide acts as an osmotic agent with resulting cathartic effect on the bowels. Efficacy in terms of bowel cleansing is comparable to NaP and PEG-ELS [46,47]. Electrolyte abnormalities (severe hyponatremia) have been reported in the elderly with use of sodium picosulfate and should be used very cautiously in this patient population [48,49].
Finally, magnesium citrate is a relatively inexpensive osmotic laxative but data on its efficacy as a standalone colonoscopy preparation is lacking. Although not a routine first-line bowel preparation in Europe and the United States, it is commonly used in Japan, South Korea, and other countries as a single bowel preparation agent or combined with sodium picosulfate [50-52]. It should be avoided in patients with renal insufficiency as magnesium is excreted through the kidney. Resulting magnesium toxicity may induce bradycardia, hypotension, nausea, and death [53].
Many options are available for bowel preparations. As mentioned, each option has its positives and negatives and must be customized for the specific patient population to optimize the quality of bowel preparation. For the most part, PEG-ELS seems to be the most utilized based upon fewest population restrictions due to its isosmotic properties and overall efficacy. However, the large volume is difficult for patients to drink, leading to increased use of low-volume bowel preparations. The days of one size fits all bowel preparation, although easy, are likely over. In Japan, it is not uncommon to add a prokinetic agent to the bowel preparation in an effort to minimize abdominal discomfort [54,55]. However, due to side effects of most prokinetic agents and lack of convincing evidence on its benefit to the patient and preparation, this practice is not recommended in the United States and Europe at this time [5,6]. Bowel preparation agent choice must be adjusted to the patient to ensure optimization of the preparation. Whichever preparation the patient and physician decide to use, it is extremely important to effectively evaluate or grade the bowel preparation to improve the quality of preparation over time. By implementing a grading system, bowel preparations may be altered by continuous quality improvement to optimize the efficacy.
Optimizing bowel preparation quality by grading
Bowel cleanliness is an important determinant of a quality of colonoscopy and surveillance interval. This may be the deciding factor in scheduling an interval colonoscopy after an average risk screening colonoscopy for colorectal cancer. Appropriate documentation of the bowel preparation quality for the colonoscopy benefits patients, other endoscopists, and insurance providers when follow-up interval needs to be earlier than expected. Although many scales are evident in the literature (Table 2) [56-63], three validated bowel preparation scoring or grading systems are most commonly used: Aronchick, Ottawa, and the Boston Bowel Preparation scales.
Table 2.
Bowel preparation scales in the literature
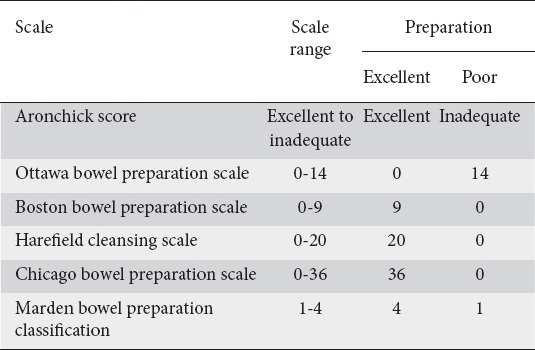
The Aronchick scale is likely the most used but most subjective bowel preparation grading scale [56]. This scale grades the adequacy of colonic cleansing by describing mucosal visualization of the colon on a five parameter scale: excellent, good, fair, poor, or inadequate. Based on this scale, excellent bowel preparation is defined as a small volume of clear liquid or greater than 95% of mucosal surface seen. A good preparation is having a large volume of clear liquid covering up to 25% of the surface but greater than 90% of mucosal surface is visualized, while fair being the presence of some semi-solid stool that could not be suctioned or washed away but greater than 90% of mucosa seen. A poor is having semisolid stool that could not be suctioned or washed away and less than 90% of surface seen and lastly patient’s with frank solid stool are labelled as having inadequate bowel preparation. A major limitation of the Aronchick scale has high interobserver variability in estimating percentage of mucosal visualization. Also, the scale is based upon visualizing the entire colon, not allowing for individually segments to be judged separately although most endoscopist using this scale grade the preparation according to the poorest preparation area visualized in the colon. Therefore, for more specificity, the Ottawa bowel preparation scale was introduced.
The Ottawa bowel preparation scale which was developed in 2004 [57]. In this scale, the colon is divided into three segments (right, mid and recto-sigmoid). Each section is graded on a scale of 0 to 4 (0 being excellent) with all sections totaling a score of 0-14 (0 being excellent). For each segment, 0 corresponds to an excellent preparation, 1 is suction very little fluid with good visualization, 2 is suctioning liquid to see colon wall, 3 corresponds to the need for washing and suctioning, and 4 represents non-visualization of colon wall. Once the sections are graded, another score is applied to the quantity of fluid which is scored from 0-2, 0 being small amount of fluid, 1 being moderate amount of fluid, and 2 being large amount of fluid. Both the values are then summed and scored out of a total of 14. The Ottawa scale also has a similar limitation as the Aronchick score, with higher interobserver between endoscopists. Also, the Ottawa scale is more complex with no defined agreement on score necessary for overall satisfactory versus unsatisfactory preparation. Lastly, this is the only scoring system that defines the lowest number as a better preparation with all other scales using the higher number as a better preparation, which may lead to confusion among endoscopist. Due to its complexity, other scales have been introduced.
The Boston bowel preparation scale (BBPS) is a validated scale that has demonstrated excellent intra- and interobserver reliability [58,59]. In BBPS, the colon is divided in three segments: Right side, transverse colon, and the left side of the colon. The score is applied after washing the colonic wall and during the withdrawal phase of the colonoscopy. The grading after cleaning, not before, is extremely important and has led to confusion amongst endoscopists with this scale. Each of the three segments is given a score after cleaning of 0 to 3, with 0 being unprepared colon with solid stool, 1 representing portion of the mucosa visualized but other areas not well seen, 2 corresponding to good visualization with minor amount of residual staining with small fragments of stool or opaque liquid, and 3 being entire mucosa visualized with no residual staining, stool, or opaque liquid. The overall score is calculated after adding scores of all three segments for a total of 0 to 9, with 9 representing excellent preparation score. A score of ≥5 seems to be the consensus for adequacy of bowel preparation; however, many endoscopists prefer ≥6 [60,61,64]. A recent study has demonstrated that a BBPS score of 2 or greater in each segment (BBPS of ≥6) is sufficient to detect adenomatous polyps >5 mm and should not affect standard surveillance interval [61]. The BBPS is a widely used score because of its straightforward terminology, easy calculation during colonoscopy, and less inter and intraobserver variability. Furthermore, if training is needed, a training program for the BBPS online may be utilized (http://www.cori.org/bbps/).
