

Abstract
Defining chronic kidney disease (CKD) is the subject of intense debate in the current nephrology literature. The debate concerns the threshold value of estimated glomerular filtration rate (eGFR) used to make the diagnosis of CKD. Current recommendations argue that a universal threshold of 60 mL/min/1.73m2 should be used. This threshold has been defended by epidemiological studies showing that the risk of mortality or end-stage renal disease increases with an eGFR below 60 mL/min/1.73m2. However, a universal threshold does not take into account the physiologic decline in GFR with ageing nor does it account for the risk of mortality and end-stage renal disease being trivial with isolated eGFR levels just below 60 mL/min/1.73m2 in older subjects and significantly increased with eGFR levels just above 60 mL/min/1.73m2 among younger patients. Overestimation of the CKD prevalence in the elderly (medicalisation of senescence) and underestimation of CKD (potentially from treatable primary nephrologic diseases) in younger patients is of primary concern. An age-calibrated definition of CKD has been proposed to distinguish age-related from disease-related changes in eGFR. For patients younger than 40 years, CKD is defined by eGFR below 75 mL/min/1.73m2. For patients with ages between 40 and 65 years, CKD is defined by 60 mL/min/1.73m2. For subjects older than 65 years without albuminuria or proteinuria, CKD is defined by eGFR below 45 mL/min/1.73m2.
Introduction: what is the controversy?
Chronic kidney disease (CKD) is often described as the “silent killer” in medicine, as this pathology is seldom symptomatic until the glomerular filtration rate (GFR) is severely decreased. Therefore, blood and urine screening during routine medical care is of key importance. The two most useful biomarkers to assess the kidney health are GFR and albuminuria (or proteinuria) assessment.1 Other more specific tests exist for characterising CKD but are beyond the scope of this review article. Estimation of GFR (eGFR) is based on renally-filtered serological biomarkers, most commonly serum creatinine levels (SCr)-based equations.2 The value of SCr is dependent on GFR but also on muscular mass, tubular secretion of creatinine and to some extent dietary consumption of lean, cooked meat. Moreover, the relationship between SCr and GFR is a reciprocal function. Estimation of GFR by creatinine-based equations includes other variables like gender, ethnicity and, importantly for our discussion, age.3,4 There have been multiple creatinine-based equations developed3,5,6 as well as methods of albuminuria or proteinuria testing developed.7–10 To simplify the discussion, we will consider the recommendations of the widely disseminated Kidney Disease Improving Global Outcome (KDIGO) guidelines.1 They recommend the Chronic Kidney Disease Epidemiology (CKD-EPI) equation and the urinary albumin (or protein)-creatinine ratio (UACR) on a random spot urine sample, preferably obtained in the morning.
Based on these two parameters, the KDIGO have defined classification or categorisation for CKD (Table 1).1 Basically, the subject or the patient can be classified in 6 different categories according to the eGFR level: from category 1 when the eGFR is over 90 mL/min/1.73m2 to category 5 when eGFR is below 15 mL/min/1.73m2, the category 3 being divided into 3A (eGFR between 45 and 59 mL/min/1.73m2) and 3B (eGFR between 30 and 44 mL/min/1.73m2).1,11 It is fundamental to understand that the label of “CKD” will be attributed to every patient with an eGFR below 60 mL/min/1.73m2, even in the absence of abnormal albuminuria, whereas the diagnosis will be considered in patients with eGFR over 60 mL/min/1.73m2, only if they have one additional evidence of kidney injury, most of the time, abnormal UACR. Also of importance, eGFR below 60 mL/min/1.73m2 must persist for at least 3 months to be considered CKD.1 Absent from the KDIGO definition of CKD is any consideration for the age-related decline in GFR. Many physiological functions naturally decrease with ageing.12–19 Failure to account for this in the definition of CKD has led to many elderly subjects being misclassified as having CKD, even when their modest reduction in eGFR is the normal expected change in physiology with ageing.12,13,15,18,20–25 We proposed an alternative classification in subjects older than 65 years where category 3A will not be considered as CKD in the absence of any other sign of kidney damage (like an abnormal UACR).23 Moreover, we also proposed the GFR threshold of CKD for patients younger than 40 years be raised at 75 mL/min/1.73m2.26 Thus, the definition of CKD by eGFR thresholds alone should be age-calibrated in order to identify pathological reductions in GFR that do not simply occur with normal ageing.
Table 1.
GFR categories according to the KDIGO.1 Category 1 and 2 are CKD only if additional kidney injury. Our proposal is that category 3A is no longer considered as CKD in subjects older than 65y and without any other kidney damage (like albuminuria).23
| Categories | eGFR (mL/min/1.73m2) |
|---|---|
| 1 | >90 |
| 2 | 60–89 |
| 3A | 45–59 |
| 3B | 30–44 |
| 4 | 15–29 |
| 5 | <15 |
What is the definition of normality in diagnostic medicine?
