

Abstract
Various developmental models have attempted to explain the relationship between antisocial behavior and depressive symptoms in youth, often proposing intermediary processes such as social and academic functioning. However, few studies have tested these developmental models fully, particularly in mixed gender samples. The current study strives to fill this gap in the literature, examining these processes in an early adolescent sample. Results indicated both direct and indirect paths between antisocial behavior and depression. In addition, potentially important gender differences were found. These results underscore the importance of examining direct and indirect links between symptoms of depression and anti-social behavior, and suggest that there may be important developmental differences between girls and boys in the relationship between these symptoms.
Keywords: depression, conduct disorder, dual-failure model, gender differences, developmental psychopathology
A multitude of studies have found significant overlap between symptoms of depression and conduct disorder beyond what would be expected by chance, at both the clinical and subclinical levels (Angold, Costello, & Erkanli, 1999; Capaldi, 1991). However, the direction of influence between these two symptom clusters over time is not well understood. For instance, a number of longitudinal studies with both clinic-referred and community samples have found that conduct problems often precede depression (e.g. Biederman, Faraone, Mick, & Lelon, 1995; Capaldi, 1992; Moffitt, Caspi, Rutter, & Silva, 2001; Moilanen et al, 2010; Nock et al., 2006), although other studies have failed to support this link (e.g. Beyers & Loeber, 2003). Conversely, some research has suggested that symptoms of depression may precede conduct problems (Capaldi & Stoolmiller, 1999; Curran & Bollen, 2001; Kovacs et al, 1988), and that earlier symptoms of depression are associated with more serious delinquency over time (Beyers & Loeber, 2003). Finally, bidirectional relations between depression and conduct problems over time have also been found (e.g. Wiesner, 2003).
Several models have been put forth to describe the pathways through which conduct problems may lead to depression, and vice versa. The dual-failure model, for instance, holds that conduct problems are associated with a number of negative sequelae, including poor academic functioning, peer rejection, and increased family conflict (Capaldi, 1991, 1992). These failure experiences, in turn, leave the adolescent more vulnerable to the development of depressive symptoms. Conversely, other models focus on depression predicting later conduct problems. For instance, an irritable depression model suggests that youth may express the irritability associated with depression through acting out with family and peers, leading to escalating conduct problems over time (Wolff & Ollendick, 2006). In line with this model, Hipwell and colleagues (2011) found that developmental relations between earlier depression and later conduct problems in a longitudinal sample of girls were attenuated when controlling for emotional dysregulation associated with oppositional defiant disorder, suggesting that such irritability may explain, in part, the effect of depression on CD in girls. Further, the social difficulties commonly experienced by depressed youth may lead them to gravitate into deviant peer networks in which they are reinforced for acting out, leading to escalating conduct problems (e.g. Connell & Dishion, 2006). Models such as these are important because they may suggest targets for prevention efforts to disrupt processes leading to co-occurring emotional and behavioral difficulties. Very few studies, however, have provided a comprehensive examination of these models, although a number of studies have examined specific pathways. These social relational and academic pathways are reviewed, followed by a review of possible gender differences in the developmental links between conduct problems and depression.
Social Functioning
The dual-failure model predicts that peer rejection partially mediates the relationship between conduct problems and later depressive symptoms. Indeed, research has shown that early conduct problems predict later peer rejection (e.g. Coie, Dodge, & Kupersmidt, 1990), and that peer rejection and relational problems, in turn, are associated with increased depressive symptoms (Chen et al, 1995; Hawker & Boulton, 2000; Rudolph, Hammen, & Burge, 1994; Zwierzynska, Wolke, & Lereya, 2013). In a partial test of the dual-failure model, Kiesner (2002) found that behavior problems and popularity were both predictive of future depressive symptoms, although popularity with peers did not mediate the relationship between antisocial and depressive symptoms.
Theories that posit that symptoms of depression precede the development of conduct problems also identify peer processes, including peer rejection and deviant peer relationships, as mediating variables. Consistent with this model, depressive symptoms have been found to be a risk factor for peer relationship difficulties (Kochel, Ladd, & Rudolph, 2012), as well as for increased deviant peer association (Fergusson et al, 2003). Deviant peer association, in turn, predicts increased antisocial behavior (Monahan, Steinberg, & Cauffman, 2009; Toro, Urberg, & Heinze, 2004). In addition, Burke and colleagues (2005) found in their all male sample that psychosocial impairment mediated the relationship between symptoms of depression and subsequent symptoms of conduct disorder (although the impairment variable in this study included both peer relational and academic problems). Again this relationship may be bidirectional, as association with deviant peers has been shown to predict subsequent elevations in depressive symptoms (Connell & Dishion, 2006). Indeed, reciprocal influences appear to be common. For example, in their meta-analysis, Reijntjes et al (2011) concluded that peer victimization serves as both an antecedent and a consequence of externalizing behavior.
Academic Functioning
Cross-sectional research has found that academic functioning is correlated with both conduct problems and depression (e.g. Nelson, Benner, Lane, & Smith, 2004; Diego, Field, & Sanders, 2003). Consistent with the dual-failure model, several longitudinal studies have found support for temporal relations between conduct problems and academic competence. For instance, Moilanen, Shaw, and Maxwell (2010) found that externalizing problems at ages 6 and 8 were related to decreases in academic competence at ages 8 and 10, which, in turn were related to increased internalizing symptoms at ages 10 and 11 respectively. Similarly, Masten and colleagues (2005) found that early externalizing symptoms (assessed between 8 to 12 years) predicted lower academic competence in adolescence, which in turn predicted heightened internalizing symptoms in adulthood (age 30). Additionally, McCarty and colleagues (2008), found that conduct problems for boys in late childhood were predictive of school failure in adolescence, and that school failure during adolescence was predictive of a depressive episode in young adulthood for females, supporting pieces of the dual-failure model. Similarly, although not examining earlier conduct problems, Schwartz, Gorman, Duong, and Nakamoto (2008) found that low academic achievement was predictive of depressive symptoms only for children who had few friends.
Fewer studies have examined the longitudinal relations between depression and academic difficulties, and the results of those studies have been mixed. For instance, Quiroga and colleagues (2013) found that depressive symptoms in 7th grade predicted lower self-reported academic competence across adolescence, and in turn, a higher likelihood of dropping out of school by 11th grade. Similarly, in a two year longitudinal study with children between second and 4th grade, Chen, Rubin, & Li (1995) found that academic success was negatively correlated with depressive symptoms, while a decline in academic performance was correlated with an increase in depressive symptoms (Chen, Rubin, & Li, 1995). Conversely, the aforementioned study by Masten and colleagues (2005) did not find evidence of early internalizing symptoms predicting academic problems over time. Similarly, Cole and colleagues (1996) found that while depression and academic competence were correlated, depression was not predictive of academic competence after controlling for baseline levels of competence, and academic competence was not predictive of depressive symptoms after controlling for baseline depression levels.