Regardless of bowel preparation score used, the scales may significantly help in optimizing bowel preparations for the specified patient population. By using a validated scale and continuous quality improvement, endoscopists may adjust bowel preparations to maximize the efficacy and freely compare to other institutions in area or nationally. Therefore, bowel preparation scores appear to be extremely important in optimizing bowel preparations.
Optimizing bowel preparation for special factors
Many factors may affect the quality of bowel preparation resulting in suboptimal exams, from patient understanding of instructions to co-morbidities affecting bowel transit times. Given these factors, specialization or modification of the bowel preparation may be required.
A common factor is inability of the patient to correctly follow the bowel preparation instructions [65]. Given the research on health literacy, bowel preparation instructions should be written at a level that even children may understand. In the United States, this generally refers to a 5th-grade reading level. By ensuring this, nearly all patients will be able to read and understand the bowel preparation instructions leading to improved bowel preparation scores. To further enhance patient understanding of preparation instructions, many videos are available [66-68]. These educational videos have been shown to significantly improve bowel preparation as well as increase cecal intubation rate and adenoma detection rate [68]. Videos may be available online or made locally at low cost for a specific preparation or patient population. In addition to videos, other patient factors influence bowel preparation.
Many factors have an impact on the optimization of bowel preparation, from co-morbidities to environment [69]. Patient co-morbidities may result in suboptimal bowel preparation such as history of chronic constipation, diabetes mellitus, neurological conditions such as Parkinson’s disease, colonic resection or history of prior abdominal surgeries, and overweight/obesity (defined as body mass index >25 kg/m2) [70-72]. Other factors have also been found to affect quality of preparation, such as later colonoscopy starting time, patient taking bowel preparation as inpatient [70,73], and use of sedatives and hypnotics, especially tricyclic antidepressants [74]. Additional factors have been implicated, including low literacy, single or widowed marital status, Medicaid insurance, hospitalized, and male gender, resulting in a significant number of unsatisfactory bowel preparation for colonoscopy [74-78]. With any of these factors, special attention may be required to optimize the bowel preparation and decrease need for repeat colonoscopy at earlier interval.
The use of videos and recognition of factors influencing bowel preparations will likely improve bowel preparations prior to colonoscopy, reduce unnecessary earlier repeat colonoscopies, and may improve adenoma detection rate with improved visualization. Furthermore, a recent study by Kim et al demonstrated predictive factors for optimizing bowel preparation including <5 h from PEG-ELS consumption to colonoscopy, frequency of defecation >5 times, and completely liquid stool at time of procedure [79]. With predictive factors, optimization of the bowel preparation may be significantly improved. Endoscopists must be mindful of these factors and adjust preparations as needed to optimize the bowel preparation.
Optimizing bowel preparation in special populations
The choice and efficacy of bowel preparation may be heavily influenced by patient factors and co-morbidities. Many special populations may require adjustments in timing and type of bowel preparations. Patients with the following co-morbidities or circumstances usually require modification of the bowel preparation: congestive heart failure, chronic renal disease, inflammatory bowel disease, elderly, and lower gastrointestinal bleeding.
In patients with congestive heart failure or chronic renal disease, the bowel preparation utilized should not result in massive fluid shifts or electrolyte absorption. For these reasons, PEG-ELS seems to the bowel preparation of choice. NaP should not be used due to possibility of phosphate nephropathy [35-39,80]. Furthermore, sodium sulfate preparations have not been studied well in these populations and are generally avoided [41]. Likewise, sodium picosulfate is also avoided in patients with chronic renal disease.
Patients with inflammatory bowel disease are also limited, but not to the extent of those with congestive heart failure or chronic renal disease. In this patient population, the clinician should avoid NaP as it has been shown to potentially cause mucosal damage that may mimic colitis [81]. Other bowel preparations seem to be better.
Elderly patients, 65 years of age or older, have been shown to have poor bowel preparation in up to 19% of colonoscopies [82]. This is due to a variety of reasons but it seems mostly due to the intolerance to drinking a large volume of preparation. In patients 80 years of age or older, approximately 40% report poor tolerance to large-volume bowel preparations [83]. Furthermore, given the prevalence of renal insufficiency in the elderly population, NaP bowel preparations are generally avoided [82]. Therefore, in this population, a low-volume bowel preparation may be ideal.
In patients with lower gastrointestinal bleeding, the bowel preparation also requires some adjustments. Although blood acts as a cathartic laxative, blood coated on the mucosal has been shown to increase incomplete colonoscopies and limit visualization significantly [84,85]. A common practice is what is known as a purge preparations. In this preparation, 4-6 L of PEG-ELS is administered orally or via nasogastric tube (if cannot tolerate oral or unable to drink preparation) over 2-3 h [86,87]. This rapid administration of preparation has been shown to improve the ability to find source and treat bleeding endoscopically [86].
Endoscopists should chose the bowel preparation wisely in these special populations to optimize the efficacy and treatment of these patients. In general, PEG-ELS in split-dose fashion seems to be the safest preparation for most of these populations except in the elderly where low-volume PEG-ELS preparation should predominate.
Optimizing bowel preparation by diet
Practices pertaining to dietary instructions prior to bowel preparation vary globally. In the United States, a clear liquid diet is usually recommended the day prior to the colonoscopy evaluation. This type of restrictive diet is not well liked among patients. Furthermore, the clear liquid diet is difficult to maintain for patients, leading to ingestion of solids foods during the day prior to colonoscopy which, in turn, may decrease quality of bowel preparation. In an effort to improve patient compliance with the dietary restriction prior to colonoscopy, a low-residue diet, rather than clear liquid diet, was introduced and studied.
