

Abstract
To impact population health, it is critical to collaborate across disciplinary and practice-based silos and integrate resources, experiences, and knowledge to exert positive change. Complex systems shape both the prevention outcomes researchers, practitioners, and policymakers seek to impact and how research is translated and can either impede or support movement from basic scientific discovery to impactful and scaled-up prevention practice. Systems science methods can be used to facilitate designing translation support that is grounded in a richer understanding of the many interacting forces affecting prevention outcomes across contexts. In this paper, we illustrate how one systems science method, system dynamics, could be used to advance research, practice, and policy initiatives in each stage of translation from discovery to translation of innovation into global communities (T0-T5), with tobacco prevention as an example. System dynamics can be applied to each translational stage to integrate disciplinary knowledge and document testable hypotheses to inform translation research and practice.
Electronic supplementary material
The online version of this article (doi:10.1007/s13142-016-0390-z) contains supplementary material, which is available to authorized users.
Keywords: Translational stages, Translational research, Dynamic complexity, System dynamics, Behavioral disorders, Prevention science
INTRODUCTION
This paper illustrates the use of a systems thinking approach, system dynamics, to guide the integration of evidence and otherwise isolated efforts to translate evidence into impactful action targeting complex risky behaviors. We consider tobacco prevention as an example. Broadly, a small fraction of scientific insights is actually translated into real-world effects. And, when this does occur, the process can take decades [1–5]. Translation of scientific findings into widely used preventive interventions involves six interconnected stages (T0–T5, see Table 1). Back-translation is an integral part of the translation process, whereby earlier steps are revisited as new insights emerge and demand integration into earlier stage’s frameworks, methods, and deliverables to strengthen impact. Many challenges present themselves throughout the translational process, protracting its effectuation. For example, changes in environment, policy, or prevention implementation systems often require old interventions to be updated [6]. If expected efficacy cannot be established, foundational science and intervention design should be revisited. And if negative real-world reactions to intervention undermine its potential impact (effectiveness), implementation plans need to be altered or a new intervention developed [6]. Another challenge stems from the need for collaboration both within and across all translational stages between teams of basic and social scientists, intervention developers, organizational and community leaders, cross-sector agency staff, front-line service providers, dissemination and implementation scientists, funders, policymakers, and individuals whose behaviors are targeted for change.
Table 1.
Translational research stages—definitions, sources of complexity, and examples of complexity in tobacco prevention
| Type | Type 0 translation (T0) | Type 1 translation (T1) | Type 2 translation (T2) |
|---|---|---|---|
| Definition | The fundamental process of translating findings and discoveries from social and biomedical sciences into research with human subjects. | Moving from bench to bedside. Translation of applied theory to methods and program development. | Moving from bedside to practice and involves translation of program development to efficacious trials. |
| General challenge driven by complexity | In this translational stage, it can be challenging to integrate different scientific research discoveries relevant to a complex behavioral problem that occur across relevant disciplines (e.g., psychology, neurobiology, social epidemiology, behavioral economics) that have implications at multiple ecological levels (e.g., intra- and inter-personal, family, community, etc.). | As interventions, programs, and policies are developed, they must be based on a holistic understanding of the mechanisms determining risky behaviors. With increasing complexity of underlying mechanisms, it is more difficult to design impactful interventions because unaddressed factors may undermine effects. | Maximizing intervention efficacy requires understanding how interventions are best delivered. Based on insights from T0 and T1 work, it is important to make critical decisions about how an intervention should be implemented. In the context of complex behavior change, this can require careful study, planning, and experimentation. |
| Challenge specific to tobacco prevention | How do neurobiological processes, epigenetics, and socio-cultural forces interconnect and affect tobacco use, non-use, quitting, and relapse in individuals and populations over time? (Fig. 1) | Based on the holistic, mechanistic understanding of tobacco use resulting from T0 stage work, what are the most appropriate and actionable targets for decreasing tobacco use? What unanticipated consequences might result from each option? Can actions be re-designed to make them more synergistic and impactful? (Fig. 2) | Before implementing a school-based prevention intervention, what must be considered to support intervention fidelity? What is the appropriate dosage of intervention components? For an accompanying social marketing campaign, what can be done to ensure that critical audiences are reached to maximize intervention synergy? (Fig. 3) |
| Type | Type 3 translation (T3) | Type 4 translation (T4) | Type 5 translation (T5) |
| Definition | Determining whether efficacy can be replicated under real world settings. | Wide-scale implementation, adoption and institutionalization of new guidelines, practices, and policies. | Translation to global communities. Involves fundamental, universal change in attitudes, policies, and social systems. |
| General challenge driven by complexity | As more complex behaviors are targeted by intervention, all of the factors that matter in stages T0-T2 are likely to vary in the real world – across individuals, community, and over the life-course. At this point, it is important to identify and evaluate which complexities across real-world settings are most likely to compromise or bolster real-world effectiveness. | In this translational stage, it is important to study threats to broad use of the intervention. The greater the quantity and diversity of stakeholders affected by the intervention, the greater is the likelihood that some group (or groups) might resist it. At this point, it is important to understand what aspects of the intervention might be resisted, by whom, and why. | As the complexity of targeted behaviors increases, and the number of stakeholders affecting or affected by intervention grows, a more complex web of attitudes, incentives, relationships, rules of engagement, and sphere of influence surrounds intervention. Understanding which changes will best support prevention can be daunting and requires careful planning. |
| Challenge specific to tobacco prevention | How will the multi-pronged tobacco prevention intervention (school-based intervention with an accompanying social marketing campaign) work in communities with different levels of resources and motivation to implement? What else might threaten the intervention’s effectiveness in certain communities? How might a community adapt it to address problems that arise in implementation, to make the intervention more consistent with local context and culture? (Fig. 4) | Who is most likely to react negatively to the tobacco prevention intervention, and why? What shape is resistance likely to take, and will it undermine the intervention’s effectiveness? What can be done to position the intervention for minimal resistance and optimal wide-scale diffusion? (For example, can tobacco company response be anticipated and addressed at the outset?) (Fig. 5) | What can be done within communities, and at state, national, and global levels to best support meaningful tobacco prevention? (Fig. 6) |
Effective translation requires strong, interdisciplinary foundational science, as well as integration of this knowledge to support transdisciplinary and holistic understanding of the mechanisms affecting risky behaviors (moving from science to efficacy, T0–T2). To succeed, the interventions developed in T1, implementation plans developed in T2 and T3, dissemination plans developed in T4, and action plans to support global impact developed in T5 must all be grounded in this transdisciplinary understanding. And importantly, given ultimate translational goals, the process must also be cognizant of what is practical and impactful within different contexts. Successful translation also requires learning and adaptive leadership to change attitudes, policies, and social systems in ways that scaffold the intervention in a dynamic world. Not only are the high-risk outcomes targeted by prevention often themselves complex but also is the interconnected set of factors shaping effective translation of knowledge into practice, policy, and supportive environments/communities.
To improve the ability to navigate translation efficiently and effectively, researchers, practitioners, and policymakers need practical and reliable methods that support transdisciplinary understanding and action when dealing with this complexity. Systems thinking, captured in diagrams and models, could be used to better transfer knowledge to other research teams and integrate insights across translational stages and contexts over time. In this paper, we introduce and illustrate one example of a broader class of systems science methods—system dynamics—which could be used to grow understanding and strengthen action around complex translation efforts. We (1) define key terms related to complexity, including “dynamic complexity,” “systems problems,” and “feedback loops”; (2) introduce system dynamics causal loop and stock and flow diagramming as a means of elucidating determinants of complex problematic behavior, which will serve as the foundation for developing more robust, sustainable solutions; (3) illustrate how these methods could be used to explicate, diagrammatically, the complex factors affecting each stage of translation; and (4) describe how converting diagrams into quantified computer simulation models could further support research, practice, policy, and advocacy seeking to prevent high-risk behaviors. Using systems diagramming at each stage of translation will advance inquiry beyond key events or patterns/associations between factors in favor of developing a richer understanding of the complex system structure producing outcomes over time.