The role of gender
There may be important gender differences in the direction of the relationship between depressive symptoms and behavior problems. For instance, while many studies have found support for aspects of the dual-failure model, these studies often examined purely male samples (e.g. Capaldi 1991, 1992; Patterson & Stoolmiller, 1991). Studies that have included mixed-gender samples have found important gender differences in relations between conduct problems and depression. For instance, Kofler and colleagues (2011) found that early depressive symptoms were a stronger risk factor for delinquent behavior in females than in males. Similarly, Wiesner (2003) found that while early delinquency predicted later depression for boys across adolescence, bidirectional relations were found across 4 assessment waves for girls, with both delinquency predicting subsequent depression and depression predicting increases in subsequent delinquency. Further, females with conduct disorder are more likely to exhibit comorbid depression, a finding consistent with the “gender paradox” theory, which posits that when symptoms of a disorder occur with differential frequency in one sex, members of the group with the lower prevalence rate will be more severely affected (see Keenan, Loeber, & Green, 1999; Loeber and Keenan, 1994).
In addition, the intervening processes in the relationship between depression and behavior problems may vary by gender. For example, some research suggests that interpersonal relationships appear to be more important in the expression and course of conduct problems for females than for males (Ehrensaft, 2005). Conversely, Toro et al (2004) found that the relationship between deviant peer association and antisocial behavior was stronger in males than females. Further, males show higher rates of behavior problems in late childhood, and while this type of behavior is negatively related to academic achievement in males, internalizing problems are more strongly related to academic achievement in females (Moilanen et al, 2010). In addition, while depressive symptoms are related to self-perceptions of academic and social competence in males, others’ perceptions of competence are related to self-perceptions in these areas in females (Cole et al, 1997).
Thus, there is a small body of literature suggesting that there may be important gender differences in the direction of influence between symptoms of depression and behavior problems, however more research using large samples that include females is needed. It is especially important to examine gender differences in studies using dimensional symptom counts, as is done in the current study. Research using diagnostic categories would not be able to examine the potentially important and nuanced gender differences that can be captured using dimensional counts. This is due to the fact that individuals at this age are not likely to meet actual diagnostic criteria, and those that do are not likely to be a representative sample. In addition, males and females are likely to meet criteria for different disorders at this age, even though they may have symptoms of more than one disorder. Because of this, stronger gender effects may be found in diagnostic studies and thus theories developed using only these types of studies may be somewhat misleading.
The Current Study
While a number of studies have examined pieces of the dual-failure and irritable depression models, few studies have been conducted that can examine the full pathways between conduct problems and depression over an extended period of time. Further, alternative models suggest conflicting developmental process. The current study offers advantages over previous studies of the developmental relations between depression and conduct problems by examining multiple, theoretically-important intervening processes in a community-based, mixed-gender sample followed across a 4-year time period in early adolescence. We examined a comprehensive set of measures of domains of the dual-failure and irritable depression models, including depressive symptoms, antisocial behavior, academic achievement, and aspects of social functioning. Aspects of social functioning include teasing by peers as well as deviant peer affiliation, which is important because of its relation to variation in levels of depressive symptoms (Connell & Dishion, 2006) as well as its relation to antisocial behavior (Monahan, Steinberg, & Cauffman, 2009; Toro, Urberg, & Heinze, 2004). By including multiple intervening processes within a cross-lagged panel model design, we were able to examine intermediary processes between depression and conduct problems over time, and to examine whether such intervening processes may differ for males and females.
The data used in this study were taken from a large school-based intervention trial. Previous studies have reported that the intervention predicted lower rates of substance use and antisocial behavior among youth whose families complied with the Family Check-Up (Stormshak et al, 2011). However these treatment effects were found only when examining sample subgroups using Complier Average Causal Effect analyses. Past analyses have shown no significant treatment effects for the overall sample using an Intent To Treat analytic approach (Connell, Dishion, & Stormshak, 2013; Connell, Stormshak, & Dishion, 2014; Connell, Stormshak, & Dishion, 2009). This suggests that the subgroup treatment effects are unlikely to translate into the cross-lagged paths we are examining in the present study. Thus the current study used data from the control and intervention groups combined. This approach is consistent with that used in similar longitudinal studies examining developmental questions in treatment samples (Dishion, Veronneau, & Myers, 2010; Murray-Close et al, 2010).
The current study had the following goals. First, we sought to examine gender differences in the direction of relations between depression and conduct problems. In line with Kofler and colleagues (2011), and Wiesner (2003), we predicted that depressive symptoms would be stronger predictors of later conduct problems for females, while the reverse would be true for males. Second, we sought to examine social and academic pathways between conduct problems and depression. Consistent with the dual-failure model, we hypothesized that for males, early externalizing symptoms would be associated with problems in academic and social functioning, leading in turn to increased depressive symptoms. Conversely, based on the findings of Ehrensaft (2005), we predicted that peer relational difficulties, such as peer teasing and peer deviance, would play a more prominent intermediary role for females than for males.
Method
Participants
Participants were recruited from three public middle schools in an urban area. All families with a child in the sixth grade were invited to participate, which translated to a total of 782 families. Of those, 593 families agreed to take part in the study, for an enrollment rate of 76%. The sample was 51% male and represented a wide variety of ethnic backgrounds (36% European American, 18% Hispanic/Latino, 15% African American, 7% Asian, 19% biracial/mixed identity, 2% Pacific Islander, 2% Native American). The average age of participants was as follows: 11 years 10 months (wave 1), 13 years 1 month (wave 2), 14 years 1 month (wave 3), and 15 years (wave 4). 80% of participants’ fathers and 79% of mothers had attained at least a high school diploma. 65% of participating children reported feeling that their family had adequate financial resources. 87% of children stated that they felt their neighborhood was safe or very safe, and 64% of children reported feeling safe at school often or always. Those families who agreed to participate were randomly assigned to receive the intervention (N = 386; 65%) or “school as usual” (N = 207; 35%). Randomization was done using an unbalanced approach to increase the power to detect heterogeneous patterns of intervention effects.
Assessment procedures
Every spring from the sixth through the ninth grade, student participants completed a questionnaire that assessed a wide range of domains. This questionnaire was adapted from Metzler and colleagues (2001). Assessments were conducted in the school. If a child was absent or the family had moved out of the school district, assessments were mailed to the home. Students received $20 for each completed assessment. Measures used in this study are briefly described below. Further details regarding these measures have been included in previous publications (Dishion & Kavanagh, 2003; Dishion & Stormshak, 2007).
Measures
Adolescent antisocial behavior
Antisocial behavior was measured by adolescent self-report each year of the study. Eleven items assessed participation in activities during the past month, including lying, theft, getting into physical fights, carrying weapons, and destroying property. Responses on the measure ranged from 0 (never) to 5 (more than 20 times), and the average was used in this study. In the current study, Cronbach’s alpha was between 0.82 and 0.86 for this measure across the four waves of data.