Multiple studies has evaluated the use a low-residue diet on the day prior to colonoscopy [88-96]. These studies utilized a low-residue diet at various stages of the day, with some having the diet only for breakfast [93], some with breakfast and lunch [92,94,95], one with lunch only [91], and others for the entire day [88-90,96]. Many of these studies showed improved or equivalent bowel preparation quality compared to having a clear liquid diet on the day before colonoscopy. Recently, a meta-analysis was performed on randomized trials comparing clear liquid diet to low-residue diet on the day prior to colonoscopy [97]. This meta-analysis demonstrated that with a low-residue diet prior to outpatient colonoscopy, patients were more willing to have a repeat colonoscopy performed (OR 1.86; 95% CI, 1.34-2.59; P<0.01) and improved tolerability of preparation (OR 1.92; 95% CI, 1.36-2.70; P<0.01) with no differences in quality of bowel preparations or adverse effects [97]. With this new information, liberalizing the diet to a low-residue diet on the day before colonoscopy should be strongly considered to enhance tolerability of preparation while not decreasing overall bowel preparation quality. However, for hospitalized patients, this diet may not be as effective given multiple other factors. In hospitalized patients, a clear liquid diet was noted to be the only dietary modification that improved quality of colonic preparation [73].
The diet on the day prior to colonoscopy does influence the bowel preparation and varies widely throughout the world. In the past, a clear liquid diet has been used in an effort to lower residue in the colon during exam. Based upon new information, a low-residue diet on the day prior to colonoscopy seems to be better for patients and should be utilized more often for outpatient procedures. However, inpatient procedures continue to use a clear liquid diet prior to colonoscopy to optimize the bowel preparation.
Optimizing bowel preparation by timing
The timing of bowel preparation prior to colonoscopy impacts the quality greatly. A shorter interval from completion of bowel preparation to colonoscopy is recommended. It has been reported that the ideal time to colonoscopy after completion of bowel preparation is 3-4 h [98] and should be less than 8 h after completion of bowel preparation [99]. This has led to the concept of split-dosing the bowel preparation.
Split-dose bowel preparation refers to taking a portion of the bowel preparation the night prior to colonoscopy (usually 50%) and the other portion on the day prior to colonoscopy (usually the other 50%). This may be done with nearly all bowel preparations. A meta-analysis of five randomized controlled trials in 2011 compared split-dose PEG-ELS to full-dose PEG-ELS the night before colonoscopy and discovered that by using split-dose PEG-ELS, the number of satisfactory bowel preparations (OR 3.70; 95% CI: 2.79-4.91; P<0.01) and willingness to repeat preparation (OR 1.76; 95% CI: 1.06-2.91; P=0.03) were significantly increased [10]. Furthermore, less nausea and need for discontinuation of preparation were decreased [10]. Since 2011, multiple studies and guidelines have advocated the use of split-dose bowel preparation for any preparation used [1,9-12,100-104]. Given the overwhelming amount of evidence supporting the practice of split-dosing the preparation, split-dosing the preparation should be performed for patients undergoing colonoscopy. However, the timing of the last drink of preparation to beginning of colonoscopy has not been fully addressed. Given the use of sedation medications, the risk of aspiration of bowel preparation contents when consuming the preparation on the same day (as in split-dosing) has induced anxiety among endoscopists and anesthesiologists. New studies have shown that split-dose bowel preparation with last drink of bowel preparation 2-3 h prior to colonoscopy results in similar gastric residual volumes as those with full-dose night before preparations [103,104]. Therefore, split-dosing appears safe with most preferring the last drink of preparation to be 3 h prior to colonoscopy.
Bowel preparation on the same day of colonoscopy is vital in improving the quality of examination. Split-dose bowel preparation has been shown to be superior to full-dose preparation in numerous studies and meta-analyses, which has led to the adoption of this practice in many guidelines. Regardless of the preparation used, splitting the dose will optimize the quality of the bowel preparation.
Concluding remarks
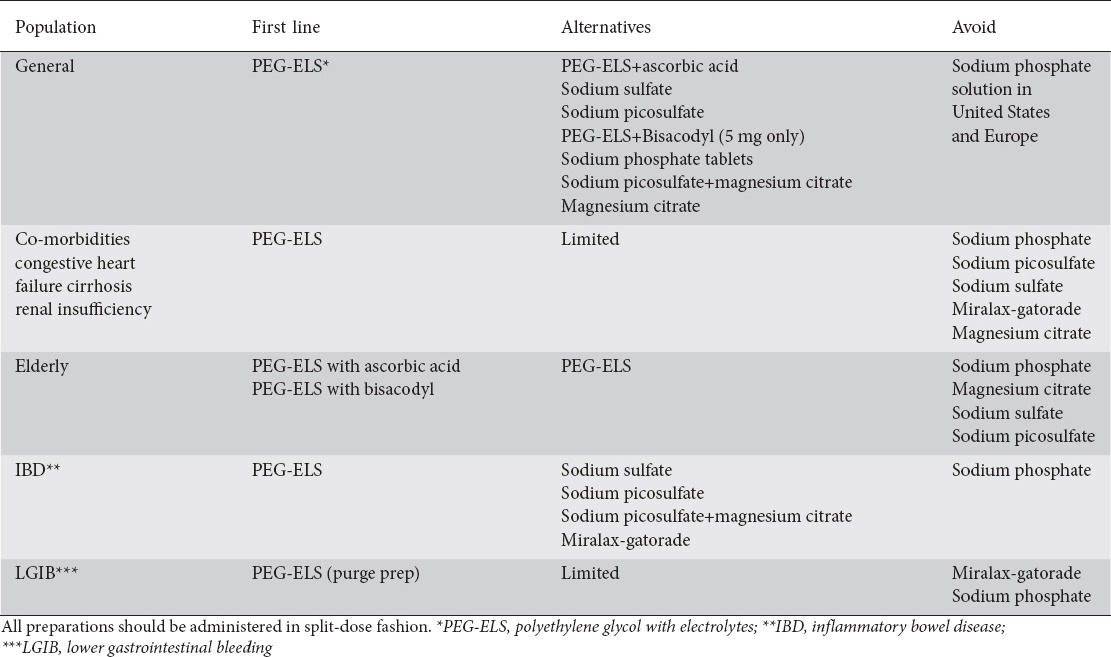
In summary, today’s colonoscopist is increasingly individualizing bowel preparations to achieve an efficient, tolerable, and safe bowel preparation. An optimal bowel preparation leads to decreased total colonoscopy procedure time, increased cecal intubation, and decrease costs by preventing canceled procedures and increasing intervals between screening/surveillance colonoscopies. Predictors of non-compliance with bowel preparation should be assessed prior to scheduling the screening colonoscopy so an attempt can be made to remedy with provision of detailed preparation instructions, switching to a lower volume bowel preparation, and patient engagement. In an effort to minimize confusion, we have summarized our recommendations based on the literature in Table 3. Regardless of choice of bowel preparation, split-dosing the preparation should be performed. Furthermore, adjusting the preparation for special populations, using videos and written preparation instructions, and liberalizing the diet to a low-residue diet on the day prior to colonoscopy is extremely beneficial. Lastly, continuous quality improvement through grading or scoring the adequacy of the bowel preparation enables adjustments in preparation practice to optimize the quality of preparation. With these practices, bowel preparations should be optimized.