Illustrating complexity in translation
At each stage, complexity might arise, making a translational initiative even more challenging. For example, consider intervention development (T1) focused on reducing tobacco use among teens and young adults through restricting youth access to tobacco. This approach is grounded in T0 understanding of the most important factors shaping initiation and use. Is that understanding sufficiently broad? Substantial effort has, in fact, been directed toward restricting youth access to tobacco; all 50 states have passed youth access laws, such as the Synar Amendment, as a target for intervention endorsed by the Centers for Disease Control and Prevention and the Institute of Medicine [7–10]. Unfortunately, there is limited and mixed support for this approach, and it remains controversial [11–19], in part, due to how difficult it is to restrict teens from obtaining cigarettes from noncommercial sources [20] and the potential for criminalizing youth [12]. These laws may be more costly to enforce, with requisite resources perhaps better spent in other ways. Additionally, when federal or state governments implement a policy that is designed to reduce initiation, whether it is restricting youth access, availability, or taxation, it may trigger reactive strategies by the tobacco industry because it is regarded as an attempt to limit industry marketing efforts and revenue [21, 22]. That said, perhaps evidence on the effectiveness of youth access is mixed because the context in which it is evaluated differs, e.g., were other interventions targeting social acceptability of smoking among youth and addressing enforcement of youth access restrictions present?
These macrodynamics threatening success of tobacco prevention initiatives are compounded by the complexity of individual-level factors affecting tobacco use among teens, At the level of T0, an understanding of the interaction between individual-level risk factors (e.g., genetics and physiological response to nicotine) and a variety of factors operating at other levels or within other systems (e.g., peer and family influence, economic and marketing systems, educational and counter-educational systems, and, state/federal regulatory systems) [21, 23] should inform T1 prevention planning. And there is wide variation between cause and effect across individuals and groups. For teens, social and physiological reinforcements associated with smoking are immediate, while negative health effects take decades to manifest. Health risks are not linear over the life course or by dose, nor are the effects of triggers on the risk of relapse among an experimenting teen trying to break their budding addiction. Youth access to tobacco is also a very important and relevant factor that must be understood—but in the context of broader systems forces [23].
Defining “dynamic complexity”
As described above, tobacco use illustrates characteristics of a dynamically complex problem [24, 25]. Dynamic complexity arises when focal outcomes over time are shaped by an inter-connected and changing web of factors crossing socio-ecological levels (e.g., factors within organs, an individual, a family, a community, a state or country) and disciplines (e.g., physiology, psychology, sociology, economics). Unlike static associations, these outcomes and associated factors are jointly changing in time, influencing one another. Dynamic complexity is compounded by heterogeneity among affected individuals (e.g., by race, SES, developmental stage), as well as the context surrounding prevention efforts (e.g., family behaviors and influence, related policies and resources in the community, competing priorities for the individual or community, etc.). Additional complexity is introduced by nonlinear relationships and wide variations in the timing between the influence, their invoked changes, and their downstream “ripple effects.” Ripple effects often involve feedback wherein variables involved in strings of cause and effect are reciprocal or circular—either reinforcing or counteracting (balancing) earlier changes [24]. These characteristics often combine to create counter-intuitive or “emergent” system behavior [26].
Failure to appreciate dynamic complexity may lead to the development, implementation, and dissemination of interventions that are not particularly synergistic [23, 27] or that make outcomes worse despite the investment [24, 25, 28, 29]. In the context of limited public health resources and resistance to policy [25], knowing which effective interventions to prioritize, integrate, and disseminate, is challenging. Table 1 outlines complexity in each translational stage to illustrate ways in which an understanding of dynamic complexity may improve results within and across each stage.
Using systems science approaches to address complex translational challenges
Addressing the complex array of factors that affect high-risk behaviors and translational efforts to prevent their emergence does not need to seem daunting. There are many systems science methods designed to deal with such complexity. Quoting a call to use systems science methods in prevention [24], “systems science is a broad term referring to a family of analytic approaches that at their heart aim to elucidate the behavior of complex systems and inform efforts to address one or more system problems.”
Defining “system”
Often the word “system” conjures images of an organizational chart, biological systems, or technology. Instead of these very formal systems, for our present purposes, we pose that systems should be thought of as all of the forces and factors affecting, arising from, and responding to a problem or behavioral outcome of interest and the structure (rules and relationships) directing how these factors change over time. A system, as defined by Levine and Fitzgerald is “…a functional whole, composed of a set of components, coupled together to function in a way that might not be apparent from the functioning of the separate component parts” [30].
For example, rather than attempting to understand how the Federal Drug Administration (FDA) works (one formal system), we might seek to understand how we could increase or improve FDA regulation of tobacco. This question would compel us to consider systems forces well outside of the government, such as norms around regulation or personal rights to clean air, tobacco industry lobbying, tobacco education and control, perceived health risks from smoking, or even current smoking prevalence. While it is important to improve our understanding of formal systems, we must not forget that sometimes less formal systems can be incredibly powerful. As an example, Pentz has shown that changing social norms towards non-drug use promotes more rapid adoption of policies that are aimed at institutionalizing prevention programs compared to administrative voting on formal policy change [31].
Systems science methods to model dynamically complex systems problems
In the presence of dynamic complexity, systems science offers several approaches to conceptualizing and simulating complex systems challenges. The specific systems science modeling approach chosen depends on a modeling team’s objectives and the most efficient approach to simulating the system the model seeks to replicate. For example, discrete event and agent-based models simulate individual-level events and interactions among a population of autonomous agents (often people, in prevention research) as they interact with system resources. System dynamics models typically simulate the most important set of interacting system forces that lead to problematic patterns of behavior (measurable outcomes) over time. Rather than simulating heterogeneous individuals, system dynamics models focus on outcomes relevant to a typical individual (such as the likelihood a youth will use tobacco), the number of individuals in a population with different behaviors or outcomes over time (such as the number of youth who have ever tried versus never tried cigarettes), or other accumulating variables of interest such as organizational adoption of a prevention practice across the country. While each of these and other methods are relevant to translational prevention research, for simplicity, we will focus on illustrating how one, system dynamics, could be used to advance prevention initiatives through each translational stage in the presence of dynamic complexity.
System dynamics methods offer a diagrammatic and mathematical way of thinking about and representing dynamically complex system behavior over time (i.e., trends in key variables under study). System dynamics methods also offer guidance on building, testing, and using these diagrams—and ultimately quantified computer simulation models—to support learning and guide intervention [32]. It is an iterative process, where clear boundaries around the system problem under study must be established to focus a given project around the key forces shaping outcomes of interest as well as to inform decision-making about how best to direct change [28, 32, 33]. Guidance and scripted activities such as those reflected within system dynamics group model building have been developed to ensure stakeholders are meaningfully engaged in system dynamics processes and to guide use of these methods by new teams [34–37].