While perhaps thought to be easily determined, clinical chemists are well aware that determining “normal reference ranges” can be quite challenging.27,28 Establishing normal reference values is however of much importance as they will often be used to define a disease status. Basically, there are two main methods to define normality in medicine:12 1) the classical method measures the parameter in a presumably healthy, normal, representative population and calculate a range value such as the 2.5th to 97.5th percentiles; 2) the risk-based method considers the risk of outcomes associated with the thresholds. The first method is applied for most parameters in clinical chemistry. For example, the normal values of a parameter like parathyroid hormone will be very different if global healthy subjects are considered (like blood donors) or if the definition of normality is more restrictive and requires subjects with normal eGFR, calcium and vitamin D levels.29 An example of the risk-based method is the serum cholesterol concentration for which clinically relevant thresholds are determined according to risk of cardiovascular events as well as established clinical benefit with treatment to these thresholds.30 Perhaps ideally, both methods would give more or less the same reference limits of “normal” GFR.
Normal GFR range: the classical method
Normal GFR values observed in young healthy adult populations are approximately 100–110 mL/min/1.73m2, even if results can vary slightly depending on the method used to measure GFR (mGFR) (e.g. with reference methods using inulin, iothalamate, 51Cr-EDTA or iohexol)12,17,18 or estimated GFR.31,32 It is obvious from these studies involving healthy populations that GFR decreases with ageing. This decrease in GFR is confirmed either with mGFR (including living kidney donors) 12,17,18 or eGFR (including healthy general population).31,32 This ageing process is illustrated in Figure 1. From these studies, it can be concluded that a significant part of the healthy population older than 65 years of age have a GFR (mGFR or eGFR) below 60 mL/min/1.73m2. These results are clear and strong arguments for the necessity of an age-calibrated CKD categorisation.
Figure 1.
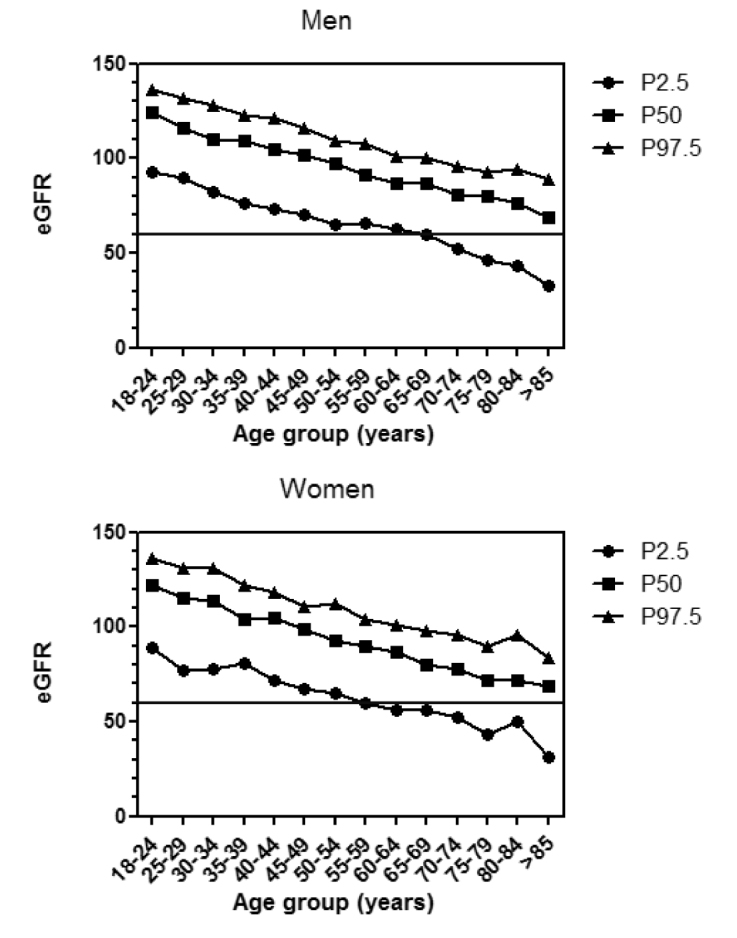
Percentile (P) values (97.5th, 50th and 2.5th) for estimated GFR (eGFR; in mL/min/1.73m2) by the CKD-EPI equation for healthy community living (Caucasian) adult Males and Females according to age between 18 and 85+ years (adapted with permission from van den Brand et al, 201132) . For comparison, the KDIGO threshold for defining CKD is given as a bold horizontal line (60 mL/min/1.73m2). Note the substantial numbers of individuals >60 years of age in the 2.5th to approximately the 40th percentile of eGFR that fall below the 60mL/min/1.73m2 threshold.