Adolescent depressive symptoms
Depressive symptoms were assessed annually using a 14-item measure. Adolescents were asked about the frequency of symptoms such as feeling sad, moody, or hopeless and having trouble sleeping, with all diagnostic criteria for depression addressed by at least one item. Participants rated each symptom on a 5-point scale that ranged from “never or almost never” to “always or almost always” for the past month, and the average across items was used in analyses. This measure has been shown to have high internal reliability (Stormshak, Fosco, & Dishion, 2010). In the current study, Cronbach’s alpha was between 0.92 and 0.95 for this measure across the four waves of data. In addition, a subset of the sample completed the Child Depression Inventory (CDI) in the first two waves of the study, and the average CDI item score was significantly correlated to the average depressive symptom score used in these analyses (r = .49 and .53 for waves 1 and 2 respectively).
Peer victimization
Each year, youth responded to 7-items reflecting the frequency with which they were the target of such behaviors as being teased for the clothing they wear or for being a good student, over the past month. Each item was rated on a 5-point scale from “never” to “always” and the average across items was used in analyses. Cronbach’s alpha was between 0.81 and 0.84 for this measure across the four waves of data.
Peer deviance
Association with deviant peers was assessed annually using 5 items that asked each youth to report how often they spent time with friends who in the past month had engaged in such behaviors as stealing, lying, and fighting. Items were rated on a 5-point scale from “never” to “more than 7 times,” and the average score was used in analyses. Cronbach’s alpha was between 0.73 and 0.86 for this measure across the four waves of data.
Academic performance
An estimate of each child’s academic performance during the current school year was obtained annually with one item that asked the child to rate her performance on a 5-point scale, where 1 represented “mostly A’s” and 5 represented “mostly F’s.” There was also an option for “not in school,” although no participants endorsed this item. In support of the validity of this academic performance estimate, scores on this item were significantly correlated with school-reports of standardized testing in math and reading subjects which were available in waves 1 – 3 (correlations ranged from -.29 to-. 48, with youth reporting better grades tending to score higher on standardized tests). Because testing results were not available for all study waves, however, we used youth-reports in the current analyses.
Gender
The gender of the child was coded as 0 = male and 1 = female.
Ethnicity
A dichotomous score reflecting youth reports of ethnicity was used in current analyses, with 0 = ethnic minority and 1 = Caucasian.
Intervention Protocol
The current study made use of a dataset taken from a randomized, school-based prevention trial. The prevention program was a multilevel, school-based intervention (see Dishion & Kavanagh, 2003). The first level was the family resource center (FRC), which was established in each school taking part in the study and was available to all families assigned to the intervention condition. The next level of the intervention was the Family Check-Up (FCU), which is based on motivational interviewing and uses the Drinker’s Check-Up (Miller & Rollnick, 2002) as a model. This too was offered to all families in the intervention condition, and included three sessions: an initial home visit and interview, an ecological assessment, and finally a feedback session. For a more thorough explanation of the intervention, see Dishion and Kavanagh (2003) or Stormshak, Fosco, and Dishion (2010). Most families in the intervention group chose not to take advantage of the services offered or only participated in the low intensity universal intervention.
Analytic Approach
The analyses for this study were conducted using Mplus 7.1 (Muthen & Muthen, 2013). A series of cross-lagged path models were used to test hypotheses. Ethnicity was included as a covariate in all analyses by regressing time 1 variables on ethnicity. First, possible differences across treatment and control conditions were examined using a series of nested models to determine if the paths examined in this study were equal across the control and intervention groups. We compared a model in which all paths were constrained to be equal across intervention and control conditions with one in which all paths were allowed to vary by intervention status, with the difference tested via chi-square difference test. Second, we examined possible gender differences using a similar nested model comparison approach, comparing a model in which paths were allowed to vary across genders with a model in which paths were constrained to be equal for males and females. This test provides an overall examination of gender as a moderator of the relations between depression and antisocial behavior. Third, we conducted follow-up analyses to examine gender differences in specific paths, using model constraints in Mplus. Finally, we examined indirect paths from depression to antisocial behavior, and vice versa, with standard errors for indirect effects calculated using the delta method described by MacKinnon and colleagues (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002; MacKinnon, Lockwood, & Williams, 2004). We limited our examination of indirect paths in the models to those focused on the relations between depression and antisocial behavior over time.
Results
Descriptive Statistics
The mean number of symptoms present at each assessment point is presented in Table 1 by gender, and bivariate correlations are shown in Table 2. Repeated measures ANOVAs were used to examine gender differences in mean symptom levels over time. Results indicated significant interactions between depressive symptoms and gender, such that females had significantly higher levels of symptoms in grades 7, 8, and 9, F(1, 428) = 32.48, p < .05. The opposite pattern was observed for antisocial behavior. Across the four waves, males’ level of antisocial behavior was higher than females’, though this difference reached significance only at grade 7, F(1, 428) = 2.57, ns. For deviant peer association, the only significant difference was at grade 6, when males reported a higher frequency than females, F(1, 433) = .01, ns. Males also reported being a target for teasing more frequently than females at grade 6, F(1, 435) = 1.6, ns. Finally, there was a significant interaction between gender and academic performance, such that at each time point females had significantly higher academic performance than males, F(1, 424) = 12.33, p < .05. Table 2 shows significant correlations for the majority of the variables across all 4 waves of the study. However, correlations between peer victimization and academic performance were not significant past grade 6.
Table 1.
Means (Standard Deviations) of Study Variables
| Grade 6 | Grade 7 | Grade 8 | Grade 9 | |||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | |
| Depression | 1.80 (.75) |
1.89 (.80) |
1.76 (.72) |
2.05 (.84) |
1.71 (.68) |
2.23 (.95) |
1.74 (.72) |
2.16 (.89) |
| Antisocial Behavior | 1.22 (.43) |
1.15 (.29) |
1.30 (.50) |
1.21 (.35) |
1.35 (.55) |
1.29 (.42) |
1.33 (.50) |
1.31 (.41) |
| Deviant Peers | .70 (1.04) |
.50 (.74) |
1.06 (1.36) |
.93 (1.23) |
1.20 (1.55) |
1.33 (1.48) |
1.33 (1.59) |
1.59 (1.69) |
| Teasing | 1.72 (.70) |
1.58 (.66) |
1.65 (.71) |
1.63 (.67) |
1.50 (.60) |
1.54 (.58) |
1.47 (.60) |
1.39 (.49) |
| Academic Performance | 2.16 (1.12) |
1.89 (1.0) |
2.32 (1.13) |
1.89 (.97) |
2.29 (1.09) |
1.95 (.99) |
2.49 (1.18) |
2.27 (1.16) |
Table 2.
