

Abstract
Caldwell Luc surgery (CWS) is almost 120 years old now and it still enjoys an important place in ENT Surgeons armamentarium. The logic behind this surgery is to replace the diseased and scarred mucosa from maxillary sinus with new mucosa. In the initial period of this long journey the surgery gained many other important indications which also includes approach to surrounding structures which makes us to think if it’s really a radical surgery as it is used just an approach to other structure. This was a retrospective study of CWS done during period of 2002–2014 in Sri Venkateshwara ENT Institute and Bowring & Lady Harding Hospital both of these attached to Bangalore Medical College & Research Institute. In this study we have tried to analyze the indications and surgical procedure adapted and complications. Even though it has synonym of radical antrostomy the complications were minor and temporary, except for permanent tooth anesthesia and nasal vestibular stenosis. With reasonable expertise if this surgery is done for proper indication: its worth to face these complications and it’s a versatile surgery even today.
Keywords: Caldwell Luc surgery, Antrostomy, Complications
History
The faintest of description of paranasal sinuses were tracked till 16th century. It was Berenger Del Carpi, anatomist and surgeon at Bologna who described the existence of paranasal sinuses and later infections of such sinuses [1]. But the clinico-pathological aspects of maxillary sinusitis were first described by Nathaniel Highmore by whose name the sinus is still called as sinus of Highmore [2]. And so goes the treatment aspect to him. He practiced thrusting a silver bodkin through an empty tooth socket which drained the sinus. Later many other surgeons practiced lavage with similar technique. Lamorier [3] in 1743 and Desault [4] in 1798 preferred the canine fossa approach. In 1835, John Hunter [5] was one of the first proponents of the intranasal approach and in 1893 it was a surgeon from New York, George W Caldwell [6, 7] who combined canine fossa approach to gain access to the sinus and did intranasal drainage which improved surgical outcomes tremendously. He published his work in the year 1893 in the New York Medical Journal. Across the Atlantic ocean similar surgery was being done for chronic sinusitis by French surgeon called Henry Luc in 1897 [7, 8]. The only difference in this surgeon’s procedure was he did antrostomy in middle meatus in contrast to Caldwell who did inferior meatal antrostomy. But since then there were many modifications tried with little change in postoperative outcomes.
As we understood the pathophysiology of sinusitis many surgeons could do relatively conservative surgeries like FESS, Mini FESS to balloon sinuplasty for sinusitis. So at present scenario, this surgery is kept as a last resort where other surgeries have failed to adequately cure the infection. The indications lately had increased as CWS was the only approach which could provide clear and wide exposure to maxillary sinus and floor of orbit and pterygopalatine fossa. As many of these structures now can be approached with excellent illumination, visualization, with HD endoscopy sets and advanced instruments the most likely indications encountered by an otolaryngologist today will be for management of complex midfacial trauma, for removal of foreign bodies in maxillary sinus and approach to pterygopalatine fossa [9].
Materials and Methods
This is a retrospective study of CWS done during period of 2002–2014 in Sri Venkateshwara ENT Institute and Bowring & Lady Curzon hospital, both of these hospitals attached to Bangalore Medical College & Research Institute. In this study we have tried to analyze the indications and surgical procedure and complications. This is a descriptive study.
Surgical Method
Done in either general anesthesia or local anesthesia.
The Upper lip is retracted and the tissues just above the gingivolabial reflection.
Infiltrated with 1 ml 1:200 000 solution of adrenaline or mixed with 1 % xylocain in cases of local anesthesia.
The incision is placed 3 mm above the line of reflection and starting at the canine ridge runs laterally for 3.5–4 cm parallel to the teeth.
Elevation of periosteum over canine fossa till Infraorbital foramen, not to injure the nerve.
Antrum is opened at canine fossa either by gouge and hammer or cutting burr.
The eventual size of the bony opening should be approximately circular and 1.5–2 cm in diameter.
Dealing with pathology/removal of sinus mucosa.
Making nasoantral window which helps in natural way to remove packing from the antrum, drainage of postoperative collection after pack removal, aeration,
Packing the sinus cavity and nasal cavity with single long ribbon gauge soaked in Betadine ointment with free end placed anteriorly in the vestibule of nose which provides adequate hemostasis.
Suturing sublabial incision with chromic catgut with good approximation of edges.