The first step, also the emphasis of this paper, is to use disciplined diagramming to understand the important forces shaping outcomes. In this way, diagrams become dynamic hypotheses, documenting the set of cause-and-effect relationships occurring over time that are thought to produce observed, hoped for, or feared trends. Relationships in diagrams are operationalized as a series of ordinary difference equations, often using specialized software, and simulated under different “what if” scenarios. As a modeling approach, system dynamics methods simplify reality; nevertheless, it complements reductionist approaches that are only focused on individual components and are not well positioned to study problems including nonlinear relationships, delays, or feedback loops holistically, over time. System dynamics also has an advantage over multilevel theory that posits that multiple levels of influence operate simultaneously on behaviors targeted for prevention, but that does not explain the processes by which factors affect each other [25, 29, 38].
METHODS: DIAGRAMMING COMPLEX SYSTEMS PROBLEMS USING SYSTEM DYNAMICS
We developed a sequence of systems science diagrams that correspond to each transitional state in Table 1. We start with a simple diagram to introduce basic diagrammatic constructs and add more components to build in additional important factors grounded in evidence and theory. Across translational stages, we sought to illustrate how diagramming could integrate different expertise to inform the development (T1), testing (T2 and T3), adaptation (T1-T3), scale-up, and dissemination (T4) of interventions, as well as to change the world in which we intervene to make intervention more globally impactful (T5). These diagrams are for illustration only and actual application of them to the real world would require further testing and iteration [32]. While system dynamics methods have been used to study tobacco control [21, 22, 39–56] and even to inform implementation of evidence into practice broadly [21], this is the first attempt to apply the method to illustrate dynamic complexity and efforts within each translational stage.
Components of system dynamics models
The first component of diagrams are variables—noun or noun phrases with clear meaning when they increase or decrease over time. When a change in one variable leads to a change in another variable, an arrow is drawn from the first (independent variable) to the second (dependent variable). This causal linkage between variables is annotated by placing an “s” or “o” on the arrow to describe whether variables move in the same or opposite directions, respectively. Key variables whose accumulations over time are key in defining “the physics” of a problematic system are denoted as stocks and diagrammed with text in boxes. Flows carrying contents between stocks over time are indicated as pipes, double-lined arrows, with valves that control the rate of flow.
A feedback loop occurs when variables, connected by arrows, create a closed loop. These circular strings of ripple effects drive powerful changes in systems. Figure 2a illustrates one feedback loop, while Fig. 2b illustrates two loops involving both causal linkages and flows. In Fig. 2a, the reinforcing power of social norms is driven by a reinforcing loop. This type of loop circles around to reinforce earlier changes, leading to exponential growth or decay in variables within the loop. Changes could trigger this loop to operate in the other direction, where an external force decreasing the prevalence of tobacco use will reinforce anti-tobacco use norms—at least until something else changes outside of this feedback loop. As the diagram is extended, additional system forces important in reproducing focal trends are added to the diagram. Overall, the goal is to understand the balance of system effects and the effect of delays between cause and effect that contribute to counterintuitive system behavior. Given the importance of feedback loops in determining system behavior, inquiry around each loop should focus on when they would operate and what might occur to limit their growth. The second type of feedback loop, balancing loops, counteracts change in systems. Feedback loops are annotated with a small circle and a letter, either “R” or “B” depending on whether the loop is reinforcing or balancing.
Fig. 2.

System dynamics diagram illustrating complexity in type 1 translation work supporting tobacco prevention. For a larger version of the figure, see Supplementary materials
RESULTS: APPLICATION OF DIAGRAMMING AT EACH TRANSLATIONAL STAGE TO ADVANCE TOBACCO PREVENTION
In this section, we present a system dynamics diagram to illustrate how diagramming could advance transdisciplinary inquiry within each translational research stage. Translational stages, sources of complexity common in each, and a focal challenge relative to tobacco prevention highlighted in each section below are summarized in Table 1.
Mechanistic understanding of system functioning: system dynamics and T0 translation
In T0, basic research is used to generate and test etiologic models via scientific hypotheses that explain or predict phenomena of interest. To advance tobacco control, a challenge for prevention science is to adequately describe the interplay of multiple factors associated with smoking initiation and cessation. Epidemiological methods help us establish relationships, such as associations between environmental cues and social norms that support tobacco use and prevalence rates in different subpopulations, often in the form of regression models. However, factors such as social norms and prevalence can be the cause and effect of change in each other (a feedback loop). Furthermore, complexity grows when additional factors are considered within transdisciplinary inquiry. An addiction psychologist might introduce stages of use and describe differences in individuals’ responsiveness to intervention based on their stage. A psychiatrist might describe the brain’s neurochemical mechanisms, which contribute to initiation and addiction.
A system dynamics model allows the epidemiologist to introduce a feedback loop between social norms and prevalence rates (Fig. 1a), not achievable with traditional regression methods. The model can be expanded by an addiction psychologist, modeling individuals in stocks based on their stages of use (never using, using, quitting, or abstaining) with flows between stocks that describe how responsive individuals are in these stages to cues in the environment (Fig. 1b). Finally, modelers can integrate a psychiatrist’s contributed understanding of the brain’s neurochemical mechanisms, such as reward and stress mechanisms depicted in Fig. 1c. Compared to the etiological models, each discipline would create and test independently in T0, system dynamics models have the potential to provide a more thorough mechanistic understanding of system functioning, thus informing the development of more synergistic interventions in T1.
Fig. 1.
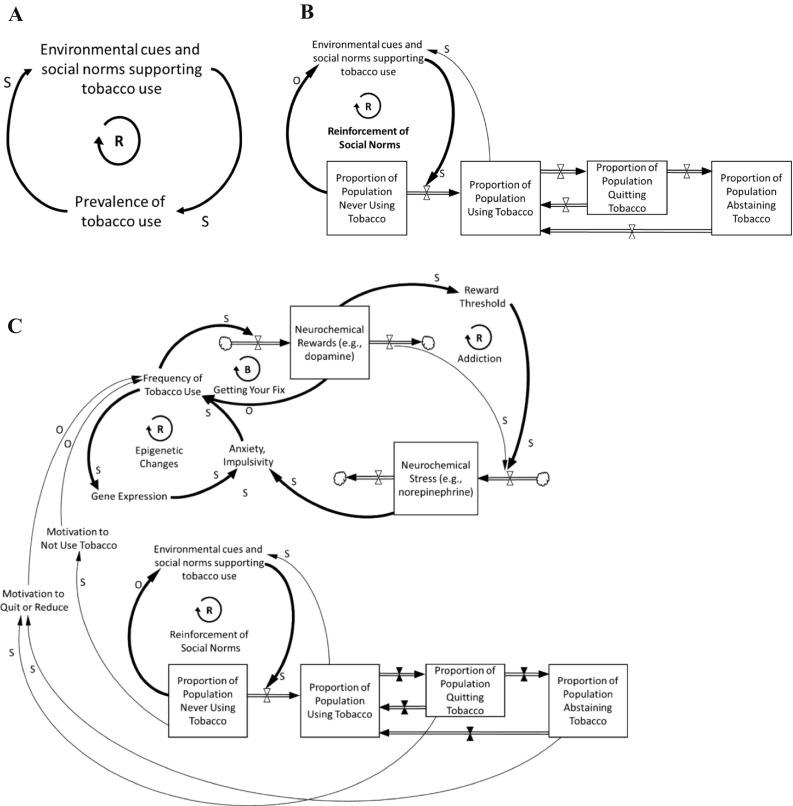
System dynamics diagram illustrating complexity in type 0 translation work supporting tobacco prevention, with increasing detail added across panels. Arrows indicate causal connections, where a change in the first variable triggers a change in the second over time, all else equal. S indicates variables move in the same direction, whereas O indicates movement in opposite directions. Boxes represent stocks, while double-lined arrows indicate flow between stocks over time. Feedback loops are indicated as either reinforcing R or balancing B. For a larger version of the figure, see Supplementary materials
Developing interventions: system dynamics and T1 translation
Stage 1 translation (T1) involves consideration of scientific discoveries in T0 to design more effective interventions, programs, and policies. A challenge for prevention science is to identify the set of intervention strategies that, when combined, has the greatest potential impact while limiting negative unintended consequences. Mechanistic (explanatory) system dynamics models developed in T0 can support the identification of high-impact targets for intervention or leverage points [57], as well as potential unintended consequences [25]. These otherwise unanticipated consequences, which can be either positive or negative, should be carefully considered as interventions are developed. For example, a widespread treatment innovation such as nicotine replacement therapy (NRT) may result in a positive unintended prevention effect because NRT will reduce the number of those who smoke, reducing social norms supporting tobacco use, which reduces the rate at which never smokers initiate.