Normal GFR range: the prognostic method
The unique threshold of 60 mL/min/1.73m2 for CKD definition by the KDIGO is justified by a risk based approach.1 The arguments mainly come from the CKD-EPI prognosis consortium epidemiologic studies.33–36 These investigators have collected data from several large cohorts of patients worldwide. The sample sizes (over 1 million subjects) are very impressive but the methodology used to determine eGFR is more questionable. Among other methodological criticisms, we underline the absence of IDMS (isotope dilution mass spectrometry) traceable standardised creatinine assay in several cohorts,37 and the fact that these studies lack confirmation of decreased eGFR for at least 3 months.38 A recent study with a follow-up of 25 years in 3888 Icelandic people showed that the risk of CKD 20 years hence for a woman who is currently aged 45 years, will decrease from 16.8 to 8.6%, if CKD is changed from one eGFR value below 60 mL/min/1.73m2 to two consecutive values below 60 mL/min/1.73m2 over 3 months.39 Lack of confirmation of eGFR in epidemiological “one-off” studies leads to a large number of “false-positive” results. Studies by the CKD-EPI prognosis consortium also demonstrate a significant higher risk of death when eGFR is below 60 mL/min/1.73m2. Further, the risk of mortality associated with an eGFR below 60 mL/min/1.73m2 remains statistically significant at any age, albeit the relative risk was substantially attenuated in older adults.34
Is the debate on age-calibration of thresholds of eGFR for defining CKD relevant?
Before going further into the details of the debate on the wisdom of an age-calibrated CKD definition, it seems important to know if the changes proposed are relevant, and not purely semantic. In other words, it should be shown that an age-calibration proposal has an impact on the epidemiology of CKD in the general population. A proposal that subjects classified in stage 3A without UACR do not have CKD would greatly impact the prevalence of CKD.23 In Figure 2, one can observe the prevalence of CKD in the United States according to the KDIGO definition based on eGFR and UACR. The global prevalence is as high as 11.5%. If we focus only on the subset of patients considered to have CKD by eGFR below 60 mL/min/1.73m2 but without albuminuria, the prevalence is 4.8%. Also, the prevalence of subjects classified in CKD category 3A and without albuminuria (CKD 3A1), is 3.6%.1 This CKD category 3A1 is clearly the most important from an epidemiological point of view and corresponds to millions of subjects in the US. A study in Italy confirmed that CKD 3A is the most important contributor to the CKD epidemiology.40,41 Moreover, Figure 3 illustrates that the proportion of CKD diagnosis based on “eGFR only” increases with ageing.42 In other words, in young patients, the vast majority of CKD patients will have increased UACR and “normal” eGFR (at least according to the KDIGO criteria) whereas among older subjects, most will be labelled as CKD because of an eGFR just below 60 mL/min/1.73m2, but with a normal UACR. Clearly, the proposal that older subjects classified in CKD 3A1 do not actually have CKD is very relevant to the prevalence of CKD. In particular, the alarmingly high prevalence of CKD in the elderly (as high as 50%) with the current KDIGO based definition will be greatly decreased with adoption of an age-calibrated system.21,39,43,44
Figure 2.
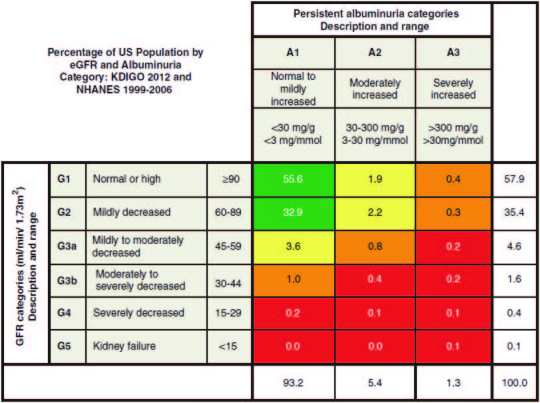
Prevalence of CKD in USA based on ACR and eGFR with the KDIGO classification system. Reprinted with permission from KDIGO.1
Figure 3.
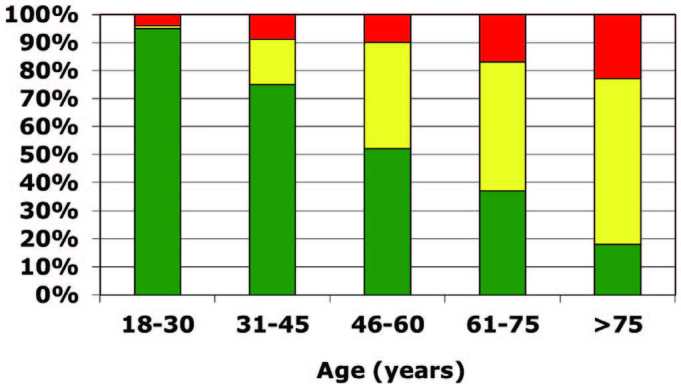
Proportion of CKD based on eGFR (yellow), ACR (green) or both (red) in different age categories (adapted from reference 42).
Is the definition of normality based on risk prediction misleading and potentially confusing?