Table 3.
Recommendations of bowel preparations for specific populations based on literature and authors’ analysis
Biography
University of Missouri, Columbia; University of Illinois, Peoria; University of California, Irvine, USA
Footnotes
Conflict of Interest: None
References
- 1.Bechtold ML, Choudhary A. Bowel preparation prior to colonoscopy:a continual search for excellence. World J Gastroenterol. 2013;19:155–157. doi: 10.3748/wjg.v19.i2.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75:1197–1203. doi: 10.1016/j.gie.2012.01.005. [DOI] [PubMed] [Google Scholar]
- 3.Hillyer GC, Basch CH, Lebwohl B, et al. Shortened surveillance intervals following suboptimal bowel preparation for colonoscopy:results of a national survey. Int J Colorectal Dis. 2013;28:73–81. doi: 10.1007/s00384-012-1559-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Burke CA, Church JM. Enhancing the quality of colonoscopy:the importance of bowel purgatives. Gastrointest Endosc. 2007;66:565–573. doi: 10.1016/j.gie.2007.03.1084. [DOI] [PubMed] [Google Scholar]
- 5.Wexner SD, Beck DE, Baron TH, et al. A consensus document on bowel preparation before colonoscopy:prepared by a task force from the American Society of Colon and Rectal Surgeons (ASCRS), the American Society for Gastrointestinal Endoscopy (ASGE), and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) Dis Colon Rectum. 2006;49:792–809. doi: 10.1007/s10350-006-0536-z. [DOI] [PubMed] [Google Scholar]
- 6.Hassan C, Bretthauer M, Kaminski MF, et al. European Society of Gastrointestinal Endoscopy. Bowel preparation for colonoscopy:European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2013;45:142–150. doi: 10.1055/s-0032-1326186. [DOI] [PubMed] [Google Scholar]
- 7.Lim YJ, Hong SJ. What is the best strategy for successful bowel preparation under special conditions? World J Gastroenterol. 2014;20:2741–2745. doi: 10.3748/wjg.v20.i11.2741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rex DK, Imperiale TF, Latinovich DR, Bratcher LL. Impact of bowel preparation on efficiency and cost of colonoscopy. Am J Gastroenterol. 2002;97:1696–1700. doi: 10.1111/j.1572-0241.2002.05827.x. [DOI] [PubMed] [Google Scholar]
- 9.Hillyer GC, Lebwohl B, Basch CH, et al. Split dose and MiraLAX-based purgatives to enhance bowel preparation quality becoming common recommendations in the US. Therap Adv Gastroenterol. 2013;6:5–14. doi: 10.1177/1756283X12464100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kilgore TW, Abdinoor AA, Szary NM, et al. Bowel preparation with split-dose polyethylene glycol before colonoscopy:a meta-analysis of randomized controlled trials. Gastrointest Endosc. 2011;73:1240–1245. doi: 10.1016/j.gie.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 11.Martel M, Barkun AN, Menard C, Restellini S, Kherad O, Vanasse A. Split-dose preparations are superior to day-before bowel cleansing regimens:a meta-analysis. Gastroenterology. 2015;149:79–88. doi: 10.1053/j.gastro.2015.04.004. [DOI] [PubMed] [Google Scholar]
- 12.Shah H, Desai D, Samant H, et al. Comparison of split-dosing vs non-split (morning) dosing regimen for assessment of quality of bowel preparation for colonoscopy. World J Gastrointest Endosc. 2014;6:606–611. doi: 10.4253/wjge.v6.i12.606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Parra-Blanco A, Ruiz A, Alvarez-Lobos M, et al. Achieving the best bowel preparation for colonoscopy. World J Gastroenterol. 2014;20:17709–17726. doi: 10.3748/wjg.v20.i47.17709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sharma VK, Chockalingham SK, Ugheoke EA, et al. Prospective, randomized, controlled comparison of the use of polyethylene glycol electrolyte lavage solution in four-liter versus two-liter volumes and pretreatment with either magnesium citrate or bisacodyl for colonoscopy preparation. Gastrointest Endosc. 1998;47:167–171. doi: 10.1016/s0016-5107(98)70351-7. [DOI] [PubMed] [Google Scholar]
- 15.Clark RE, Godfrey JD, Choudhary A, Ashraf I, Matteson ML, Bechtold ML. Low-volume polyethylene glycol and bisacodyl for bowel preparation prior to colonoscopy:a meta-analysis. Ann Gastroenterol. 2013;26:319–324. [PMC free article] [PubMed] [Google Scholar]
- 16.Godfrey JD, Clark RE, Choudhary A, Ashraf I, Matteson ML, Bechtold ML. Low-volume polyethylene glycol and ascorbic acid for bowel preparation prior to colonoscopy:A meta-analysis. World J Meta-Anal. 2013;1:10–15. [PMC free article] [PubMed] [Google Scholar]
- 17.Baudet JS, Castro V, Redondo I. Recurrent ischemic colitis induced by colonoscopy bowel lavage. Am J Gastroenterol. 2010;105:700–701. doi: 10.1038/ajg.2009.637. [DOI] [PubMed] [Google Scholar]
- 18.Ajani S, Hurt RT, Teeters DA, Bellmore LR. Ischaemic colitis associated with oral contraceptive and bisacodyl use. BMJ Case Rep 2012. 2012:bcr1220115451. doi: 10.1136/bcr-12-2011-5451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lopez Morra HA, Fine SN, Dickstein G. Colonic ischemia with laxative use in young adults. Am J Gastroenterol. 2005;100:2134–2136. doi: 10.1111/j.1572-0241.2005.50395_8.x. [DOI] [PubMed] [Google Scholar]
- 20.Oh JK, Meiselman M, Lataif LE., Jr Ischemic colitis caused by oral hyperosmotic saline laxatives. Gastrointest Endosc. 1997;45:319–322. doi: 10.1016/s0016-5107(97)70282-7. [DOI] [PubMed] [Google Scholar]