Over-time Correlation Matrix
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Depression wave 1 | – | ||||||||||||||||||
| 2. Antisocial wave 1 | .2 4* | – | |||||||||||||||||
| 3. Deviant peers wave 1 | .1 7* | .5 4* | – | ||||||||||||||||
| 4. Teasing wave 1 | .3 2* | .2 0* | .1 0* | – | |||||||||||||||
| 5. Poor grades wave 1 | .0 9* | .2 6* | .2 4* | .1 2* | – | ||||||||||||||
| 6. Depression wave 2 | .4 5* | .1 7* | .1 2* | .2 2* | .1 1* | – | |||||||||||||
| 7. Antisocial wave 2 | .1 6* | .3 7* | .4 7* | .0 4 | .2 2* | .2 1* | – | ||||||||||||
| 8. Deviant peers wave 2 | .1 0* | .2 7* | .4 4* | .0 2 | .1 9* | .2 0* | .6 7* | – | |||||||||||
| 9. Teasing wave 2 | .3 0* | .0 5 | .0 2 | .5 2* | .0 5 | .4 2* | .0 2 | −.0 1 | – | ||||||||||
| 10. Poor grades wave 2 | .02 | .1 1* | .0 8 | −.0 9* | −.1 0* | .0 9* | .1 4* | .0 5 | −.0 6 | – | |||||||||
| 11. Depression wave 3 | .3 4* | .1 7* | .1 2* | .1 8* | .0 5 | .5 1* | .1 7* | .1 9* | .2 5* | .0 3 | – | ||||||||
| 12. Antisocial wave 3 | .1 1* | .2 8* | .3 6* | .0 6 | .1 6* | .1 6* | .5 9* | .4 8* | −.0 3 | .0 7 | .3 1* | – | |||||||
| 13. Deviant peers wave 3 | .05 | .2 1* | .3 6* | .0 5 | .1 4* | .0 8 | .5 2* | .6 0* | −.0 9* | .0 8 | .2 2* | .63* | – | ||||||
| 14. Teasing wave 3 | .2 9* | .1 1* | .0 9* | .4 4* | .0 3 | .2 9* | .0 8 | .0 4 | .6 2* | −.0 1 | .3 7* | .11* | .0 5 | – | |||||
| 15. Poor grades wave 3 | .1 2* | .2 1* | .2 0* | .1 2* | .4 6* | .1 2* | .2 9* | .2 6* | −.0 1 | .0 7 | .0 8 | .24* | .31* | −.0 1 | – | ||||
| 16. Depression wave 4 | .2 9* | .1 7* | .1 4* | .1 7* | .0 4 | .4 7* | .1 3* | .1 0* | .2 1* | .0 5 | .6 4* | .17* | .13* | .27* | .12* | – | |||
| 17. Antisocial wave 4 | .0 9* | .1 5* | .2 2* | .0 8 | .0 6 | .1 0* | .4 6* | .4 0* | .0 4 | .0 8 | .1 9* | .54* | .37* | .0 9 | .21* | .22* | – | ||
| 18. Deviant peers wave 4 | .1 2* | .1 3* | .2 5* | .0 7 | .0 2 | .1 9* | .3 5* | .4 1* | .0 4 | .13* | .2 6* | .34* | .44* | .12* | .17* | .28* | .5 6* | – | |
| 19. Teasing wave 4 | .2 4* | .0 8 | .1 0* | .3 3* | −.0 1 | .2 7* | .0 6 | .0 3 | .5 1* | .0 0 | .2 2* | .12* | .0 3 | .51* | .0 0 | .20* | .2 1* | .1 7* | – |
| 20. Poor grades wave 4 | .03 | .1 8* | .1 8* | .1 4* | .4 0* | .1 1* | .2 4* | .2 3* | .0 5 | .0 4 | .0 7 | .19* | .25* | .0 3 | .54* | .18* | .2 6* | .2 0* | .0 5 |
p < .05
Cross-lagged Models
First, a series of nested models was run to determine if the paths examined in this study were equal across the control and intervention groups. Results of a chi-square difference test were not significant (χ2diff (35) = 34.29, n/s), indicating that allowing paths to vary across intervention conditions did not lead to significantly improved fit. As such, subsequent analyses combined intervention and control groups, although intervention status was included as a covariate to control for any possible effects of intervention on outcomes (no significant intervention effects were observed). Next, a model in which all paths were constrained to be equal across time points was compared to one in which paths were allowed to vary. Results of a chi-square difference test were significant, (χ2diff (140) = 278.74, p < .05), indicating that the model in which paths were allowed to vary across time points had a significantly better fit. Finally, a nested model comparison examined if results were consistent across males and females. Results of a chi-square difference test were significant (χ2diff (35) = 107.74, p < .05), indicating a better model fit when paths were allowed to vary by gender. This model fit the data well χ2 (180) = 374.07, p < .05 (CFI = .95, TLI = .88, RMSEA = .06). For the sake of clarity, significant paths of the cross-lagged panel models are shown separately for males (Figure 1) and females (Figure 2). For both males and females, Caucasian youth reported lower levels of antisocial behavior relative to ethnic minority youth (male: beta = −.15, SE = .03; female: beta = −.11, SE = .04) and peer deviance at time 1 (male: beta = −.28 SE = .12; female: beta = −.27, SE = .09). For females, Caucasian youth also reported better academic performance than minority youth (beta = −.70, SE = .12).
Figure 1.
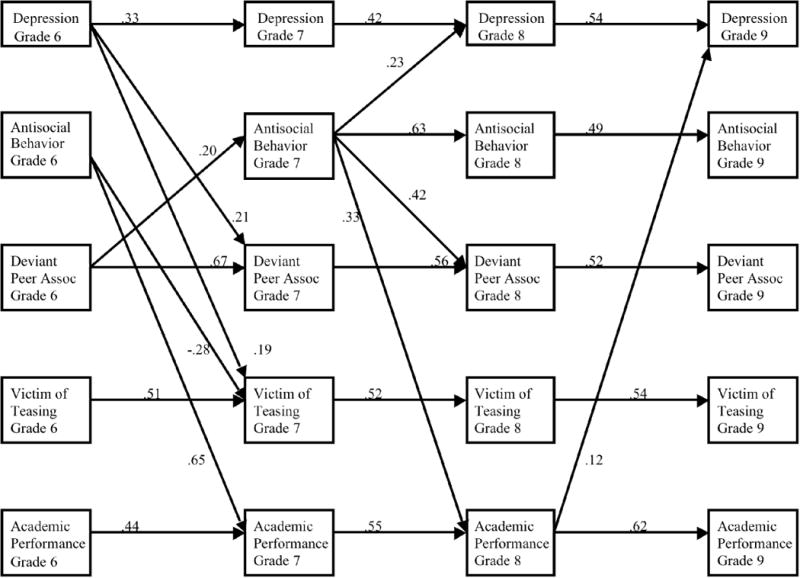
Cross-lagged Panel Model for Males.
Figure 2.
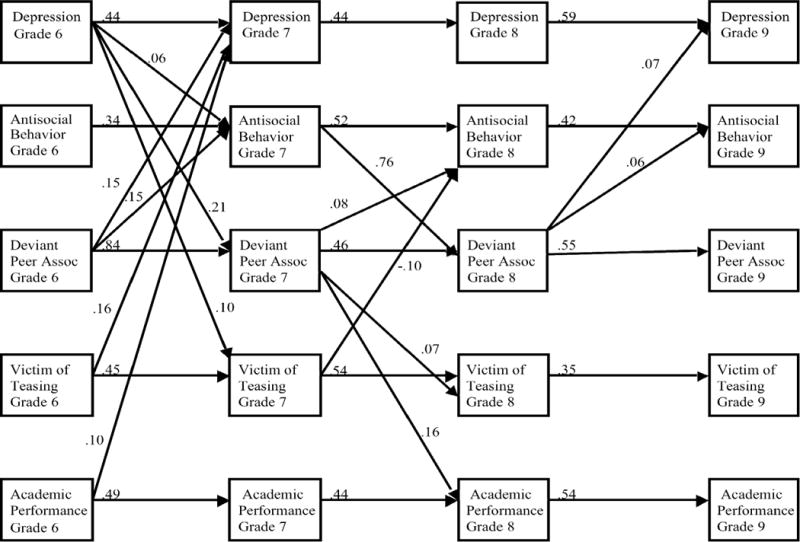
Cross-lagged Panel Model for Females.