Use of the prognostic (risk-based) method for CKD definition may be defendable with albuminuria,8,11 but such a strategy is much more questionable for eGFR. The reasons are several. Firstly, there exists a large disagreement concerning the level of eGFR associated with increased mortality, i.e. 60 mL/min/1.73m2 and eGFR actually observed in healthy populations.12,22 For example, in the healthy population described by van den Brand et al in the Netherlands, low normal eGFR value (defined as the 5th percentile) is 94 and 85 mL/min/1.73m2 at 25–29 years, 67 and 70 mL/min/1.73m2 at 50–54 years and 44 and 51 mL/min/1.73m2 at 70–74 years, for men and women respectively.32 Secondly, the prognosis-based threshold could be different according to the chronicity of the reduced eGFR.22 For example, an earlier study to suggest that increased all-cause mortality risk was independently associated with decreased eGFR was published in 2004 by Go et al. The authors showed that patients with eGFR of 45–59 mL/min/1.73m2 had a higher risk of all-cause mortality compared to an eGFR of 60ml/min/1.73m2 or greater. However, this increased risk disappeared completely when a subgroup of subjects with repeated measurement of eGFR was considered.45 Thirdly, the prognostic approach could lead to different CKD definitions if other GFR biomarkers, like serum cystatin C, were used to estimate GFR. Indeed, the threshold for worse prognosis would move the diagnosis of CKD from 60 to 80 mL/min/1.73m2 with cystatin C-based equation,22,46 even if we question if cystatin C-based equations really give better estimates of GFR,47 and if better association with mortality is not due to non-GFR determinants of cystatin C, such as obesity or inflammation.48 Finally, age, a strong predictor of mortality, is also an important variable in all eGFR estimating equations and could thus inflate all these associations.19,22,49
Is the risk of mortality associated with GFR really the same with ageing?
The concept that a unique threshold of 60 mL/min/1.73m2 is associated with risk of mortality whatever the age is also questionable. A careful study of findings by the CKD-EPI consortium is helpful.34 Firstly, contrary to the interpretations by the authors, these data support an age-calibration to CKD classification for the purposes of mortality risk. Secondly, other studies with discordant results compared to those of this study34 support the argument for an age-calibrated definition of CKD based on a mortality risk formulation (see below “Data from other CKD cohorts”).
Data from the CKD-EPI prognosis consortium
In the first CKD-EPI prognosis consortium study, not age-calibrated, the reference value of eGFR used for the hazard ratio (HR) calculation was 95 mL/min/1.73m2.36 In other words, the significant higher risk of eGFR below 60 mL/min/1.73m2 is calculated in comparison with an eGFR of 95 mL/min/1.73m2. This value makes sense as it is comparable to normal eGFR values observed in a young adult healthy population. In 2012, the same consortium looked again at the risk of mortality across categories of age.34 However, the reference value of eGFR for risk calculations was 80 mL/min/1.73m2, not 95 mL/min/1.73m2. This was done because there were not enough older individuals with higher eGFR to use as a reference group. This implicitly accepts that: 1) that the “normal” GFR decreases with ageing, and 2) the eGFR reference group for HR calculations can change according to age. However, one can easily recalculate the HR with different reference groups. Indeed, it seems fully logical to choose as reference group, the eGFR range which is actually associated with the lowest risk (Figure 4). Considering this strategy, one can easily conclude that:1) with ageing, the eGFR range of the reference group decreases, which is expected regarding the natural decline of GFR with ageing; 2) in subjects older than 65 years, CKD category 3A1 (eGFR of 45 to 59 mL/min/1.73m2) is associated with a trivial risk of mortality, whereas eGFR below 75 mL/min/1.73m2 is associated with a notably increased mortality in the youngest adult age group.19 Thus, an age-calibrated reference group applied to published data34 supports an age-dependent definition of CKD if based on mortality risk.
Figure 4.
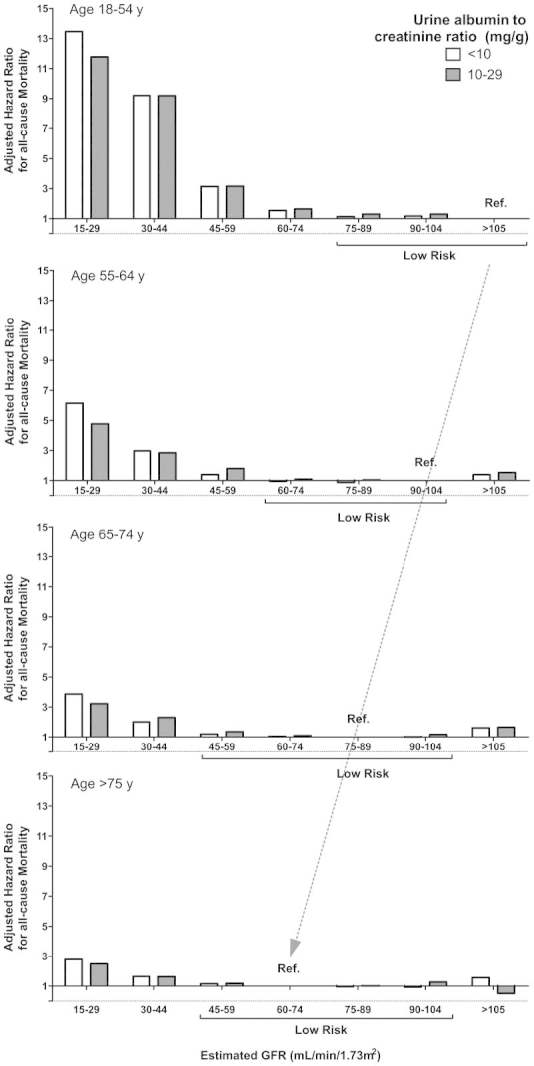
HR for mortality when the reference group19 is the one with the lowest risk. eGFR ranges into the brackets (low risk) are not significantly different from the reference group.