Postoperative antibiotics were given in all cases for minimum of 5 days with analgesic.
One dose of intravenous betamethasone 8 mg was given in all patients to prevent postoperative edema of cheek.
Patient was put in head end up position and was instructed not to blow nose for 2 weeks.
Antibiotics were given for minimum of 5 days.
Pack was removed after 24–48 h followed by decongestant nasal drops for 5 days.
Saline packing was done—after pack removal in cases of nasal crusting.
Patient was asked to come for regular follow ups at weekly intervals for 15 days and at 3rd and 6th month.
Inclusion Criteria
All the patients who have undergone CWS during 2002–2014 for sinus pathology.
Patients who have undergone CWS for indications as an approach to surrounding structures.
Patients who have undergone CWS earlier.
Exclusion Criteria
Children under 17 years.
Patients who lost to follow up.
Observations and Results
Total of 53 patients were included in this study who fulfilled inclusion criteria. In that 36 were male patients and 17 were females (Fig. 1).
Fig. 1.

Graph showing sex distribution
In our study majority of patients had recurrent antrochoanal polyp for which patient would have undergone other surgeries like middle meatal antrostomy, FESS etc. numbering more than half of cases (35 cases out of 53). The next major chunk was of resistant sinusitis numbering 10 out of 53. Dental and dentigerous cyst comes to 5 and cholesteatoma of nose comes to three (Fig. 2).
Fig. 2.
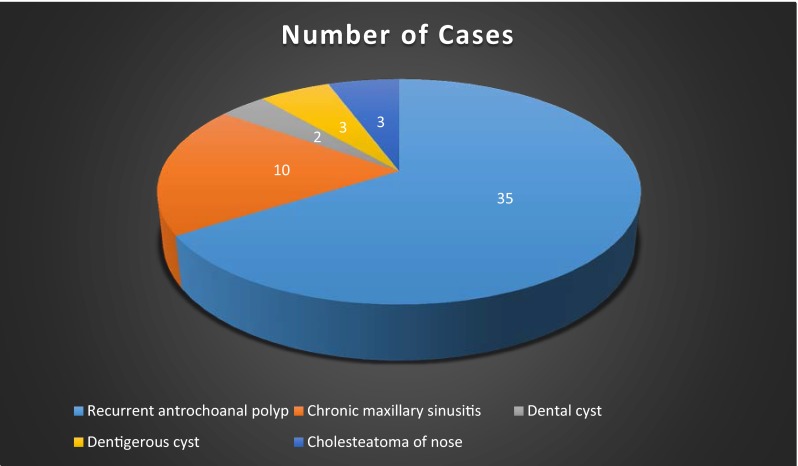
Showing the various indications for Cadwell Luc surgery in our study
Most common immediate complication in our study was facial swelling in 42 (79 %). Followed by nasal bleeding 3 (0.5 %). All patients had attended follow up visits and at 3rd month facial paresthesia was found 5 (1 %) patients and there were no fistula/and nasolacrimal duct obstruction. 3 (0.5 %) patients had anesthesia of upper tooth. No patient had discoloration of tooth. At 6th month follow up one of five patients with facial paresthesia had improvement and one had nasal vestibular stenosis. However patient did not consent for repair procedure.
Discussion
As it was said earlier CWS has seen generations of ENT surgeon’s. It was successful even in pre antibiotic era. And this surgery will continue to be the choice for few indications in future also. There are many research articles published from various authors which not just increased the list of indications but decreased the number of complications to reach this stage and now it can be considered as safer procedure.
Literature quotes many indications for this surgery/approach like chronic sinusitis with irreversible changes in sinus mucosa which would not respond to medical line of management or conservative surgeries like FESS. It was used for many dental conditions like dental and Dentigerous cysts with effective cure rates. It is also used for closure of oro antral communications which is also a potential complication of this surgery. As roof of maxillary antrum forms the floor of orbit this approach is used to repair blow out fracture of floor of orbit also. CWS is an excellent approach to vidian canal for vidian neurectomy and also used to approach maxillary artery for its ligation.
There are many research articles published which preach about the problems associated with this surgery and very radical nature of the surgery and it was found that the regenerated mucosa of antrum would not have a normal ciliary motility and function. Becker et al. [10] in his comparison of maxillary sinus specimens removed during Caldwell Luc procedures and traditional maxillary sinus antrostomies found that post CWS samples from antrum found to have necrotic bone debris compared to control group where he found relatively healthy mucosa. So ti should be kept in mind that this surgery to be used as last resort when other modality fails.