An interdisciplinary team is needed to inform the development of system dynamics models in T1, which serve as testable, dynamic hypotheses (theories of change) about interventions’ effects. For example, a clinical epidemiologist is needed to understand model variables such as the rate of acceptance and success of NRT (not diagrammed, but affecting dynamics in Fig. 2) and its association with overall prevalence of tobacco use. At an individual level, a psychiatrist would describe how NRT increases neurochemical rewards, leading to slow reduction of craving and habitual use [58]. A psychologist could suggest that, without consideration of the potential influence of environmental cues and social norms, the impact of NRT may be limited long-term. Finally, public health professionals citing studies such as by Niederdeppe et al. [59] would suggest that social marketing campaigns at a population-level can play an important role in reducing norms supporting tobacco use, reducing initiation, and the subsequent number of never users—triggering an increase in participation in smoking cessation as motivation to quit increases among current smokers.
The diagram in Fig. 2 thus highlights several potential strategies for supporting tobacco prevention. System dynamics models at this stage generate new opportunities to consider dynamic hypotheses regarding how interventions influence each other over time. For example, a team might hypothesize that social marketing campaigns and NRT will produce synergistic effects because (1) social marketing campaigns reduce social norms supporting tobacco use, which increases the population of non-users and improves motivation to quit among users, and (2) NRT enhances motivated users chances of successfully quitting. And then, over time, (3) reductions in social norms that support tobacco use are further reinforced. With a simulated version of the model integrating relevant data and scientific evidence, the hypothesis could be tested in silico to inform evaluation measures for research examining the effectiveness and efficacy of such an intervention. Other combination intervention scenarios can be formulated and simulated, to help teams determine which combination of interventions is likely to best support reaching tobacco prevention goals [21, 60, 61].
Maximizing the efficacy of a theoretical intervention: system dynamics and T2 translation
Type 2 translation involves moving program development to implementation, with a focus on internal and external validity. Although most research places emphasis on the end behavioral outcomes, the translational process requires an understanding of how interventions are delivered. After strategies for intervention are developed (T1), it is necessary to understand implementation parameters such as the dosage of included strategies, how to ensure fidelity to intended design, and how many individuals need to be reached for the strategy to become an efficacious intervention [62]. At this stage, key challenges for prevention research include variability in how intervention strategies are interpreted and implemented, differential response of targeted individuals, and understanding of non-linear effects of intervention dose in the short- and long-term. System science diagramming can inform this understanding.
In our example, we are considering prevention-focused interventions at both prevention and treatment levels. These interventions seek to affect initiation and cessation transitions. The dosage of intervention components, which accumulate based on implementation design as well as fidelity to this design in either research-controlled (efficacy) or more realistic practice-based (effectiveness) settings are important [63] and might be represented with stocks. Stocks could also be used to study the reach of intervention components. To illustrate, reach would increase if implementation of a prevention program is spread from one teacher to another within the same school, from one school to a district, or across individuals receiving the intervention, thus increasing the number of youth actually exposed to and participating in the intervention.
In Fig. 3, the new stocks represent research participants or intervention targets. Consider a potential school-based prevention intervention, divided into three major components—education of short-term consequences, refusal skills, and normative education (each an evidence-based strategy for tobacco use prevention among youth [63]). To address detailed implementation needs and feasibility of such interventions, it is critical to get the actual implementers (teachers, principals) involved. Key issues to discuss at this stage might include the following: motivation and attitudes of staff, training of implementers, and the quality of intervention design (e.g., complexity, relative advantage, compatibility, observability, trialability [23, 63]). Similarly, when considering intervention dosage to support cessation, it is important to get key stakeholders involved to strengthen the dosage of cessation support and extend the reach of a social marketing campaign.
Fig. 3.

System dynamics diagram illustrating complexity in type 2 translation work supporting tobacco prevention. For a larger version of the figure, see Supplementary materials
The maximization of efficacy is considered in this case, within the limitations of potential dose-response, fidelity, and intervention resources. For example, it would be ideal for the treatment intervention to support every single smoker in quitting; however, this is not feasible. Similarly, a limited-fund social marketing campaign can have only temporary effects on social cues and responses to the cues. Diagramming and early simulation modeling using existing data informs implementation plan design, through improved understanding of the likely value associated with changes in dosage, reach, or fidelity realized through reallocating resources across strategies or improving the balance between multiple strategies by adjusting their dosage or timing. There may be synergies between strategies whereby one amplifies or attenuates the effect of others, depending on when and the extent to which it is implemented [23, 27]. A simulated system dynamics model has significant potential to enhance understanding of how organizational dynamics (e.g., within a school) may impact the effectiveness of interventions (e.g., school-based tobacco prevention). For example, a model formulated to understand the influence of motivation, communication, and design quality on fidelity of an intervention to promote healthy foods in convenience stores (e.g., menu labeling, introduce healthier foods) found important information about “tipping” dynamics in regards to staff motivation [64]. There was a specific level of motivation at which a small change (over or under) influenced outcomes considerably. This has important implications for setting thresholds for intervention design parameters such as dosage and may elucidate potential levels at which increasing dosage results in diminishing marginal returns on investment.
Informed by modeling, actual efficacy trials are then implemented and can improve numeric estimates of model parameters. Model re-analysis could inform even more efficacious intervention, given project resources.
Maximizing real-world effectiveness of an efficacious intervention: system dynamics and T3 translation
To launch intervention in real-world settings, the goal in T3 is to understand and support intervention adoption, successful adaptation, and dissemination. For prevention research, a challenge at this stage is to understand the impact of interventions implemented in new contexts and under varying conditions. For example, appreciating the impact of political landscapes or the short- and long-term financial and resource burdens imposed by sustained intervention is critical. Impact estimates from efficacy studies might, for example, have been based on a few participating schools that did not have overworked teachers. Schools that are chronically understaffed and with overworked teachers might formally welcome the new intervention, but it may prove less effective or require changes to the intervention or its implementation plan. Systems science methods are useful at this stage to document, quantify, and test, through simulation, effects of the multilevel and dynamically complex forces impacting broad real-world implementation. Work in this translational stage should focus on identifying and studying the important factors supporting or threatening broad intervention effectiveness and direct change in implementation plans to best support wide-spread implementation. Interdisciplinary teams from diverse settings must be engaged to inform diagrams and research in T3, beyond academic scholars and stakeholders from controlled trial settings. Community leaders, stakeholders with political power, government regulatory officers, key business representatives, front-line staff, and other stakeholders are needed to contribute to the understanding of real-world implementation issues.