Data from other CKD cohorts
Besides the CKD-EPI prognosis consortium, other epidemiological data suggested that risk of mortality in elderly with eGFR just below 60 mL/min/1.73m2 could be even more trivial or non-existent. Roderick et al analysed data from a UK cohort of people 75 years and older with a median follow-up of 7.3 years. They demonstrated that the mortality risk was significantly higher only when eGFR was below 45 mL/min/1.73m2, but not if eGFR was 45–59 mL/min/1.73m2.50 In US, O’Hare analysed a large database of the Veteran Affairs (n=2,583,911) and showed that eGFR predicted the risk of mortality in the eGFR range of 50–59 mL/min/1.73m2, only in patients younger than 65 years.51 Data from the REGARDS study (for “REasons for Geographic and Racial Differences in Stroke”) confirmed that patients older than 70 years with an eGFR between 45 and 59 mL/min/1.73m2 have no increased significant risk of mortality if the UACR was normal.52 In France, the Three-City Study confirmed that eGFR was associated with mortality but the threshold was near to 45 mL/min/1.73m2 in this cohort with a mean age of 74 years.53 Comparable results are observed in an Italian population with mean age of 71 years where CKD category 3B but not 3A was associated with higher mortality on a median follow-up of 7.2 years.41 A large Canadian database (n=949,119) confirmed that life expectancy was similar in the elderly if category CKD 3A or category CKD 1–2 was considered.54 In a very recent study from Sweden, authors followed eGFR in 363 elderly women for 10 years between ages 75 and 85 years. They also found that category CKD 3B, but not 3A, was associated with mortality in 1011 women considered at baseline.55 This last study must however be interpreted carefully as no UACR measurements were available and a lack of statistical power is possible. The absence of UACR measurements is unfortunately a frequent limitation of several epidemiological studies on this topic.39,55–59 Many other epidemiological reports utilising large cohorts have included values for both eGFR and UACR, but the subjects with CKD category 3A without abnormal UACR have not commonly been specifically examined.60,61
What about the risk of end stage renal disease (ESRD)?
Many studies have shown that the risk of ESRD increases with lower eGFR, even well above the 60 mL/min/1.73m2 threshold. There are also several reasons why an age-calibrated approach is logical with eGFR thresholds for purposes of ESRD risk. First, with ageing, there is an important competing risk between mortality and ESRD. Indeed, with ageing, the risk of dying increases and exceeds the risk of ESRD.51,62,63 Notably, we can only say these elderly patients with category 3A CKD (eGFR 45 to 59 mL/min/1.73m2) die with CKD, as evidence that modest age-related reduction in GFR plays a causal role in mortality lacks any good evidence. Second, risk models used for predicting ESRD show that older age is associated with a lower risk of ESRD compared to a younger patient with the same eGFR.64 Indeed, the risk of ESRD in a 75 year old male with an eGFR of 50 mL/min/1.72 m2, no albuminuria, and otherwise unremarkable biochemistry is only 0.2% at 5 years. Thus, it is difficult to justify a label of CKD based on ESRD risk for elderly patients with category 3A CKD without albuminuria.
The “below 60 mL/min/1.73m2” threshold leads to under-diagnosis of CKD in young adults
We have focused our critique of CKD definition based on eGFR below 60 mL/min/1.73m2 to the elderly because these people represent the majority of the so-called “CKD epidemic” and are misdiagnosed with a disease that is simply normal ageing. Even considering true CKD in elderly people, i.e. category CKD 3B or higher and/or positive ACR, the vast majority of CKD in elderly is related to hypertension and/or diabetes.65 Primary nephrologic diseases, including glomerulonephritis, can be diagnosed without even needing eGFR in young patients even if their prevalence is very low.66 Such a diagnosis is of prime importance as specific effective therapies are available for glomerulonephritis. Of course, albuminuria and proteinuria measurements are a key tool for diagnosing such diseases. But regarding the eGFR criteria, the threshold of 60 mL/min/1.73m2 can be considered as much too low for young people, where a normal GFR is closer to 100–110 mL/min/1.73m2. Strictly speaking, these young patients could lose many nephrons, seeing their GFR value decreasing near to half, before being categorised as CKD.26 In summary, we consider that the current CKD classification overestimates the prevalence of CKD in older patients with very frequent but secondary (“secondary” meaning that another disease such as hypertension or diabetes precedes the CKD) nephrologic diseases but underestimates the prevalence of CKD in younger patients with rare but primary nephrologic diseases that are potentially treatable.