- 21.Rees DC, Kelsey H, Richards JD. Acute haemolysis induced by high dose ascorbic acid in glucose-6-phosphate dehydrogenase deficiency. BMJ. 1993;306:841–842. doi: 10.1136/bmj.306.6881.841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pockros PJ, Foroozan P. Golytely lavage versus a standard colonoscopy preparation. Effect on normal colonic mucosal histology. Gastroenterology. 1985;88:545–548. doi: 10.1016/0016-5085(85)90519-0. [DOI] [PubMed] [Google Scholar]
- 23.Marshall JB, Pineda JJ, Barthel JS, King PD. Prospective, randomized trial comparing sodium phosphate solution with polyethylene glycol-electrolyte lavage for colonoscopy preparation. Gastrointest Endosc. 1993;39:631–634. doi: 10.1016/s0016-5107(93)70213-8. [DOI] [PubMed] [Google Scholar]
- 24.Franga DL, Harris JA. Polyethylene glycol-induced pancreatitis. Gastrointest Endosc. 2000;52:789–791. doi: 10.1067/mge.2000.109718. [DOI] [PubMed] [Google Scholar]
- 25.Gabel A, Müller S. Aspiration:a possible severe complication in colonoscopy preparation of elderly people by orthograde intestine lavage. Digestion. 1999;60:284–285. doi: 10.1159/000007672. [DOI] [PubMed] [Google Scholar]
- 26.Enestvedt BK, Brian Fennerty M, Zaman A, Eisen GM. MiraLAX vs. Golytely:is there a significant difference in the adenoma detection rate? Aliment Pharmacol Ther. 2011;34:775–782. doi: 10.1111/j.1365-2036.2011.04795.x. [DOI] [PubMed] [Google Scholar]
- 27.Siddique S, Lopez KT, Hinds AM, Ahmad DS, Nguyen DL, Matteson-Kome ML, Puli SR, Bechtold ML. Miralax with gatorade for bowel preparation:a meta-analysis of randomized controlled trials. Am J Gastroenterol. 2014;109:1566–1574. doi: 10.1038/ajg.2014.238. [DOI] [PubMed] [Google Scholar]
- 28.Matro R, Daskalakis C, Negoianu D, et al. Randomised clinical trial:Polyethylene glycol 3350 with sports drink vs. polyethylene glycol with electrolyte solution as purgatives for colonoscopy-the incidence of hyponatraemia. Aliment Pharmacol Ther. 2014;40:610–619. doi: 10.1111/apt.12884. [DOI] [PubMed] [Google Scholar]
- 29.Baeg MK, Park JM, Ko SH, et al. Seizures due to hyponatremia following polyethylene glycol preparation;a report of two cases. Endoscopy. 2013;45(Suppl 2 UCTN):E269–E270. doi: 10.1055/s-0033-1344568. [DOI] [PubMed] [Google Scholar]
- 30.Nagler J, Poppers D, Turetz M. Severe hyponatremia and seizure following a polyethylene glycol-based bowel preparation for colonoscopy. J Clin Gastroenterol. 2006;40:558–559. doi: 10.1097/00004836-200607000-00017. [DOI] [PubMed] [Google Scholar]
- 31.Lewis JJ, Eswaran SL, Schoenfeld PS. Severe hyponatremia associated with MiraLAX-Gatorade bowel prep prior to colonoscopy. Gastroenterology. 2011;140:S–18. [Google Scholar]
- 32.Scarpignato C, Blandizzi C. Editorial:hyponatremia - a possible but forgotten consequence of bowel preparation for colonoscopy. Aliment Pharmacol Ther. 2014;40:1110–1112. doi: 10.1111/apt.12917. [DOI] [PubMed] [Google Scholar]
- 33.Sweetser S, Baron TH. Optimizing bowel cleansing for colonoscopy. Mayo Clin Proc. 2015;90:520–526. doi: 10.1016/j.mayocp.2015.01.015. [DOI] [PubMed] [Google Scholar]
- 34.Tan JJ, Tjandra JJ. Which is the optimal bowel preparation for colonoscopy - a meta-analysis. Colorectal Dis. 2006;8:247–258. doi: 10.1111/j.1463-1318.2006.00970.x. [DOI] [PubMed] [Google Scholar]
- 35.Perkowska-Ptasińska A, Szewczyk K, Skuza A, Wasińska-Krawczyk A, Rydzewski A. Phosphate nephropathy after administration of bowel purgative containing sodium phosphate - a case report. Pol J Pathol. 2014;65:60–65. doi: 10.5114/pjp.2014.42671. [DOI] [PubMed] [Google Scholar]
- 36.Florentin M, Liamis G, Elisaf MS. Colonoscopy preparation-induced disorders in renal function and electrolytes. World J Gastrointest Pharmacol Ther. 2014;5:50–54. doi: 10.4292/wjgpt.v5.i2.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Choi NK, Lee J, Chang Y, et al. Acute renal failure following oral sodium phosphate bowel preparation:a nationwide case-crossover study. Endoscopy. 2014;46:465–470. doi: 10.1055/s-0034-1365419. [DOI] [PubMed] [Google Scholar]
- 38.Slee TM, Vleming LJ, Valentijn RM. Renal failure due to acute phosphate nephropathy. Neth J Med. 2008;66:438–441. [PubMed] [Google Scholar]
- 39.Singal AK, Rosman AS, Post JB, Bauman WA, Spungen AM, Korsten MA. The renal safety of bowel preparations for colonoscopy:a comparative study of oral sodium phosphate solution and polyethylene glycol. Aliment Pharmacol Ther. 2008;27:41–47. doi: 10.1111/j.1365-2036.2007.03558.x. [DOI] [PubMed] [Google Scholar]
- 40.Gonlusen G, Akgun H, Ertan A, Olivero J, Truong LD. Renal failure and nephrocalcinosis associated with oral sodium phosphate bowel cleansing:clinical patterns and renal biopsy findings. Arch Pathol Lab Med. 2006;130:101–106. doi: 10.5858/2006-130-101-RFANAW. [DOI] [PubMed] [Google Scholar]
- 41.Rex DK. Dosing considerations in the use of sodium phosphate bowel preparations for colonoscopy. Ann Pharmacother. 2007;41:1466–1475. doi: 10.1345/aph.1K206. [DOI] [PubMed] [Google Scholar]