Specific paths
For males, depression at grade 6 predicted association with deviant peers and being a target of teasing at grade 7, while antisocial behavior at grade 6 predicted lower levels of academic performance as well as less teasing at grade 7. Peer deviance at grade 6 predicted greater antisocial behavior at grade 7. At grade 7, antisocial behavior predicted greater symptoms of depression and association with deviant peers, as well as poor academic performance at grade 8. Poor academic performance at grade 8, in turn, was related to higher symptoms of depression at grade 9. Tests of gender differences in specific paths indicated several paths were significantly stronger in males than females, including the path from poor academic performance in grade 8 to depression at grade 9, the stability of academic problems from grade 7 to 8, the stability of teasing from grade 8 to 9, the path from antisocial behavior at grade 7 to teasing at grade 8, and the path from peer deviance at grade 6 to academic problems at grade 7 (the latter two paths were at trend-level for males and so are not shown in Figure 1).
For females, depression at grade 6 predicted increases in association with deviant peers and in experiences of peer victimization. Unlike males, however, depression at grade 6 also directly predicted increased symptoms of antisocial behavior at grade 7. In addition, association with deviant peers at grade 6 predicted higher levels of depression and antisocial behavior at grade 7. Academic problems at grade 6 also predicted greater depression at grade 7. Grade 7 antisocial behavior predicted higher levels of association with deviant peers at grade 8, while association with deviant peers at grade 7 predicted greater antisocial behavior and more teasing as well as poorer academic performance at grade 8. At grade 8, association with deviant peers predicted greater levels of antisocial behavior at grade 9. Tests of gender differences in specific paths indicated that the following paths were significantly stronger in females than males: the stability of antisocial behavior from grade 6 to 7, the path from peer deviance at grade 6 to depression at grade 7, the paths from peer deviance at grade 7 to antisocial behavior, teasing, and academic problems at grade 8; the paths from peer deviance at grade 8 to depression and antisocial behavior at grade 9, and the path from grade 6 teasing to grade 7 peer deviance (this path was at trend level and so is not shown on figure 2).
Indirect effects
Finally, we examined indirect pathways between depression and antisocial behavior for boys and girls. For males, several significant indirect paths were found. Antisocial behavior at grade 6 had a significant indirect effect on depressive symptoms at grade 9, via academic performance in grades 7 and 8 (estimate = .04, SE = .02, p < .05). Further, the indirect effect of antisocial behavior at grade 7 on depressive symptoms at grade 9 via depressive symptoms at grade 8 was significant (estimate = .12, SE = .06, p < .05). Finally, there was a significant indirect effect of grade 6 peer deviance on grade 8 depression via grade 7 antisocial behavior (estimate = .05, SE = .02, p < .05).
For females, the overall indirect effect of depressive symptoms at grade 6 on antisocial behavior at grade 8 was significant (estimate = .06, SE = .02, p < .05), with depressive symptoms at grade 6 predicting antisocial behavior at grade 8 via antisocial behavior at grade 7 (estimate = .03, SE = .01, p < .05), and association with deviant peers at grade 7 (estimate = .02, SE = .01, p <.05). The indirect effect of grade 6 depression on grade 8 antisocial behavior via grade 7 teasing approached significance (estimate = −.01, SE = .01, p =.08). The overall indirect effect of depressive symptoms at grade 6 on antisocial behavior at grade 9 (estimate = .04, SE = .01, p < .05) was also significant. More specifically, this path was effected by antisocial behavior at grades 7 and 8 (estimate = .01, SE = .01, p < .05).
Discussion
While a wealth of literature has highlighted that depression and conduct problems are interrelated across adolescent development, questions remain regarding the direction of influences across these domains, processes that may explain these interrelations, as well as gender differences in these pathways. The goal of this paper was to examine the intermediary processes linking symptoms of depression and conduct disorder across early adolescence in a community-based, mixed gender sample. The hope was to add to the body of research examining alternative theories of these processes and attempting to establish the nature of the relationship between these two symptom groups. Broadly, our results were generally consistent with those of Kofler and colleagues (2011), and Wiesner (2003), as conduct problems appeared to precede depression for boys, while depression appeared to precede conduct problems for girls. Thus, models of developmental processes used in this study indicated that there are important differences between girls and boys in the broad direction of the relationship between symptoms of depression and conduct disorder over time, and that different models may need to be applied to males and females.
For boys, two paths from earlier conduct problems to depressive symptoms at grade 9 were observed, including a direct path from conduct problems at grade 7 to depression at grades 9 via depression at grade 8, as well as a path from conduct problems at grade 6 to academic difficulties at grade 7 and 8, and then to depression at grade 9. This latter path is notable, as it is consistent with the dual-failure model, highlighting that boys exhibiting disruptive behavior problems are at risk for academic difficulties in adolescence, and that such difficulties, in turn, heighten the risk for developing problems with depression. In light of this academic-difficulties pathway, prevention programs incorporating a focus on building academic skills for boys may be particularly valuable in disrupting the spread of problems from early antisocial behavior to later problems with depression. It is worth highlighting that academic difficulties were also associated with depression in girls, albeit somewhat earlier (with academic problems in 6th grade predicting depression in 7th grade for girls), and not linked to prior behavior problems. Thus, building academic skills for girls may help to disrupt the earlier development of problems with depression.
For girls, significant indirect paths went from earlier problems with depression to later problems with antisocial behavior—no significant indirect paths went in the reverse direction. Depression in 6th grade predicted increased antisocial behavior, greater affiliation with deviant peers, and more frequent teasing by peers at 8th grade, and these factors predicted increased antisocial behavior at 9th grade, in turn (although the indirect effect of teasing was only at trend level, and so should be interpreted cautiously). These paths are broadly consistent with the irritable depression model, which suggests that depression may heighten peer difficulties, which in turn may predict increases in behavioral difficulties. Similar relations between depression and deviant peer association were reported by Connell & Dishion (2006), who hypothesized that such peer relationships may provide depressed adolescents with at least some camaraderie, despite carrying potential risks for antisocial behavior development. Further, tests of individual paths generally suggested that peer deviance may be a stronger factor in developmental transitions for girls than boys, as peer deviance predicted escalations in depression in 7th grades and 9th grades for girls, as well as increases in antisocial behavior in 8th and 9th grade that were significantly stronger for girls than boys. Similarly, peer deviance in 7th grade was more strongly related to later teasing and academic problems in girls relative to boys. Collectively, the pattern of results suggests that interpersonal targets may be particularly salient in prevention programs targeting early adolescent girls. Prevention efforts targeting deviant peer processes may be particularly warranted for girls in adolescence, given their central role in the spread of problems from depression for girls across this age range.