The gold standard tool for CKD classification
Because the definition of CKD based on mortality risk alone lacks evidentiary support, one must return to the classical method to define normality and study normal healthy populations to define reference limits for GFR. The main issue with GFR is the physiological decline of GFR with ageing. The best scientific tool to define the lower reference limit would be the use of percentiles such as the 5th or 2.5th percentile (Figure 1).21,67 Such an approach would avoid both false negative (in young people) and false positive (in elderly individuals) in the diagnosis of CKD. Such data are available in the literature for eGFR both in Caucasians and Asians.31,32,67,68 For mGFR, several publications are available in all ethnicities though we need more data for subjects older than 70 years.17,18,69 Percentiles of values for eGFR according to age (see Figure 1) to create entirely new age-calibrated eGFR thresholds for all categories of CKD 1 to 5 are thus attractive, but perhaps too complicated and challenging to implement in view of the worldwide acceptance of the current categorisation and its laboratory reporting. A simpler approach would be to use age-calibrated eGFR thresholds for defining CKD rather than for all categories of CKD. If a laboratory is capable of calculating eGFR, then it should be capable of calculating the eGFR threshold for that age (by simply filling in the 95th or 97.5th percentile for serum creatinine) and comparing both values. This change would however call upon worldwide laboratory implementation and reporting. Moreover, the choice of the most useful lowest percentile (5th, 2.5th or 3th) still needs to be defined. Our proposal to consider category CKD 3A1 (without any kidney damage) as non-CKD for subjects older than 65 years and an eGFR below 75 mL/min/1.73m2 as CKD in patients younger than 40 years seems a good compromise that would be simpler.23,26
Are these proposals nihilist and arbitrary?
The age-calibrated categorisation for identification of legitimate CKD is not unique in medicine. For example, pulmonologists recognise organ senescence in their specialty and its impact on lung function.70 The forced expiratory volume in 1 second (FEV1) is the functional equivalent of GFR for the lung and is interpreted with age-specific reference ranges to account for its gradual decline with ageing. An older individual with an isolated age-related reduction of FEV1 is not labeled as suffering from chronic lung disease. In addition, the latest iteration of the Joint National Commission on Hypertension (JNC-8) also recognises the need for age-stratification of thresholds of blood pressure when making treatment decisions.71 By a same logical reasoning, a lower eGFR (or mGFR) in older subjects need not be ascribed exclusively to a “disease”, but can be regarded as within the spectrum of physiological ageing and its associated anatomical and functional consequences.13–15,19
Three main arguments are frequently put forward against this age-calibrated categorisation for CKD. Firstly, the proposal does not fully recognise the risk inherent to progressively declining GFR and thereby may discourage future research in the field of nephrology, especially in geriatric nephrology.72 Secondly, the proposal does not take into account the potential risk both of acute kidney injury and/or potential toxicity due to the lack of drug dosage adjustment of water-soluble therapies in CKD.73 Thirdly, the new thresholds for young and old people are arbitrary and may lead to a “birthday” paradox where diagnoses would change in individuals based on an older age alone even in the presence of unchanging eGFR.
Regarding the first argument, we have discussed the weak and inconsistent evidence linking isolated eGFR just below 60 mL/min/1.73m2 to an increased risk of mortality in the elderly. Even regarding “true” CKD among older patients, it is clear that up to now, the main therapy to fight against CKD progression is to treat the underlying cause/risk factors for CKD, namely hypertension and/or diabetes.1 The lack of any specific nephrologic therapies to slow down CKD progression is however not an argument per se as it is possible such therapies may be developed in the future. However, innovative therapies must be studied and tested in true CKD patients where the risk is high enough to observe a meaningful improvement from new therapies. This point can be illustrated ad absurdum: renin-angiotensin system (RAS) inhibitors are without doubt the most effective therapies in nephrology to prevent ESRD.74 However, a recent simulation study with real-life data demonstrated that therapies with RAS inhibition would be considered as totally ineffective if studies were performed in elderly subjects with category 3A CKD and no albuminuria!63
The second argument considers the possibility that subjects at category CKD 3A1 have an increased risk of developing an adverse event when prescribed standard doses of water-soluble, potentially toxic agents. But, there are very few, if any, nephrotoxic drugs for which a dose adjustment is already recommended at this level of eGFR, 45–59 mL/min/1.73m2.11 Moreover, well-designed prospective studies must be performed to validate the hypothesis that such labelling in older subjects with an eGFR of 45–59 ml/min and no abnormal proteinuria are at greater risk of adverse events from pharmacological agents than those of similar age with an eGFR over 60 mL/min/1.73m2.