- 42.Kumagai E, Shibuya T, Makino M, et al. A randomized prospective study of bowel preparation for colonoscopy with low-dose sodium phosphate tablets versus polyethylene glycol electrolyte solution. Gastroenterol Res Pract 2014. 2014:879749. doi: 10.1155/2014/879749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sagawa T, Sato K, Tomizawa T, et al. A prospective randomized controlled trial of AJG522 versus standard PEG+E as bowel preparation for colonoscopy. Biomed Res Int 2015. 2015:521756. doi: 10.1155/2015/521756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Koshitani T, Kawada M, Yoshikawa T. Bowel preparation for colonoscopy using standard vs reduced doses of sodium phosphate:A single-blind randomized controlled study. World J Gastrointest Endosc. 2014;6:379–384. doi: 10.4253/wjge.v6.i8.379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Di Palma JA, Rodriguez R, McGowan J, Cleveland Mv. A randomized clinical study evaluating the safety and efficacy of a new, reduced-volume, oral sulfate colon-cleansing preparation for colonoscopy. Am J Gastroenterol. 2009;104:2275–2284. doi: 10.1038/ajg.2009.389. [DOI] [PubMed] [Google Scholar]
- 46.Renaut AJ, Raniga S, Frizelle FA, Perry RE, Guilford L. A randomized controlled trial comparing the efficacy and acceptability of phospo-soda buffered saline (Fleet) with sodium picosulphate/magnesium citrate (Picoprep) in the preparation of patients for colonoscopy. Colorectal Dis. 2008;10:503–505. doi: 10.1111/j.1463-1318.2007.01383.x. [DOI] [PubMed] [Google Scholar]
- 47.Katz PO, Rex DK, Epstein M, et al. A dual-action, low-volume bowel cleanser administered the day before colonoscopy:results from the SEE CLEAR II study. Am J Gastroenterol. 2013;108:401–409. doi: 10.1038/ajg.2012.441. [DOI] [PubMed] [Google Scholar]
- 48.Weir MA, Fleet JL, Vinden C, et al. Hyponatremia and sodium picosulfate bowel preparations in older adults. Am J Gastroenterol. 2014;109:686–694. doi: 10.1038/ajg.2014.20. [DOI] [PubMed] [Google Scholar]
- 49.Jafri SM, Monkemuller K, Lukens FJ. Endoscopy in the elderly:a review of the efficacy and safety of colonoscopy, esophagogastroduodenoscopy, and endoscopic retrograde cholangiopancreatography. J Clin Gastroenterol. 2010;44:161–166. doi: 10.1097/MCG.0b013e3181c64d64. [DOI] [PubMed] [Google Scholar]
- 50.Yoo IK, Lee JS, Chun HJ, et al. A randomized, prospective trial on efficacy and tolerability of low-volume bowel preparation methods for colonoscopy. Dig Liver Dis. 2015;47:131–137. doi: 10.1016/j.dld.2014.10.019. [DOI] [PubMed] [Google Scholar]
- 51.Muñoz-Navas M, Calleja JL, Payeras G, et al. A randomized trial to compare the efficacy and tolerability of sodium picosulfate-magnesium citratesolution vs. 4 L polyethylene glycol solution as a bowel preparation for colonoscopy. Int J Colorectal Dis. 2015;30:1407–1416. doi: 10.1007/s00384-015-2307-6. [DOI] [PubMed] [Google Scholar]
- 52.Leitao K, Grimstad T, Bretthauer M, et al. Polyethylene glycol vs sodium picosulfate/magnesium citrate for colonoscopy preparation. Endosc Int Open. 2014;2:E230–E234. doi: 10.1055/s-0034-1377520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kontani M, Hara A, Ohta S, Ikeda T. Hypermagnesemia induced by massive cathartic ingestion in an elderly woman without pre-existing renal dysfunction. Intern Med. 2005;44:448–452. doi: 10.2169/internalmedicine.44.448. [DOI] [PubMed] [Google Scholar]
- 54.Tajika M, Niwa Y, Bhatia V, et al. Efficacy of mosapride citrate with polyethylene glycol solution for colonoscopy preparation. World J Gastroenterol. 2012;18:2517–2525. doi: 10.3748/wjg.v18.i20.2517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mishima Y, Amano Y, Okita K, et al. Efficacy of prokinetic agents in improving bowel preparation for colonoscopy. Digestion. 2008;77:166–172. doi: 10.1159/000141040. [DOI] [PubMed] [Google Scholar]
- 56.Aronchick CA, Lipshutz WH, Wright SH, DuFrayne F, Bergman G. Validation of an instrument to assess colon cleansing [abstract] Am J Gastroenterol. 1999;94:2667. [Google Scholar]
- 57.Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc. 2004;59:482–486. doi: 10.1016/s0016-5107(03)02875-x. [DOI] [PubMed] [Google Scholar]
- 58.Calderwood AH, Schroy PC, 3rd, Lieberman DA, Logan JR, Zurfluh M, Jacobson BC. Boston Bowel Preparation Scale scores provide a standardized definition of adequate for describing bowel cleanliness. Gastrointest Endosc. 2014;80:269–276. doi: 10.1016/j.gie.2014.01.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Calderwood AH, Jacobson BC. Comprehensive validation of the Boston Bowel Preparation Scale. Gastrointest Endosc. 2010;72:686–692. doi: 10.1016/j.gie.2010.06.068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lai EJ, Calderwood AH, Doros G, Fix OK, Jacobson BC. The Boston bowel preparation scale:a valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc. 2009;69:620–625. doi: 10.1016/j.gie.2008.05.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Clark BT, Protiva P, Nagar A, et al. Quantification of adequate bowel preparation for screening or surveillance colonoscopy in men. Gastroenterology. 2016;150:396–405. doi: 10.1053/j.gastro.2015.09.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Halphen M, Heresbach D, Gruss HJ, Belsey J. Validation of the Harefield Cleansing Scale:a tool for the evaluation of bowel cleansing quality in both research and clinical practice. Gastrointest Endosc. 2013;78:121–131. doi: 10.1016/j.gie.2013.02.009. [DOI] [PubMed] [Google Scholar]