It is worth highlighting that peer deviance in 7th grade was predicted by depression in males, as well (although the pathway from peer deviance to later antisocial behavior was specific to females). Further, an indirect pathway from peer deviance in 6th grade to later depression via 7th grade antisocial behavior was observed in boys. This pathway is partially consistent with the failure model in highlighting that peer relational difficulties are an important part of the developmental relations between earlier antisocial behavior and later depression for boys. In addition, we found that antisocial behavior in 6th grade was not significantly related to antisocial in 7th grade, controlling for 6th grade peer deviance. This finding may further underscore the central role of peer deviance in the etiology of early antisocial behavior in boys. Finally, it is worth noting that depression predicted increased teasing for boys in 7th grade (as it did for females), while boys’ antisocial behavior in 6th grade predicted decreased teasing, suggesting that such behavior may be reinforced for boys in early adolescence. Thus, although a number of peer relational pathways were weaker for boys than girls, some overlap in pathways across genders was observed, highlighting the importance of targeting peer processes for boys, too.
There are a number of possible reasons why these gender differences in developmental processes may emerge. Several authors (e.g. Wiesner, 2003; Broidy et al, 2003) suggest that gender socialization may play a role. As Wiesner (2003) explains, the fact that females are socialized to be more nurturing and passive, combined with the fact that socialization pressures increase during adolescence, could explain why gender differences emerge in this age range. If females are socialized to value interpersonal relationships more than males, then perhaps as they age interpersonal factors, such as stressful life events, quality of peer relationships, and family support, become more important in influencing the development of psychopathology in females than in males. In other words, as children age boys’ self-perceptions may be more reflective of internal states, while girls’ self-perceptions may be more reflective of others’ perceptions, particularly those of peers (Cole et al, 1997). Further, Broidy and colleagues (2003) suggest that differential socialization drives females to exhibit their deviant behavior differently than males do, in ways that may not be assessed in traditional measures of antisocial behavior. Examples include risky sexual behavior and disordered eating (Broidy et al, 2003). Future studies that include these behaviors in addition to more traditional delinquent behavior (e.g. vandalism) may better capture manifestations of delinquent behavior in females and thus may be able to more fully speak to gender differences in the developmental relationship between symptoms of depression and conduct disorder over time.
Limitations and future directions
These results underscore the importance of examining both direct and indirect links between symptoms of depression and antisocial behavior and highlight the importance of models that attempt to unpack these intermediary processes. It is worth highlighting that direct paths between antisocial behavior and later depression were observed for males, while more indirect paths between depression and later antisocial behavior were observed for females. Such direct paths may reflect the reliance on annual assessments in the current study. It is common for large longitudinal studies to rely on annual assessments, in light of the methodological and practical challenges associated with large-scale data collection. This assessment approach may miss developmental processes that unfold over shorter intervals for males, however, and studies employing short-term longitudinal methods may be needed to unpack such processes.
One potential reason for the disparate results across this literature is the inconsistency of methods across studies. Peer functioning, for example, has been operationalized as association with deviant peers (Patternson, Dishion, &Yoerger, 2000), social competence (Bornstein, Hahn, & Haynes, 2010), and derived ratings of popularity among peers (Kiesner, 2002; van Lier & Koot, 2010). Further, academic functioning can include academic performance (Cole et al, 1997; Dishion, Veronneau, & Myers, 2010), teacher ratings of classroom behavior (Kiesner, 2002; Moilanen et al, 2010), or a combination of the two (Masten et al, 2005). Studies also vary in the length of time between assessments, with follow-ups occurring anywhere from months to multiple years following baseline assessment. This may affect the pattern of results researchers find.
It is also worth highlighting that we used a treatment sample in the current study. While this approach has also been used in similar types of studies (Dishion, Veronneau, & Myers, 2010; Murray-Close et al, 2010), it will be important for other studies to examine these developmental processes in non-treatment samples. In addition, the intent to treat (ITT) approach used in this study does not account for the amount of intervention received by each family. Alternative analytic strategies, such as complier average causal effect models, could be used in future studies to better account for treatment dosage.
This study also focused on a relatively limited age range. However, the processes that impact the relationship between symptoms of depression and antisocial behavior no doubt begin before grade 6 and extend beyond grade 9. Thus future studies should apply this analytic approach to samples including a wider age range. It may be particularly important to use samples that begin at earlier ages, as it appears that the majority of the significant findings were between the sixth and seventh grades, especially for females. It is possible that a true developmental cascade model using a wider age range would pick up these earlier effects, when more minor levels of symptoms are present. It may also be the case that different models apply to children who have early rather than late onset of behavior problems, as early onset of behavior problems has been associated with greater impairment in later functioning in males (Moffitt, Caspi, Harrington, & Milne, 2002). Having information regarding earlier symptoms would allow researchers to examine this possibility. Further, it is possible that participants in this study may have exhibited behavior problems at younger ages that have since desisted but may have influenced the other symptoms they are currently exhibiting. Following this sample further into adolescence may also be informative, as other research suggests that females may exhibit a delayed onset of behavior problems relative to males (Silverthorn & Frick, 1999).
It is also important to recognize that failures in different domains may be more or less salient depending on the developmental tasks relevant to the specific age– e.g. academic problems are perhaps more salient for school-age children than young adults, and peer rejection may be more important in adolescence (Masten et al, 2005). Further, this study looked at peer victimization, however it may also be important to examine the role that other types of peer dynamics play in the relationship between the development of internalizing and externalizing symptoms. Such dynamics include peer rejection and popularity (van Lier & Koot, 2010). In addition, peer relationships are only one type of relationship important in the lives of early adolescents. The influence of the quality of the parent-child relationship in the processes examined here will be important to study in future work. The data used in these analyses were also taken entirely from adolescent self-report. While the use of adolescent-report measures has advantages (for example, parents may be less aware of adolescent antisocial behavior, depression, or peer problems than are teens), objective measures and/or multiple informants should be used in future studies to examine the potential impact of mono-rater bias on the current pattern of results. Despite these limitations, these results highlight the importance of examining gender differences in developmental questions and intermediary processes in the links between disorders for both informing intervention design and theoretical understanding.
Acknowledgments
This research was supported by the National Institute on Drug Abuse Grant DA018374 to Elizabeth Stormshak and National Institutes of Health Grant DA018760 to Thomas Dishion. We acknowledge the contribution of the Portland Public Schools, the Project Alliance staff, and participating youth and families.