The third argument considers the proposed threshold of less than 45 mL/min/1.73m2 in the ageing subjects and less than 75 mL/min/1.73m2 in the young subject as being as arbitrary as the 60 mL/min/1.73m2 threshold. However these thresholds account for the irrefutable decline in GFR with age. These thresholds correspond to a clinically significant increase in mortality risk (Figure 4). Finally, these thresholds are obtained from the serum creatinine distribution of healthy subjects in combination with the most appropriate eGFR calculation formulas,28,75 CKD-EPI4 and BIS (for “Berlin Initiative Study”).76 It is known that the distribution of serum creatinine for healthy Caucasians is centred at 0.90 umol/L, with 97.5th percentile of 1.20 mg/dL (males) and 0.93 umol/L (females).28,75 Assuming a Gaussian distribution and to avoid that 2.5% is considered ‘abnormal’; the normal range may extend to 1.35 mg/dL for males and 1.05 mg/dL for females, corresponding to the 99.9th percentile. By incorporating this upper reference limit (99.9th percentile) for serum creatinine into the CKD-EPI formula, most suited for that level of GFR, we have:
The latter formula could be used as an age-dependent cut-off formula. If age is between 65 and 100 years, then this age-dependent cut-off would extend from 55 ml/min/1.73m2 at 65 years to 43 ml/min/1.73m2 at 100 years, with a mean of 49 ml/min/1.73m2 for the over 65. A similar approach applied to the BIS1 eGFR equation, most suitable for the older age-group,76 would give a mean for this age group (>65years) of 45 ml/min/1.73m2, the precise cut-off we are advocating to define CKD in the over 65 years group. The same reasoning is applicable in young subjects and justifies the choice of 75 mL/min/1.73m2.26
Conclusions
Diagnosing and labelling the elderly as having CKD by the KDIGO definition is not free of unwanted adverse consequences. A diagnosis of CKD can be a substantial source of anxiety and stress in the elderly. Moreover, such erroneous diagnostic leads to unnecessary referral to nephrologists, and potential unnecessary expensive laboratory testing and/or imaging. Acquiring such a label of CKD might also interfere with obtaining health and life insurance. Finally, such “over-diagnosing” also has impact on potential screening programs, and probably explains, at least in part, why population-based CKD screening is actually not very useful and not generally recommended.65,77 Why has a non-age-calibrated classification system been so widely (and uncritically in our view) been adopted? In some countries, reimbursement policies favour the identification of CKD, particularly at earlier stages. Finally, the widespread application of risk-based CKD definition to individuals is an indication of how nephrology is moving away from personalised, pathophysiological based diagnosis and towards population, epidemiological based “one size fits all” medicine.
In this opinion paper, arguments have been made that support a move from a CKD definition based on fixed eGFR threshold “below 60 mL/min/1.73m2” to an age-calibrated one. These arguments have received positive feedback from clinicians. In addition mass media have questioned the current definition, based on some of these arguments.78 However, to be fair, it must be stated that this call for an age-calibrated definition of CKD has still not convinced the leaders of the KDIGO.73 The question remains open.
Footnotes
Competing Interests: None declared.
References
- 1.KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3:1–150. doi: 10.1038/ki.2013.243. [DOI] [PubMed] [Google Scholar]
- 2.Perrone RD, Madias NE, Levey AS. Serum creatinine as an index of renal function: new insights into old concepts. Clin Chem. 1992;38:1933–53. [PubMed] [Google Scholar]
- 3.Delanaye P, Mariat C. The applicability of eGFR equations to different populations. Nat Rev Nephrol. 2013;9:513–22. doi: 10.1038/nrneph.2013.143. [DOI] [PubMed] [Google Scholar]
- 4.Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, III, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12. doi: 10.7326/0003-4819-150-9-200905050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Delanaye P, Pottel H, Botev R, Inker LA, Levey AS. Con: Should we abandon the use of the MDRD equation in favour of the CKD-EPI equation? Nephrol Dial Transplant. 2013;28:1396–403. doi: 10.1093/ndt/gft006. [DOI] [PubMed] [Google Scholar]
- 6.Rule AD, Glassock RJ. GFR estimating equations: getting closer to the truth? Clin J Am Soc Nephrol. 2013;8:1414–20. doi: 10.2215/CJN.01240213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lambers Heerspink HJ, Gansevoort RT, Brenner BM, Cooper ME, Parving HH, Shahinfar S, et al. Comparison of different measures of urinary protein excretion for prediction of renal events. J Am Soc Nephrol. 2010;21:1355–60. doi: 10.1681/ASN.2010010063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lambers Heerspink HJ, Kröpelin TF, Hoekman J, de Zeeuw D. Drug-induced reduction in albuminuria is associated with subsequent renoprotection: a meta-analysis. J Am Soc Nephrol. 2015;26:2055–64. doi: 10.1681/ASN.2014070688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Naresh CN, Hayen A, Weening A, Craig JC, Chadban SJ. Day-to-day variability in spot urine albumin-creatinine ratio. Am J Kidney Dis. 2013;62:1095–101. doi: 10.1053/j.ajkd.2013.06.016. [DOI] [PubMed] [Google Scholar]