In T3, an interdisciplinary team may build on prior translational stage diagrams. For example, Fig. 4 now encapsulates the multi-pronged prevention intervention targeting youth smoking formalized through T0–T2 into one stock—“intervention effectiveness.” This affords the team a broader focus on understanding implementation design problems and variation in factors such as resources or motivation to implement, which might lead to adaptation or confound effectiveness. The same implementation design variables that are key in T2 are important in T3, except that here they are used to inform the design of intervention adaptation planning and support rather than the initial intervention prototype. In T2, many of these factors (i.e., motivation) were externally controlled, by design, in the efficacy trial, and now vary in the real world. Leaders in new communities may raise concerns about the mismatch of intervention strategies (i.e., design problems) that are not aligned with their local cultural values, social norms, or resources. Figure 4 includes stocks for “design problems” and “intervention adaptations.” As mismatch is discovered and local implementers make adaptations, the frequency of implementers experiencing design problems accumulate, with these experiences flowing into the intervention adaptations stock as changes are made. Figure 4 indicates the connection between these adaptations and intervention fidelity, which is improved based on the quality of adaptations.
Fig. 4.

System dynamics diagram illustrating complexity in Type 3 Translation work supporting tobacco prevention. For a larger version of the figure, see Supplementary materials
At this stage, resources to disseminate the intervention across new communities also become a key concern for the interdisciplinary team. Figure 4 reveals important sequences of feedback loops that involve implementation effectiveness, perceived success among implementers, and resources. First, a reinforcing loop highlights how perceived intervention effectiveness changes motivation to implement an intervention, which impacts fidelity and circles back to influence perceived effectiveness (triggering a continuation of the cycle). Thus, a reinforcing loop is created that could either improve or degrade intervention effectiveness. A second reinforcing loop illustrates a common theme seen in many system dynamics projects—increased success of successful interventions. The link between intervention effectiveness and the ability to obtain additional resources influences training and other important factors that ultimately loop back to influence intervention effectiveness (and these cycles continue). Implementers not as successful find it harder and harder to secure requisite resources. A third balancing feedback loop limits the use of resources (i.e., as resources are gained, more staff can be trained, but this requires resources and reduces the stock). Understanding limitations in available resources is critical at this translational stage. A common challenge, funding agencies might not be able to cover the often substantially greater cost of program implementation in T3 (e.g., hiring more teachers to reduce teachers’ burden), rendering funding less adequate compared to more narrow T2 trials. At a qualitative level, diagramming can thus guide thinking about important aspects of implementation design. If diagrams are converted to quantitative simulation models, a team can test, empirically, the factors to which outcomes are most sensitive [65].
Scaling-up intervention: system dynamics and T4 translation
After an intervention has shown effectiveness in the real-world setting, it could be further scaled up. In T4, lessons learned about implementation adoption and institutionalization of new guidelines, practices, and policies from T3 research set the stage for further scaling up at not only the geographical and population scale but also the temporal scale. Are the interventions of interest going to be sustained? A key challenge for prevention science at this stage is policy resistance. Policy resistance is the set of phenomena that offset or undermine intervention, sometimes worsening the problems they are intended to solve [25]. Historically, system dynamics has included considerable focus on understanding issues of policy resistance by expanding the boundary around inquiry and examining potential influences over time.
In terms of tobacco prevention, it is critical to seek input from industry representatives, policymakers, and behavioral economists at this stage. Figure 5 depicts one example of how the interplay of pro- and anti-tobacco norms may influence policy resistance [31, 66]. Policymakers may use Fig. 5 to consider how the level of policy resistance, modeled as a stock, would influence efforts to undermine policies (e.g., increase in alternative tobacco products or illicit supplies) and ultimately hinder progress. Two reinforcing loops influence either an escalation in or diffusion of the level of policy resistance. The strength of either pro- or anti-tobacco norms, respectively, would influence whether escalation or diffusion occurs. The two reinforcing loops have potential to balance each other, essentially stagnating the level of policy resistance. Or, either loop could dominate. A quantified model would improve understanding of which loop has most potential to dominate under which circumstances, answering questions such as “where should we spend our efforts - increasing anti-tobacco norms or decreasing pro-tobacco norms,” e.g., those represented by tobacco industry marketing efforts [21]. A recent example of such debate is occurring around the use of electronic cigarettes. On one hand, the reduction in the number of people who switch from smoking tobacco to less harmful or potentially benign e-cigarettes is positive. On the other hand, the popularity of e-cigarettes promotes norms of smoking and undesirable habits among minors, which could lead to their increased use of e-cigarettes and possible tobacco products in the longer-term. Although diagramming does not provide estimates of the magnitude of policy resistance, it can raise concerns before policy adoption and broad implementation and motivate careful monitoring and plans for timely response should undesired effects occur.
Fig. 5.

System dynamics diagram illustrating complexity in type 4 translation work supporting tobacco prevention. For a larger version of the figure, see Supplementary materials
Changing the world to facilitate greater impact: system dynamics and T5 translation
T5 translation seeks to support sustained and enhanced impact by improving the context in which we intervene and includes fundamental and universal change in attitudes, policies, and social systems that otherwise limit intervention. Work in this stage is done after the intervention has been in place for a while, and it is possible to evaluate lessons learned. The team could consist of any to all participants in previous stages. Continuing with the tobacco prevention example, we focused T5 inquiry on the increasingly important role of community organization in supporting comprehensive tobacco prevention. Figure 6 highlights a reinforcing loop where improvement in shared decision-making strengthens leadership support for policy change, which can increase networking among leaders and the broader community, and will reinforce shared decision-making. This loop pertains to community, state, national, and/or global levels of policy decision-making. Discussion of this diagram forces acknowledgment that different types of policies may compete with each other for resources, and strategic balance must be found (e.g., between regulatory versus prevention program institutionalization policies or supply versus demand-side policies). These balances need to be intentionally preserved as marketing, and political constituency efforts might pitch a particular type of program or intervention [66].
Fig. 6.

System dynamics diagram illustrating complexity in type 5 translation work supporting tobacco prevention. For a larger version of the figure, see Supplementary materials
CONCLUSIONS
In this paper, we sought to illustrate the potential value of including the development of system dynamics diagrams, collaboratively with key stakeholders, as part of translational prevention research, practice, and policy. System dynamics diagramming offers a method for improving documentation, discussion, and integration of evidence about complex systems to support future translation efforts (Fig. 7). Researchers, practitioners, and policymakers’ understanding of the translational context dramatically impacts the quality of strategies, structures, and decision rules guiding translation across all stages. Thus, prevention outcomes are improved directly through enhancing the quality and appropriateness of practice and policy actions as well as indirectly through improving the quality of translational research. Increasing the quality of research improves prevention outcomes in many ways, for example by offering a stronger evidence base about what to do for whom under what circumstances. Higher-quality research also grows knowledge about a translational problem. If researchers, practitioners, and policymakers can translate that knowledge into a better understanding of the translation context into which they will continue to intervene, the quality of their strategies, structures, and decision rules guiding translation is again improved, and a positive, reinforcing cycle can continue.
Fig. 7.

One potential role for system dynamics methods in translational research. For a larger version of the figure, see Supplementary materials
System dynamics diagrams can be quantified, tested, and used to support decision-making across the translation spectrum. Quantification is important for testing, iterating, building confidence in models, and using models to inform prioritization and planning, as dynamically complex system behavior has been shown to be hard to intuit by the un-aided mind [25, 67].