Contributor Information
Susan Klostermann, Case Western Reserve University, Department of Psychological Sciences, Psychology Program, 10900 Euclid Avenue, Cleveland, OH 44106
Arin Connell, Associate Professor, Case Western Reserve University, Department of Psychological Sciences, Psychology Program, 10900 Euclid Avenue, Cleveland, OH 44106
Beth Stormshak, Associate Vice President for Research, Professor, College of Education, Director, Child and Family Center/Prevention Science Institute, University of Oregon, Eugene, OR 97403
References
- Angold A, Costello EJ, Erkanli A. Comorbidity. Journal of Child Psychology & Psychiatry. 1999;40(1):57–87. [PubMed] [Google Scholar]
- Beyers JM, Loeber R. Untangling developmental relations between depressed mood and delinquency in male adolescents. Journal of Abnormal Child Psychology. 2003;31:247–266. doi: 10.1023/a:1023225428957. [DOI] [PubMed] [Google Scholar]
- Biederman J, Faraone S, Mick E, Lelon E. Psychiatric comorbidity among referred juveniles with major depression: Fact or artifact? Journal of the American Academy of Child & Adolescent Psychiatry. 1995;34:579–590. doi: 10.1097/00004583-199505000-00010. [DOI] [PubMed] [Google Scholar]
- Bornstein MH, Hahn C, Haynes OM. Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Development and Psychopathology. 2010;22:717–735. doi: 10.1017/S0954579410000416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broidy LM, Trembly RE, Brame B, Fergusson D, Horwood JL, Laird R, Moffitt TE, et al. Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: A six-site, cross-national study. Developmental Psychology. 2003;39:222–245. doi: 10.1037//0012-1649.39.2.222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burke JD, Loeber R, Lahey BB, Rathouz PJ. Developmental transitions among affective and behavioral disorders in adolescent boys. Journal of Child Psychology and Psychiatry. 2005;46:1200–1210. doi: 10.1111/j.1469-7610.2005.00422.x. [DOI] [PubMed] [Google Scholar]
- Capaldi D. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: I. Familial factors and general adjustment at Grade 6. Development and Psychopathology. 1991;3(3):277–300. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Capaldi D. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: II. A 2-year follow-up at Grade 8. Development and Psychopathology. 1992;4(1):125–144. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Capaldi DM, Stoolmiller M. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: III. Prediction to young-adult adjustment. Development and Psychopathology. 1999;11:59–84. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Chen X, Rubin KH, Li B. depressed mood in Chinese children: Relations with school performance and family environment. Journal of Consulting and Clinical Psychology. 1995;63(6):938–947. doi: 10.1037//0022-006x.63.6.938. [DOI] [PubMed] [Google Scholar]
- Coie JD, Dodge K, Kupersmidt J. Peer group behavior and social status. In: Asher SR, Coie JD, editors. Peer rejection in childhood. Cambridge, England: Cambridge University Press; 1990. pp. 17–59. [Google Scholar]
- Cole DA, Martin JM, Powers B, Truglio R. Modeling causal relations between academic and social competence and depression: A multitrait-multimethod longitudinal study of children. Journal of Abnormal Psychology. 1996;105:258–270. doi: 10.1037//0021-843x.105.2.258. [DOI] [PubMed] [Google Scholar]
- Cole DA, Martin JM, Powers B. A competency-based model of child depression: A longitudinal study of peer, parent, teacher, and self-evaluations. Journal of Child Psychology and Psychiatry. 1997;38:505–514. doi: 10.1111/j.1469-7610.1997.tb01537.x. [DOI] [PubMed] [Google Scholar]
- Connell AM, Dishion TJ. The contribution of peers to monthly variation in adolescent depressed mood: A short-term longitudinal study with time-varying predictors. Development and Psychopathology. 2006;18(1):139–154. doi: 10.1017/S0954579406060081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell A, Dishion T, Stormshak B. The Family Check-up and adolescent depression: An examination of treatment non-responders. Poster presented as part of organized poster symposium at the Society for Prevention Research; San Francisco, CA. 2013. May, [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell A, Stormshak B, Dishion T. Maternal depressive symptoms and early adolescent development: Mediators and moderators. Paper presented at Life History Research Society’s 2014 Biennial Meeting; Pittsburgh, PA. 2014. May, [Google Scholar]
- Connell A, Stormshak B, Dishion T. The Family Check-Up: Family prevention effects on depressive symptoms in early adolescence. Paper presented at the International Society for Research on Child and Adolescent Psychopathology; Seattle, WA. 2009. Jun, [Google Scholar]
- Curran PJ, Bollen KA. The best of both worlds: Combining autoregressive and latent curve models. In: Collins LM, Sayer AG, editors. New Methods for the Analysis of Change Decade of Behavior. Washington, DC: American Psychological Association; 2001. pp. 107–135. [Google Scholar]
- Diego MA, Field TM, Sanders CE. Academic performance, popularity, and depression predict adolescent substance use. Adolescence. 2003;38:35–42. [PubMed] [Google Scholar]
- Dishion TJ, Kavanagh K. Intervening in adolescent problem behavior: A family-centered approach. New York, NY: Guilford Press; 2003. [Google Scholar]
- Dishion TJ, Stormshak EA. Intervening in Children’s Lives: An Ecological, Family-Centered Approach to Mental Health Care. Washington, DC: American Psychological Association; 2007. [Google Scholar]
- Dishion TJ, Veronneau MH, Myers MW. Cascading peer dynamics underlying the progression from problem behavior to violence in early to late adolescence. Development and Psychopathology. 2010;22:603–619. doi: 10.1017/S0954579410000313. [DOI] [PubMed] [Google Scholar]
- Ehrensaft MK. Interpersonal relationships and sex differences in the development of conduct problems. Clinical Child and Family Psychology Review. 2005;8(1):39–63. doi: 10.1007/s10567-005-2341-y. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Wanner B, Vitaro F, Horwood LJ, Swain-Campbell N. Journal of Abnormal Child Psychology. 2003;31:605–618. doi: 10.1023/a:1026258106540. [DOI] [PubMed] [Google Scholar]
- Hawker DSJ, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry. 2000;41:441–455. [PubMed] [Google Scholar]
- Hipwell AE, Stepp S, Feng X, Burke J, Battista DR, Loeber R, Keenan K. Impact of oppositional defiant disorder dimensions on the temporal ordering of conduct problems and depression across childhood and adolescence in girls. Journal of Child Psychology and Psychiatry. 2011;52:1099–1108. doi: 10.1111/j.1469-7610.2011.02448.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keenan K, Loeber R, Green S. Conduct disorder in girls: A review of the literature. Clinical Child and Family Psychology Review. 1999;2:3–19. doi: 10.1023/a:1021811307364. [DOI] [PubMed] [Google Scholar]
- Kiesner J. Depressive symptoms in early adolescence: Their relations with classroom problem behavior and peer status. Journal of Research on Adolescence. 2002;12:463–478. [Google Scholar]
