

Sir,
Innovations in health care and technological advancements have become an indispensable aid in the management of patients. However, few delivery rooms across the world are equipped with the state of the art infrastructure available in a fully functional NICU.
According to the ILCOR guidelines, the heart rate measurement continues to be the most effective variable used for evaluating the newborn's status and response to resuscitation.1 Despite the introduction of ECG monitoring employed in hospital units over the last five decades, the application for this technology continues to be sparse in most delivery rooms.
An inaccurate assessment of the newborn's heart rate is a major concern as it may lead to unnecessary interventions. Assessment by palpation has failed to accurately determine the heart rate while auscultation of the precordium was regarded as more reliable. However, clinical assessment of the heart rate by auscultation underestimated the actual heart rate compared with measurements done by ECG.2
The introduction of pulse oximeters with advanced processing algorithms to adjust for motion artifact and poor perfusion states led to the recommendation for pulse oximeters to be used as an adjunct in monitoring a newborn's heart rate during resuscitation. However, most studies report that ECG can assess heart rates more quickly and more reliably.3–5 Therefore, the recently revised 2015 ILCOR guidelines suggest the use of 3-lead ECG during the resuscitation of newborns (Fig. 1).1
Fig. 1.
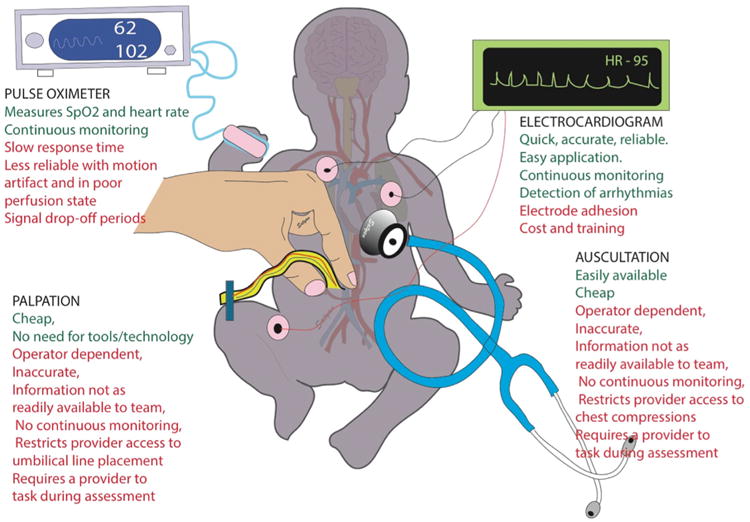
Advantages (shown in green font) and disadvantages (red font) of the currently available methods to assess the heart rate during resuscitation of the newborn infant in the delivery room. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
A very important advantage of ECG in assessing heart rate is the considerably quicker time in acquiring a heart rate as compared to a pulse oximeter. In a study of 53 term and preterm infants, the time required to acquire ECG data after sensor application is 1 (1–2) vs 12 (9–30) s, respectively.5 In another study of 30 very low birth weight newborns, the median time to acquire a reliable heart rate with ECG is reported to be 2 s (1–4), as compared to pulse oximeter that takes 24s (16–35).4 In addition, ECG electrodes can be placed quickly with reported median times of 26 (17–41)3 and 38 (34–43) s.4
The ECG's reliability and accuracy in assessing a newborn's heart rate as quickly as possible would enable health care providers to better attend to the newborn's needs. In the most severely compromised infants requiring chest compressions, ECG monitoring can reliably pick up intrinsic beats and detect return of spontaneous circulation while limiting interruption of chest compressions to auscultate the precordium.
The potential of an optimal and quick heart rate assessment of the newborn should encourage the employment of ECG, particularly in institutions that already have ECG monitoring capabilities to extend the use of this technology to the delivery room. We, therefore, welcome the new recommendation of ECG monitoring in the assessment of the newborn infant's heart rate during resuscitation in the delivery room.
Footnotes
Conflict of interest statement: The authors disclose no conflict of interest.
References
- 1.Wyllie J, Perlman JM, Kattwinkel J, et al. Part 7: Neonatal resuscitation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2015;95:e169–201. doi: 10.1016/j.resuscitation.2015.07.045. [DOI] [PubMed] [Google Scholar]
- 2.Kamlin CO, O'Donnell CP, Everest NJ, Davis PG, Morley CJ. Accuracy of clinical assessment of infant heart rate in the delivery room. Resuscitation. 2006;71:319–21. doi: 10.1016/j.resuscitation.2006.04.015. [DOI] [PubMed] [Google Scholar]
- 3.Mizumoto H, Tomotaki S, Shibata H, et al. Electrocardiogram shows reliable heart rates much earlier than pulse oximetry during neonatal resuscitation. PediatrInt. 2012;54:205–7. doi: 10.1111/j.1442-200X.2011.03506.x. [DOI] [PubMed] [Google Scholar]
- 4.Katheria A, Rich W, Finer N. Electrocardiogram provides a continuous heart rate faster than oximetry during neonatal resuscitation. Pediatrics. 2012;130:e1177–81. doi: 10.1542/peds.2012-0784. [DOI] [PubMed] [Google Scholar]
- 5.van Vonderen JJ, Hooper SB, Kroese JK, et al. Pulse oximetry measures a lower heart rate at birth compared with electrocardiography. J Pediatr. 2015;166:49–53. doi: 10.1016/j.jpeds.2014.09.015. [DOI] [PubMed] [Google Scholar]