System dynamics methods can also help decision makers determine the best course of action in the context of uncertainty. Stakeholders often possess a diversity of beliefs about the level of (un)desirability of various behaviors, acceptability of intervention, or even how best to intervene when prevention is agreed upon. Such disagreement plagues prevention science with what Vennix refers to as “messy problems”—“less tangible, ill-defined strategic issues…that is, situations in which there are large differences of opinion on the problem or even on the question of whether there is a problem” [68] (p.380). Several additional types of uncertainty that are important include: uncertainties in the data and evidence (e.g., natural variability, measurement, and sampling errors), uncertainty in the nature of causal relationships (e.g., causal mechanisms, association versus causality, strength of intervention effects, presence or strength of feedback loops), or uncertainty in the shape of relationships (e.g., linear, U-shaped, sigmoid). In the context of messy problems, it is even more important that understanding of complex systems be based on integration of science, theory, and lived experience, and that prevention stakeholders are able to critically appraise and collaboratively plan mutually acceptable solutions to pressing problems [66]. System dynamics methods are designed to support the development of a shared understanding of the dynamically complex determinants of an outcome, and once the model is quantified, to support a group in learning about which acceptable solutions will lead to the greatest positive change [24, 28, 69]. The discussion generated through diagramming may sufficiently improve understanding of the problem and next steps in research, practice, and policy work because it forces stakeholders to make their otherwise internal “mental models” (understanding of the system) explicit, and to test and integrate their assumptions with others’ [28]. System dynamics includes a rich history of using models to encourage decision makers and stakeholders to think differently about how the world works and the impact their actions and decisions have on it. The full details of this process (which includes formalized and structured group facilitation methods) can be found elsewhere [32, 34, 36, 70, 71].
We in no way intend to suggest that system dynamics is a “magic bullet” or the only approach for studying complex systems; however, it is a powerful method to add to the translation science tool box. System dynamics is just one example of the larger class of systems science methods that may be useful in translational research, practice, and policy efforts [29, 62, 72, 73]. Another approach, organizational network analysis, has already proven highly relevant to T4 translation and can improve our understanding of the adoption and implementation of evidence-based interventions [74]. Similar to system dynamics, agent-based modeling can be used to test combinations of efficacious intervention strategies in silico, improving our understanding of potential effectiveness prior to costly real-world implementation [75–77]. A National Institutes of Health (NIH) collaborative, the Initiative on the Study and Implementation of Systems, funded to understand tobacco control as a system and assess the value of systems methods concluded: “Integration and synthesis of systems approaches are key to a systems thinking environment for tobacco control, moving toward a more adaptive system that changes public health outcomes. Approaches such as systems organizing, system dynamics modeling, network methods, and knowledge management contain synergies in areas ranging from participatory stakeholder networks to simulation and knowledge environments. Achievement of this goal involves creating a vision, developing capacity, building planning models, and establishing meaningful and adaptive evaluation measurements” [21].
System dynamics and other systems science approaches have great potential value, but should be thoughtfully combined with extant methods. For example, quality improvement and process flow modeling are needed to identify improvement areas that can reduce delays in moving initiatives forward through translational stages [78, 79]. As well, assumptions made within systems science models are supported by traditional (i.e., reductionist) research.
Electronic supplementary material
Below is the link to the electronic supplementary material.
(DOCX 3.22 mb)
Compliance with ethical standards
This article does not contain any studies with human participants performed by any of the authors.
Conflict of interest
The authors declare that they have no competing interests.
Footnotes
Implications
Researchers: System dynamics tools offer an approach to integrating science, data, and stakeholders’ knowledge into explicit and testable mechanistic hypotheses about prevention outcomes that can strengthen research over time and across translational stages.
Practitioners: System dynamics diagrams offer a mechanism for describing practitioners’ understanding of the most important cross-system factors shaping behavioral outcomes, which informs action planning and helps practitioners communicate their intuition about how to improve systems.
Policymakers: System dynamics diagramming creates explicit theories of change that will inform decision-making in the context of dynamically complex systems problems and increase return on investment.
References
- 1.Balas EA, Boren SA. Managing clinical knowledge for health care improvement. In: Bemmel J, McCray AT, editors. Yearbook of Medical Informatics 2000: Patient-Centered Systems. Stuttgart, Germany: Schattauer Verlagsgesellschaft mbH; 2000. pp. 65–70. [PubMed] [Google Scholar]
- 2.Harris JK, Luke DA, Zuckerman RB, et al. Forty years of secondhand smoke research: the gap between discovery and delivery. Am J Prev Med. 2009;36:538–548. doi: 10.1016/j.amepre.2009.01.039. [DOI] [PubMed] [Google Scholar]
- 3.Kreuter MW, Bernhardt JM. Reframing the dissemination challenge: a marketing and distribution perspective. Am J Public Health. 2009;99:2123–2127. doi: 10.2105/AJPH.2008.155218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lenfant C. Shattuck lecture--clinical research to clinical practice--lost in translation? N Engl J Med. 2003;349:868–874. doi: 10.1056/NEJMsa035507. [DOI] [PubMed] [Google Scholar]
- 5.Stevens KR, Staley JM. The Quality Chasm reports, evidence-based practice, and nursing’s response to improve healthcare. Nurs Outlook. 2006;54:94–101. doi: 10.1016/j.outlook.2005.11.007. [DOI] [PubMed] [Google Scholar]
- 6.Fishbein DH, Stahl M, Ridenour T, et al. The Full Translational Spectrum of Prevention Science: Emerging Basic and Applied Research to Support Scaling Up Proven Practices That Prevent Behavioral Health Problems. Trans Behav Med. 2016. [DOI] [PMC free article] [PubMed]
- 7.Centers for Disease Control and Prevention. Best practices for comprehensive tobacco control programs. Atlanta, GA: U.S.: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health;1999.
- 8.Food and Drug Administration Regulations restricting the sale and distribution of cigarettes and smokeless tobacco products to protect children and adolescents. Fed Regist. 1995;11:41314–41451. [PubMed] [Google Scholar]
- 9.Institute of Medicine. State Programs Can Reduce Tobacco Use. Washington DC: National Cancer Policy Board, Institute of Medicine, National Research Council; 2000.