- Kochel KP, Ladd GW, Rudolph KD. Longitudinal associations among youth depressive symptoms, peer victimization, and low peer acceptance: An interpersonal process perspective. Child Development. 2012;83:637–650. doi: 10.1111/j.1467-8624.2011.01722.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kofler MJ, McCart MR, Zajac K, Ruggiero KJ, Saunders BE, Kilpatrick DG. Depression and delinquency covariation in an accelerated longitudinal sample of adolescents. Journal of Consulting and Clinical Psychology. 2011;79:458–469. doi: 10.1037/a0024108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kovacs M, Paulauskas S, Gatsonis C, Richards C. Depressive disorders in childhood: III. A longitudinal study of co-morbidity with and risk for conduct disorder. Journal of Affective Disorders. 1988;15:205–217. doi: 10.1016/0165-0327(88)90018-3. [DOI] [PubMed] [Google Scholar]
- Loeber R, Keenan K. Interaction between conduct disorder and its comorbid conditions: Effects of age and gender. Clinical Psychology Review. 1994;14:497–525. [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS, Roisman GI, Long JD, Burt KB, Obradovic J, Riley JR, Boelcke-Stennes K, Tellegen A. Developmental cascades: Linking academic achievement and externalizing and internalizing symptoms over 20 years. Developmental Psychology. 2005;41(5):733–746. doi: 10.1037/0012-1649.41.5.733. [DOI] [PubMed] [Google Scholar]
- McCarty CA, Mason WA, Kosterman R, Hawkins JD, Lengua LJ, McCauley E. Adolescent school failure predicts later depression among girls. Journal of Adolescent Health. 2008;43:180–187. doi: 10.1016/j.jadohealth.2008.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Metzler CW, Biglan A, Rusby JC, Sprague JR. Evaluation of a comprehensive behavior management program to improve school-wide positive behavior support. Education & Treatment of Children. 2001;24(4):448–479. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people for change. 2. New York: Guilford; 2002. [Google Scholar]
- Moffitt TE, Caspi A, Harrington H, Milne BJ. Males on the life-course-persistent and adolescence-limited antisocial pathways: Follow-up at age 26 years. Development and Psychopathology. 2002;14:179–207. doi: 10.1017/s0954579402001104. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A, Rutter M, Silva PA. Sex differences in antisocial behavior: Conduct disorder, delinquency, and violence in the Dunedin Longitudinal Study. New York: Cambridge University Press; 2001. [Google Scholar]
- Moilanen KL, Shaw DS, Maxwell KL. Developmental cascades: Externalizing, internalizing, and academic competence from middle childhood to early adolescence. Development and Psychopathology. 2010;22:635–653. doi: 10.1017/S0954579410000337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monahan KC, Steinberg L, Cauffman E. Affiliation with antisocial peers, susceptibility to peer influence, and antisocial behavior during the transition to adulthood. Developmental Psychology. 2009;45:1520–1530. doi: 10.1037/a0017417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray-Close D, Hoza B, Hinshaw SP, Arnold LE, Swanson J, Jensen PS, Hechtman L, Wells K. Developmental processes in peer problems of children with attention-deficit/hyperactivity disorder in The Multimodal Treatment Study of Children with ADHD: Developmental cascades and vicious cycles. Development and Psychopathology. 2010;22:785–802. doi: 10.1017/S0954579410000465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 7. Los Angeles, CA: Muthén & Muthén; 2013. [Google Scholar]
- Nelson JR, Benner GJ, Lane K, Smith BW. Academic achievement of K-12 students with emotional and behavioral disorders. Exceptional Children. 2004;71:59–73. [Google Scholar]
- Nock MK, Kazdin AE, Hiripi E, Kessler RC. Prevalence, subtypes, and correlates of DSM-IV conduct disorder in the National Comorbidity Survey Replication. Psychological Medicine. 2006;36:699–710. doi: 10.1017/S0033291706007082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR, Dishion TJ, Yoerger K. Adolescent growth in new forms of problem behavior: Macro- and micro-peer dynamics. Prevention Science. 2000;1:3–13. doi: 10.1023/a:1010019915400. [DOI] [PubMed] [Google Scholar]
- Patterson GR, Stoolmiller M. Replications of a dual failure model for boys’ depressed mood. Journal of Consulting and Clinical Psychology. 1991;59:491–498. doi: 10.1037//0022-006x.59.4.491. [DOI] [PubMed] [Google Scholar]
- Quiroga CV, Janosz M, Bisset S, Morin AJS. Early adolescent depression symptoms and school dropout: Mediating processes involving self-reported academic competence and achievement. Journal of Educational Psychology. 2013;105:552–560. [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, Boelen PA, van der Schoot M, Telch MJ. Prospective linkages between peer victimization and externalizing problems in children: a meta-analysis. Aggressive Behavior. 2011;37:215–222. doi: 10.1002/ab.20374. [DOI] [PubMed] [Google Scholar]
- Rudolph KD, Hammen C, Burge D. Interpersonal functioning and depressive symptoms in childhood: Addressing the issues of specificity and comorbidity. Journal of Abnormal Child Psychology. 1994;22:355–371. doi: 10.1007/BF02168079. [DOI] [PubMed] [Google Scholar]
- Schwartz D, Gorman AH, Duong MT, Nakamoto J. Peer relationships and academic achievement as interacting predictors of depressive symptoms during middle childhood. Journal of Abnormal Psychology. 2008;117:289–299. doi: 10.1037/0021-843X.117.2.289. [DOI] [PubMed] [Google Scholar]
- Silverthorn P, Frick PJ. Developmental pathways to antisocial behavior: The delayed-onset pathway in girls. Development and Psychopathology. 1999;11:101–126. doi: 10.1017/s0954579499001972. [DOI] [PubMed] [Google Scholar]
- Stormshak EA, Connell AM, Veronneau MH, Myers MW, Dishion TJ, Kavanagh K, Caruthers AS. An ecological approach to promoting early adolescent mental health and social adaptation: Family-centered intervention in public middle schools. Child Development. 2011;82:209–225. doi: 10.1111/j.1467-8624.2010.01551.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stormshak EA, Fosco GM, Dishion TJ. Implementing interventions with families in schools to increase youth school engagement: The Family Check-Up model. School Mental Health. 2010;2(2):82–92. doi: 10.1007/s12310-009-9025-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toro PA, Urberg KA, Heinze HJ. Antisocial behavior and affiliation with deviant peers. Journal of Clinical Child & Adolescent Psychology. 2004;33:336–346. doi: 10.1207/s15374424jccp3302_15. [DOI] [PubMed] [Google Scholar]
- Van Lier PAC, Koot HM. Developmental cascades of peer relations and symptoms of externalizing and internalizing problems from kindergarten to fourth-grade elementary school. Development and Psychopathology. 2010;22:569–582. doi: 10.1017/S0954579410000283. [DOI] [PubMed] [Google Scholar]
- Wiesner M. A longitudinal latent variable analysis of reciprocal relations between depressive symptoms and delinquency during adolescence. Journal of Abnormal Psychology. 2003;112:633–645. doi: 10.1037/0021-843X.112.4.633. [DOI] [PubMed] [Google Scholar]
- Wolff JC, Ollendick TH. The comorbidity of conduct problems and depression in childhood and adolescence. Clinical Child and Family Psychology Review. 2006;9:201–220. doi: 10.1007/s10567-006-0011-3. [DOI] [PubMed] [Google Scholar]
- Zwierzynska K, Wolke D, Lereya TS. Peer victimization in childhood and internalizing problems in adolescence: A prospective longitudinal study. Journal of Abnormal Child Psychology. 2013;41:309–323. doi: 10.1007/s10802-012-9678-8. [DOI] [PubMed] [Google Scholar]