- 63.Gerard D FD, Raiser M, Holden J, et al. Validation of a new bowel preparation scale for measuring colon cleansing for colonoscopy:the Chicago bowel preparation scale. Clin Transl Gastroenterology. 2013;4:1–11. doi: 10.1038/ctg.2013.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Marden P CT, Colleypriest B, Robertson D. Current practices for assessing colonoscopy bowel preparation in the U.K. Gastrointest Endosc. 2009;69:AB219. [Google Scholar]
- 65.Ness RM, Manam R, Hoen H, Chalasani N. Predictors of inadequate bowel preparation for colonoscopy. Am J Gastroenterol. 2001;96:1797–1802. doi: 10.1111/j.1572-0241.2001.03874.x. [DOI] [PubMed] [Google Scholar]
- 66.Ajumobi AB, Malakouti M, Bullen A, Ahaneku H, Lunsford TN. YouTube™as a source of instructional videos on bowel preparation:a content analysis. J Cancer Educ. 2015 doi: 10.1007/s13187-015-0888-y. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 67.Basch CH, Hillyer GC, Reeves R, Basch CE. Analysis of YouTube™videos related to bowel preparation for colonoscopy. World J Gastrointest Endosc. 2014;6:432–435. doi: 10.4253/wjge.v6.i9.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Bearelly D, Kottewar S, Almashhrawi A, Davis W, Marshall J, Ibdah J. Instructional video improves the quality of bowel preparation for colonoscopy. Am J Gastroenterol. 2014;109:S599. [Google Scholar]
- 69.Dik VK, Moons LM, Hüyük M, et al. Colonoscopy quality initiative. Predicting inadequate bowel preparation for colonoscopy in participants receiving split-dose bowel preparation:development and validation of a prediction score. Gastrointest Endosc. 2015;81:665–672. doi: 10.1016/j.gie.2014.09.066. [DOI] [PubMed] [Google Scholar]
- 70.Basch CH, Hillyer GC, Basch CE, Lebwohl B, Neugut AI. Characteristics associated with suboptimal bowel preparation prior to colonoscopy:results of a national survey. Int J Prev Med. 2014;5:233–237. [PMC free article] [PubMed] [Google Scholar]
- 71.Lim SW, Seo YW, Sinn DH, et al. Impact of previous gastric or colonic resection on polyethylene glycol bowel preparation for colonoscopy. Surg Endosc. 2012;26:1554–1559. doi: 10.1007/s00464-011-2068-4. [DOI] [PubMed] [Google Scholar]
- 72.Borg BB, Gupta NK, Zuckerman GR, Banerjee B, Gyawali CP. Impact of obesity on bowel preparation for colonoscopy. Clin Gastroenterol Hepatol. 2009;7:670–675. doi: 10.1016/j.cgh.2009.02.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Yadlapati R, Johnston ER, Gregory DL, Ciolino JD, Cooper A, Keswani RN. Predictors of inadequate inpatient colonoscopy preparation and Its association with hospital length of stay and costs. Dig Dis Sci. 2015;60:3482–3490. doi: 10.1007/s10620-015-3761-2. [DOI] [PubMed] [Google Scholar]
- 74.Chung YW, Han DS, Park KH, et al. Patient factors predictive of inadequate bowel preparation using polyethylene glycol:a prospective study in Korea. J Clin Gastroenterol. 2009;43:448–452. doi: 10.1097/MCG.0b013e3181662442. [DOI] [PubMed] [Google Scholar]
- 75.Lebwohl B, Wang TC, Neugut AI. Socioeconomic and other predictors of colonoscopy preparation quality. Dig Dis Sci. 2010;55:2014–2020. doi: 10.1007/s10620-009-1079-7. [DOI] [PubMed] [Google Scholar]
- 76.Nguyen DL, Wieland M. Risk factors predictive of poor quality preparation during average risk colonoscopy screening:the importance of health literacy. J Gastrointestin Liver Dis. 2010;19:369–372. [PubMed] [Google Scholar]
- 77.Reilly T, Walker G. Reasons for poor colonic preparation with inpatients. Gastroenterol Nurs. 2004;27:115–117. doi: 10.1097/00001610-200405000-00004. [DOI] [PubMed] [Google Scholar]
- 78.Yee R, Manoharan S, Hall C, Hayashi A. Optimizing bowel preparation for colonoscopy:what are the predictors of an inadequate preparation? Am J Surg. 2015;209:787–92. doi: 10.1016/j.amjsurg.2014.12.018. [DOI] [PubMed] [Google Scholar]
- 79.Kim HG, Jeon SR, Kim MY, et al. How to predict adequate bowel preparation before colonoscopy using conventional polyethylene glycol:prospective observational study based on survey. Dig Endosc. 2015;27:87–94. doi: 10.1111/den.12312. [DOI] [PubMed] [Google Scholar]
- 80.Beloosesky Y, Grinblat J, Weiss A, Grosman B, Gafter U, Chagnac A. Electrolyte disorders following oral sodium phosphate administration for bowel cleansing in elderly patients. Arch Intern Med. 2003;163:803–808. doi: 10.1001/archinte.163.7.803. [DOI] [PubMed] [Google Scholar]
- 81.Brousse N, Abdelli N, Grimaud JC, Lapuelle J, Marteau P. Endoscopic and histological findings of colonic pseudo-lesions induced by Fleet Phospho-Soda(R) Gastroenterol Clin Biol. 2002;26:105–106. [PubMed] [Google Scholar]
- 82.Day LW, Kwon A, Inadomi JM, Walter LC, Somsouk M. Adverse events in older patients undergoing colonoscopy:a systematic review and meta-analysis. Gastrointest Endosc. 2011;74:885–896. doi: 10.1016/j.gie.2011.06.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Chatrenet P, Friocourt P, Ramain JP, Cherrier M, Maillard JB. Colonoscopy in the elderly:a study of 200 cases. Eur J Med. 1993;2:411–413. [PubMed] [Google Scholar]
- 84.Rossini FP, Ferrari A, Spandre M, et al. Emergency colonoscopy. World J Surg. 1989;13:190–192. doi: 10.1007/BF01658398. [DOI] [PubMed] [Google Scholar]