Närkiö Mäkelä [11] has compared the effectiveness of CWS v/s FESS antrostomy for recurrent sinusitis patients. And he found out that there was significantly less rates of revision surgeries in CWS group.
Penttilä et al. [12] found out that symptoms improvement and compliance was better in FESS antrostomy group. This shows that FESS antrostomy should be the first choice for treating chronic sinusitis and CWS should be a reserved strategy.
Huang and Chen [13] in his study with CWS without inferior meatal antrostomy concluded that creating sinonasal window after clearing dental origin tumors/cysts from maxillary cavity do not change surgical outcome.
Conclusion
CWS is a versatile surgery and safe with present knowledge and technique. Having other safer and effective procedures this procedure should be considered for limited cases and to be done with utmost care and enthusiasm to get best of result possible.
Contributor Information
R. K. Datta, Email: drdattaranganath@rediffmail.com
B. Viswanatha, Email: drbviswanatha@yahoo.co.in
References
- 1.Wright J. A history of laryngology and rhinology. Vol. 21, Series 2. Index Catalog of the Library of the Surgeon—General’s Office, US Army. Washington DC: Government Printing Office, 1914
- 2.Fallopius G. Abstract Anatomica, Frankfurt 1600, 367. Quoted in Jeanty JM. De l’empyeme latent de l’antra d’Higmore, Bordeaux, 1891
- 3.Lamorier L. Quoted by Mickulicz J. Sur operative Behandlung das Empyens der Highmorshohle. Archiv fu¨r Klinische Chirurgie. 1743; 34: 626–34
- 4.Desault PJ. Oeuvres chirurgicales ou expose de la doctrine et de la pratique de P.J. Desault. Vol. 1: Maladie des parties molles. Chez Meguignon, 1798; 142–53
- 5.Hunter J. Collected works, Vol. ii, edited by Palmer, London: Longman. London: Royal College of Surgeons, 1835:77
- 6.Caldwell GW. Diseases of the accessory sinuses of the nose and an improved method of treatment of suppuration of the maxillary antrum. New J Med J. 1893;58:526–528. [Google Scholar]
- 7.McBeth R. Caldwell, Luc, and their operation. Laryngoscope. 1971;81:1652–1657. doi: 10.1288/00005537-197110000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Luc H. Une nouvelle methode operatoire pur la cure radicle et l’empyeme chronique du sinus maxillazire. Archives internationals de laryngologie, d’otologie et de rhinologie. 1897; 10:273–85
- 9.Har-El G. Combined endoscopic transmaxillary-transnasal approach to the pterygoid region, lateral sphenoid sinus, and retrobulbar orbit. Ann Otol Rhinol Laryngol. 2005;114:439–442. doi: 10.1177/000348940511400605. [DOI] [PubMed] [Google Scholar]
- 10.Becker SS, Roberts DM, Beddow PA, Russell PT, Duncavage JA. Comparison of maxillary sinus specimens removed during Caldwell-Luc procedures and traditional maxillary sinus antrostomies. Ear Nose Throat J. 2011;90(6):262–266. doi: 10.1177/014556131109000607. [DOI] [PubMed] [Google Scholar]
- 11.NärkiöMäkelä M, Qvarnberg Y. Endoscopic sinus surgery or CaldwellLuc operation in the treatment of chronic and recurrent maxillary sinusitis. Acta Otolaryngol Suppl. 1997;529:17780. doi: 10.3109/00016489709124115. [DOI] [PubMed] [Google Scholar]
- 12.Penttilä MA, Rautiainen ME, Pukander JS, Karma PH. Endoscopic versus CaldwellLuc approach in chronic maxillary sinusitis: comparison of symptoms at oneyear followup. Rhinology. 1994;32(4):1615. [PubMed] [Google Scholar]
- 13.Huang YC, Chen WH. CaldwellLuc operation without inferior meatal antrostomy: a retrospective study of 50 cases. J Oral Maxillofac Surg. 2012;70(9):20804. doi: 10.1016/j.joms.2011.09.044. [DOI] [PubMed] [Google Scholar]