- 10.US Department of Health and Human Services Substance abuse prevention and treatment block grants: Sale or distribution of tobacco products to individuals under 18 years of age (45 CFR Pt. 96) Fed Regist. 1993;58:45156–45174. [Google Scholar]
- 11.Craig MJ, Boris NW. Youth tobacco access restrictions: time to shift resources to other interventions? Health Promot Pract. 2007;8:22–27. doi: 10.1177/1524839905279882. [DOI] [PubMed] [Google Scholar]
- 12.Etter JF. Laws prohibiting the sale of tobacco to minors: impact and adverse consequences. Am J Prev Med. 2006;31:47–51. doi: 10.1016/j.amepre.2006.03.014. [DOI] [PubMed] [Google Scholar]
- 13.Glantz SA. Limiting youth access to tobacco: a failed intervention. J Adolesc Health. 2002;31:301–302. doi: 10.1016/S1054-139X(02)00473-1. [DOI] [PubMed] [Google Scholar]
- 14.Jason LA, Pokorny SB, Muldowney K, et al. Youth tobacco sales-to-minors and possession-use-purchase laws: a public health controversy. J Drug Educ. 2005;35:275–290. doi: 10.2190/1F1R-KGTL-PVDE-V9EJ. [DOI] [PubMed] [Google Scholar]
- 15.O’Loughlin J, Karp I, Koulis T, et al. Determinants of first puff and daily cigarette smoking in adolescents. Am J Epidemiol. 2009;170:585–597. doi: 10.1093/aje/kwp179. [DOI] [PubMed] [Google Scholar]
- 16.Pentz MA, Sussman S, Newman T. The conflict between least harm and no-use tobacco policy for youth: ethical and policy implications. Addiction. 1997;92:1165–1173. doi: 10.1111/j.1360-0443.1997.tb03676.x. [DOI] [PubMed] [Google Scholar]
- 17.Robinson J, Amos A. A qualitative study of young people’s sources of cigarettes and attempts to circumvent underage sales laws. Addiction. 2010;105:1835–1843. doi: 10.1111/j.1360-0443.2010.03061.x. [DOI] [PubMed] [Google Scholar]
- 18.Spivak AL, Monnat SM. Prohibiting juvenile access to tobacco: violation rates, cigarette sales, and youth smoking. Int J Drug Policy. 2015;26:851–859. doi: 10.1016/j.drugpo.2015.03.006. [DOI] [PubMed] [Google Scholar]
- 19.Tworek C, Yamaguchi R, Kloska DD, et al. State-level tobacco control policies and youth smoking cessation measures. Health Policy. 2010;97:136–144. doi: 10.1016/j.healthpol.2010.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.White MM, Gilpin EA, Emery SL, et al. Facilitating adolescent smoking: who provides the cigarettes? Am J Health Promot. 2005;19:355–360. doi: 10.4278/0890-1171-19.5.355. [DOI] [PubMed] [Google Scholar]
- 21.Best A. National Cancer Institute (U.S.). Greater than the sum: systems thinking in tobacco control. Bethesda, MD: National Cancer Institute, U.S. Dept. of Health and Human Services, Public Health Service, National Institutes of Health; 2007. [Google Scholar]
- 22.Marcus SE, Leischow SJ, Mabry PL, et al. Lessons learned from the application of systems science to tobacco control at the National Cancer Institute. Am J Public Health. 2010;100:1163–1165. doi: 10.2105/AJPH.2010.198721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sussman S, Levy D, Lich KH, et al. Comparing effects of tobacco use prevention modalities: need for complex system models. Tob Induc Dis. 2013;11:2. doi: 10.1186/1617-9625-11-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hassmiller Lich K, Ginexi EM, Osgood ND, et al. A call to address complexity in prevention science research. Prev Sci. 2013;14:279–289. doi: 10.1007/s11121-012-0285-2. [DOI] [PubMed] [Google Scholar]
- 25.Sterman JD. Learning from evidence in a complex world. Am J Public Health. 2006;96:505–514. doi: 10.2105/AJPH.2005.066043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cohen IR, Harel D. Explaining a complex living system: dynamics, multi-scaling and emergence. J R Soc Interface. 2006;4:175–182. doi: 10.1098/rsif.2006.0173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Weiner BJ, Lewis MA, Clauser SB, et al. In search of synergy: strategies for combining interventions at multiple levels. J Natl Cancer Inst Monogr. 2012;2012:34–41. doi: 10.1093/jncimonographs/lgs001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hassmiller Lich K, Minyard K, Niles R, et al. System dynamics and community health. In: Burke JG, Albert S, et al., editors. Emerging Methods In. Community Public Health Research: Springer Publishing Company; 2014. [Google Scholar]
- 29.Luke DA, Stamatakis KA. Systems science methods in public health: dynamics, networks, and agents. Annu Rev Public Health. 2012;33:357–376. doi: 10.1146/annurev-publhealth-031210-101222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Levine RL, Fitzgerald HE. Analysis of Dynamic Psychological Systems. New York: Plenum Press; 1992. [Google Scholar]
- 31.Pentz MA. Institutionalizing community-based prevention through policy change. Special CSAP issue. J Commun Psychol. 2000;28:257–270. doi: 10.1002/(SICI)1520-6629(200005)28:3<257::AID-JCOP3>3.0.CO;2-L. [DOI] [Google Scholar]
- 32.Sterman JD. Business Dynamics: Systems Thinking and Modeling for a Complex World. Boston: Irwin/McGraw-Hill; 2000. [Google Scholar]
- 33.Gillen EM, Hassmiller Lich, K., Yeatts KB, et al. Social Ecology of Asthma: Engaging Stakeholders in Integrating Health Behavior Theories and Practice-Based Evidence Through Systems Mapping. Health Educ Behav. 2013 [DOI] [PubMed]
- 34.Hovmand PS, Andersen DF, Rouwette E, et al. Group model-building ‘Scripts’ as a collaborative planning tool. Syst Res Behav Sci. 2012;29:179–193. doi: 10.1002/sres.2105. [DOI] [Google Scholar]
- 35.Richardson, GP. Concept models in group model building. Syst Dyn Rev. 2013; 29: 42-55.
- 36.Richardson GP, Andersen DF. Teamwork in group model-building. Syst Dyn Rev. 1995;11:113–137. doi: 10.1002/sdr.4260110203. [DOI] [Google Scholar]
- 37.Vennix JAM. Group model Building: Facilitating Team Learning Using System Dynamics. Chichester. New York: J. Wiley; 1996. [Google Scholar]
- 38.Shonkoff JP. From neurons to neighborhoods: old and new challenges for developmental and behavioral pediatrics. J Dev Behav Pediatr. 2003;24:70–76. doi: 10.1097/00004703-200302000-00014. [DOI] [PubMed] [Google Scholar]
- 39.Ahmad S. The cost-effectiveness of raising the legal smoking age in California. Med Decis Making. 2005;25:330–340. doi: 10.1177/0272989X05276859. [DOI] [PubMed] [Google Scholar]
- 40.Ahmad S. Increasing excise taxes on cigarettes in California: a dynamic simulation of health and economic impacts. Prev Med. 2005;41:276–283. doi: 10.1016/j.ypmed.2004.10.024. [DOI] [PubMed] [Google Scholar]
- 41.Ahmad S. Closing the youth access gap: the projected health benefits and cost savings of a national policy to raise the legal smoking age to 21 in the United States. Health Policy. 2005;75:74–84. doi: 10.1016/j.healthpol.2005.02.004. [DOI] [PubMed] [Google Scholar]
- 42.Ahmad S, Billimek J. Estimating the health impacts of tobacco harm reduction policies: a simulation modeling approach. Risk Anal. 2005;25:801–812. doi: 10.1111/j.1539-6924.2005.00647.x. [DOI] [PubMed] [Google Scholar]
- 43.Ahmad S, Billimek J. Limiting youth access to tobacco: comparing the long-term health impacts of increasing cigarette excise taxes and raising the legal smoking age to 21 in the United States. Health Policy. 2007;80:378–391. doi: 10.1016/j.healthpol.2006.04.001. [DOI] [PubMed] [Google Scholar]
- 44.Ahmad S, Franz GA. Raising taxes to reduce smoking prevalence in the US: a simulation of the anticipated health and economic impacts. Public Health. 2008;122:3–10. doi: 10.1016/j.puhe.2007.02.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cavana RY, Clifford LV. Demonstrating the utility of system dynamics for public policy analysis in New Zealand: the case of excise tax policy on tobacco. Syst Dyn Rev. 2006;22:321–348. doi: 10.1002/sdr.347. [DOI] [Google Scholar]