- 85.Machicado GA, Jensen DM. Acute and chronic management of lower gastrointestinal bleeding:cost-effective approaches. Gastroenterologist. 1997;5:189–201. [PubMed] [Google Scholar]
- 86.Jensen DM, Machicado GA, Jutabha R, Kovacs TO. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Engl J Med. 2000;342:78–82. doi: 10.1056/NEJM200001133420202. [DOI] [PubMed] [Google Scholar]
- 87.Saito K, Inamori M, Sekino Y, et al. Management of acute lower intestinal bleeding:what bowel preparation should be required for urgent colonoscopy? Hepatogastroenterology. 2009;56:1331–1334. [PubMed] [Google Scholar]
- 88.Park DI, Park SH, Lee SK, et al. Efficacy of prepackaged, low residual test meals with 4L polyethylene glycol versus a clear liquid diet with 4L polyethylene glycol bowel preparation:a randomized trial. J Gastroenterol Hepatol. 2009;24:988–991. doi: 10.1111/j.1440-1746.2009.05860.x. [DOI] [PubMed] [Google Scholar]
- 89.Rapier R, Houston C. A prospective study to assess the efficacy and patient tolerance of three bowel preparations for colonoscopy. Gastroenterol Nurs. 2006;29:305–308. doi: 10.1097/00001610-200607000-00007. [DOI] [PubMed] [Google Scholar]
- 90.Soweid AM, Kobeissy AA, Jamali FR, et al. A randomized single-blind trial of standard diet versus fiber-free diet with polyethylene glycol electrolyte solution for colonoscopy preparation. Endoscopy. 2010;42:633–638. doi: 10.1055/s-0029-1244236. [DOI] [PubMed] [Google Scholar]
- 91.Scott SR, Raymond PL, Thompson WO, Galt DJ. Efficacy and tolerance of sodium phosphates oral solution after diet liberalization. Gastroenterol Nurs. 2005;28:133–139. doi: 10.1097/00001610-200503000-00008. [DOI] [PubMed] [Google Scholar]
- 92.Stolpman DR, Solem CA, Eastlick D, Adlis S, Shaw MJ. A randomized controlled trial comparing a low-residue diet versus clear liquids for colonoscopy preparation:impact on tolerance, procedure time, and adenoma detection rate. J Clin Gastroenterol. 2014;48:851–855. doi: 10.1097/MCG.0000000000000167. [DOI] [PubMed] [Google Scholar]
- 93.Melicharkova A, Flemming J, Vanner S, Hookey L. A low-residue breakfast improves patient tolerance without impacting quality of low-volume colon cleansing prior to colonoscopy:a randomized trial. Am J Gastroenterol. 2013;108:1551–1555. doi: 10.1038/ajg.2013.21. [DOI] [PubMed] [Google Scholar]
- 94.Sipe BW, Fischer M, Baluyut AR, et al. A low-residue diet improved patient satisfaction with split-dose oral sulfate solution without impairing colonic preparation. Gastrointest Endosc. 2013;77:932–936. doi: 10.1016/j.gie.2013.01.046. [DOI] [PubMed] [Google Scholar]
- 95.Walter J, Patel A, Matro R, et al. The impact of diet liberalization on bowel preparation for colonoscopy. Am J Gastroenterol. 2013;108(Suppl 1):S162. doi: 10.1055/s-0043-101694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Butt J, Bunn CE, Eldho P, Gibson PR, Brown GJ. The white diet is preferred and better tolerated than a clear fluid diet without hindering successful bowel preparation for colonoscopy. Gastrointest Endosc. 2014;79:AB587. [Google Scholar]
- 97.Nguyen DL, Jamal MM, Nguyen ET, Puli SR, Bechtold ML. Low-residue versus clear liquid diet before colonoscopy:a meta-analysis of randomized controlled trials. Gastrointest Endosc. 2016;83:499–507.e1. doi: 10.1016/j.gie.2015.09.045. [DOI] [PubMed] [Google Scholar]
- 98.Seo EH, Kim TO, Park MJ, et al. Optimal preparation-to-colonoscopy interval in split-dose PEG bowel preparation determines satisfactory bowel preparation quality:an observational prospective study. Gastrointest Endosc. 2012;75:583–590. doi: 10.1016/j.gie.2011.09.029. [DOI] [PubMed] [Google Scholar]
- 99.Bryant RV, Schoeman SN, Schoeman MN. Shorter preparation to procedure interval for colonoscopy improves quality of bowel cleansing. Intern Med J. 2013;43:162–168. doi: 10.1111/j.1445-5994.2012.02963.x. [DOI] [PubMed] [Google Scholar]
- 100.Bucci C, Rotondano G, Hassan C, et al. Optimal bowel cleansing for colonoscopy:split the dose!A series of meta-analyses of controlled studies. Gastrointest Endosc. 2014;80:566–576.e2. doi: 10.1016/j.gie.2014.05.320. [DOI] [PubMed] [Google Scholar]
- 101.Altawil J, Miller LA, Antaki F. Acceptance of split-dose bowel preparation regimen for colonoscopy by patients and providers. J Clin Gastroenterol. 2014;48:e47–e49. doi: 10.1097/MCG.0b013e3182a9f78d. [DOI] [PubMed] [Google Scholar]
- 102.Johnson DA, Barkun AN, Cohen LB, et al. US Multi-Society Task Force on Colorectal Cancer. Optimizing adequacy of bowel cleansing for colonoscopy:recommendations from the US multi-society task force on colorectal cancer. Gastroenterology. 2014;147:903–924. doi: 10.1053/j.gastro.2014.07.002. [DOI] [PubMed] [Google Scholar]
- 103.Agrawal D, Elsbernd B, Singal A, Rockey D. Gastric residual volume after split-dose compared with evening-before polyethylene glycol bowel preparation. Gastrointest Endosc. 2016;83:574–580. doi: 10.1016/j.gie.2015.08.081. [DOI] [PubMed] [Google Scholar]
- 104.Huffman M, Unger RZ, Thatikonda C, Amstutz S, Rex DK. Split-dose bowel preparation for colonoscopy and residual gastric fluid volume:an observational study. Gastrointest Endosc. 2010;72:516–522. doi: 10.1016/j.gie.2010.03.1125. [DOI] [PubMed] [Google Scholar]