- 46.Cavana RY, Tobias MI. Integrative system dynamics: analysis of policy options for tobacco control in New Zealand. Syst Res Behav Sci. 2008;25:675–694. doi: 10.1002/sres.934. [DOI] [Google Scholar]
- 47.Homer J, Hirsch G, Milstein B, Homer J, Hirsch G, Milstein B. Chronic illness in a complex health economy: the perils and promises of downstream and upstream reforms. Syst Dyn Rev. 2007;23:313–343. doi: 10.1002/sdr.379. [DOI] [Google Scholar]
- 48.Houle B, Siegel M. Smoker-free workplace policies: developing a model of public health consequences of workplace policies barring employment to smokers. Tob Control. 2009;18:64–69. doi: 10.1136/tc.2008.026229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lounsbury DW, Hirsch GB, Vega C, et al. Understanding social forces involved in diabetes outcomes: a systems science approach to quality-of-life research. Qual Life Res. 2014;23:959–969. doi: 10.1007/s11136-013-0532-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Mendez D, Alshanqeety O, Warner KE. The potential impact of smoking control policies on future global smoking trends. Tob Control. 2013;22:46–51. doi: 10.1136/tobaccocontrol-2011-050147. [DOI] [PubMed] [Google Scholar]
- 51.Milstein B, Homer J, Briss P, et al. Why behavioral and environmental interventions are needed to improve health at lower cost. Health Aff (Millwood) 2011;30:823–832. doi: 10.1377/hlthaff.2010.1116. [DOI] [PubMed] [Google Scholar]
- 52.Tengs TO, Ahmad S, Moore R, et al. Federal policy mandating safer cigarettes: a hypothetical simulation of the anticipated population health gains or losses. J Policy Anal Manag J Assoc Pub Policy Anal Manag. 2004;23:857–872. doi: 10.1002/pam.20051. [DOI] [PubMed] [Google Scholar]
- 53.Tengs TO, Ahmad S, Savage JM, et al. The AMA proposal to mandate nicotine reduction in cigarettes: a simulation of the population health impacts. Prev Med. 2005;40:170–180. doi: 10.1016/j.ypmed.2004.05.017. [DOI] [PubMed] [Google Scholar]
- 54.Tengs TO, Osgood ND, Chen LL. The cost-effectiveness of intensive national school-based anti-tobacco education: results from the tobacco policy model. Prev Med. 2001;33:558–570. doi: 10.1006/pmed.2001.0922. [DOI] [PubMed] [Google Scholar]
- 55.Tengs TO, Osgood ND, Lin TH. Public health impact of changes in smoking behavior: results from the Tobacco Policy Model. Med Care. 2001;39:1131–1141. doi: 10.1097/00005650-200110000-00010. [DOI] [PubMed] [Google Scholar]
- 56.Tobias MI, Cavana RY, Bloomfield A. Application of a system dynamics model to inform investment in smoking cessation services in New Zealand. Am J Public Health. 2010;100:1274–1281. doi: 10.2105/AJPH.2009.171165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hassmiller Lich K, Osgood N, Mahamoud A. Using system dynamics tools to gain insight into intervention options related to the interaction between tobacco and tuberculosis. Glob Health Promot. 2010;17:7–20. doi: 10.1177/1757975909358255. [DOI] [PubMed] [Google Scholar]
- 58.Killeen PR. Markov model of smoking cessation. Proc Natl Acad Sci U S A. 2011;108(Suppl 3):15549–15556. doi: 10.1073/pnas.1011277108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Niederdeppe J, Avery R, Byrne S, et al. Variations in state use of antitobacco message themes predict youth smoking prevalence in the USA, 1999–2005. Tob Control. 2016;25:101–107. doi: 10.1136/tobaccocontrol-2014-051836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Cavana RY, Tobias M. Integrative system dynamics: analysis of policy options for tobacco control in New Zealand. Syst Res Behav Sci. 2008;25:675–694. doi: 10.1002/sres.934. [DOI] [Google Scholar]
- 61.Milstein B, Homer J, Briss P, et al. Why behavioral and environmental interventions are needed to improve health at lower cost. Health Aff. 2011;30:823–832. doi: 10.1377/hlthaff.2010.1116. [DOI] [PubMed] [Google Scholar]
- 62.Burke JG, Hassmiller Lich K, Neal JW, et al. Enhancing dissemination and implementation research using systems science methods. Int J Behav Med. 2015;22:283–291. doi: 10.1007/s12529-014-9417-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Pentz MA. Form follows function: designs for prevention effectiveness and diffusion research. Prev Sci. 2004;5:23–29. doi: 10.1023/B:PREV.0000013978.00943.30. [DOI] [PubMed] [Google Scholar]
- 64.Jalali MS, Rahmandad H, Bullock SL, et al. Dynamics of obesity interventions inside organizations. Paper presented at: The 32nd International Conference of the System Dynamics Society.2014, July.
- 65.Saltelli A. Global sensitivity analysis : the primer. Chichester, England. Hoboken, NJ: John Wiley; 2008. [Google Scholar]
- 66.Pentz MA, Mares D, Schinke S, et al. Political science, public policy, and drug use prevention. Subst Use Misuse. 2004;39:1821–1865. doi: 10.1081/JA-200033226. [DOI] [PubMed] [Google Scholar]
- 67.Sterman JD. Learning in and about complex systems. Syst Dynam Rev. 1994;10:291–330. doi: 10.1002/sdr.4260100214. [DOI] [Google Scholar]
- 68.Vennix JAM. Group model-building: tackling messy problems. Syst Dyn Rev. 1999;15:379–401. doi: 10.1002/(SICI)1099-1727(199924)15:4<379::AID-SDR179>3.0.CO;2-E. [DOI] [Google Scholar]
- 69.Loyo HK, Batcher C, Wile K, et al. From model to action: using a system dynamics model of chronic disease risks to align community action. Health Promot Pract. 2013;14:53–61. doi: 10.1177/1524839910390305. [DOI] [PubMed] [Google Scholar]
- 70.Vennix JAM, Akkermans HA, Rouwette EAJA. Group model-building to facilitate organizational change: an exploratory study. Syst Dyn Rev. 1996;12:39–58. doi: 10.1002/(SICI)1099-1727(199621)12:1<39::AID-SDR94>3.0.CO;2-K. [DOI] [Google Scholar]
- 71.Ghaffarzadegan N, Lyneis J, Richardson GP. How small system dynamics models can help the public policy process. Syst Dyn Rev. 2011;27:22–44. [Google Scholar]
- 72.Morrissey JP, Lich KH, Price RA, et al. Computational modeling and multilevel cancer control interventions. J Natl Cancer Inst Monogr. 2012;2012:56–66. doi: 10.1093/jncimonographs/lgs014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lich KH, Ginexi EM, Osgood ND, et al. A call to address complexity in prevention science research. Prev Sci. 2013;14:279–289. doi: 10.1007/s11121-012-0285-2. [DOI] [PubMed] [Google Scholar]
- 74.Valente TW, Palinkas LA, Czaja S, et al. Social network analysis for program implementation. PLoS ONE. 2015;10:e0131712. doi: 10.1371/journal.pone.0131712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Marshall BD, Paczkowski MM, Seemann L, et al. A complex systems approach to evaluate HIV prevention in metropolitan areas: preliminary implications for combination intervention strategies. PLoS ONE. 2012;7:e44833. doi: 10.1371/journal.pone.0044833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Gittelsohn J, Mui Y, Adam A, et al. Incorporating systems science principles into the development of obesity prevention interventions: principles, benefits, and challenges. Curr Obes Rep. 2015;4:174–181. doi: 10.1007/s13679-015-0147-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Gittelsohn J, Anderson Steeves E, Mui Y, et al. B’More healthy communities for kids: design of a multi-level intervention for obesity prevention for low-income African American children. BMC Public Health. 2014;14:942. doi: 10.1186/1471-2458-14-942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Trochim W, Kane C, Graham MJ, et al. Evaluating translational research: a process marker model. Clin Transl Sci. 2011;4:153–162. doi: 10.1111/j.1752-8062.2011.00291.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Rajan A, Sullivan R, Bakker S, et al. Critical appraisal of translational research models for suitability in performance assessment of cancer centers. Oncologist. 2012;17:e48–57. doi: 10.1634/theoncologist.2012-0216. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX 3.22 mb)