- 10.Fotheringham J, Campbell MJ, Fogarty DG, El Nahas M, Ellam T. Estimated albumin excretion rate versus urine albumin-creatinine ratio for the estimation of measured albumin excretion rate: derivation and validation of an estimated albumin excretion rate equation. Am J Kidney Dis. 2014;63:405–14. doi: 10.1053/j.ajkd.2013.08.009. [DOI] [PubMed] [Google Scholar]
- 11.Gansevoort RT, de Jong PE. Challenges for the present CKD classification system. Curr Opin Nephrol Hypertens. 2010;19:308–14. doi: 10.1097/MNH.0b013e328337bbbe. [DOI] [PubMed] [Google Scholar]
- 12.Delanaye P, Schaeffner E, Ebert N, Cavalier E, Mariat C, Krzesinski JM, et al. Normal reference values for glomerular filtration rate: what do we really know? Nephrol Dial Transplant. 2012;27:2664–72. doi: 10.1093/ndt/gfs265. [DOI] [PubMed] [Google Scholar]
- 13.Glassock RJ, Rule AD. The implications of anatomical and functional changes of the ageing kidney: with an emphasis on the glomeruli. Kidney Int. 2012;82:270–7. doi: 10.1038/ki.2012.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rule AD, Amer H, Cornell LD, Taler SJ, Cosio FG, Kremers WK, et al. The association between age and nephrosclerosis on renal biopsy among healthy adults. Ann Intern Med. 2010;152:561–7. doi: 10.1059/0003-4819-152-9-201005040-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rule AD, Cornell LD, Poggio ED. Senile nephrosclerosis--does it explain the decline in glomerular filtration rate with ageing? Nephron Physiol. 2011;119(Suppl 1):6–11. doi: 10.1159/000328012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Davies DF, Shock NW. Age changes in glomerular filtration rate, effective renal plasma flow, and tubular excretory capacity in adult males. J Clin Invest. 1950;29:496–507. doi: 10.1172/JCI102286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Poggio ED, Rule AD, Tanchanco R, Arrigain S, Butler RS, Srinivas T, et al. Demographic and clinical characteristics associated with glomerular filtration rates in living kidney donors. Kidney Int. 2009;75:1079–87. doi: 10.1038/ki.2009.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Blake GM, Sibley-Allen C, Hilton R, Burnapp L, Moghul MR, Goldsmith D. Glomerular filtration rate in prospective living kidney donors. Int Urol Nephrol. 2013;45:1445–52. doi: 10.1007/s11255-013-0408-0. [DOI] [PubMed] [Google Scholar]
- 19.Denic A, Glassock RJ, Rule AD. Structural and functional changes with the ageing kidney. Adv Chronic Kidney Dis. 2016;23:19–28. doi: 10.1053/j.ackd.2015.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Delanaye P, Cavalier E. Staging chronic kidney disease and estimating glomerular filtration rate: an opinion paper about the new international recommendations. Clin Chem Lab Med. 2013;51:1911–7. doi: 10.1515/cclm-2013-0223. [DOI] [PubMed] [Google Scholar]
- 21.Delanaye P, Glassock RJ. Lifetime risk of CKD: what does it really mean? Clin J Am Soc Nephrol. 2015;10:1504–6. doi: 10.2215/CJN.07860715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Delanaye P, Glassock RJ. Glomerular filtration rate and ageing: another longitudinal study--a long time coming! Nephron. 2015;131:1–4. doi: 10.1159/000439147. [DOI] [PubMed] [Google Scholar]
- 23.Glassock RJ, Delanaye P, El Nahas M. An age-calibrated classification of chronic kidney disease. JAMA. 2015;314:559–60. doi: 10.1001/jama.2015.6731. [DOI] [PubMed] [Google Scholar]
- 24.Glassock RJ, Winearls C. An epidemic of chronic kidney disease: fact or fiction? Nephrol Dial Transplant. 2008;23:1117–21. doi: 10.1093/ndt/gfn086. [DOI] [PubMed] [Google Scholar]
- 25.Glassock RJ. Con: Thresholds to define chronic kidney disease should not be age dependent. Nephrol Dial Transplant. 2014;29:774–9. doi: 10.1093/ndt/gft306. [DOI] [PubMed] [Google Scholar]
- 26.Pottel H, Hoste L, Delanaye P. Abnormal glomerular filtration rate in children, adolescents and young adults starts below 75 mL/min/1.73 m(2) Pediatr Nephrol. 2015;30:821–8. doi: 10.1007/s00467-014-3002-5. [DOI] [PubMed] [Google Scholar]
- 27.Cavalier E, Delanaye P. Defining a “reference population”: no easy task. J Bone Miner Res. 2009;24:1638. doi: 10.1359/jbmr.090322. [DOI] [PubMed] [Google Scholar]
- 28.Ceriotti F, Boyd JC, Klein G, Henny J, Queraltó J, Kairisto V, et al. Reference intervals for serum creatinine concentrations: assessment of available data for global application. Clin Chem. 2008;54:559–66. doi: 10.1373/clinchem.2007.099648. [DOI] [PubMed] [Google Scholar]
- 29.Cavalier E, Delanaye P, Vranken L, Bekaert AC, Carlisi A, Chapelle JP, et al. Interpretation of serum PTH concentrations with different kits in dialysis patients according to the KDIGO guidelines: importance of the reference (normal) values. Nephrol Dial Transplant. 2012;27:1950–6. doi: 10.1093/ndt/gfr535. [DOI] [PubMed] [Google Scholar]
- 30.Stroes E. Statins and LDL-cholesterol lowering: an overview. Curr Med Res Opin. 2005;21(Suppl 6):S9–16. doi: 10.1185/030079905X59102. [DOI] [PubMed] [Google Scholar]
- 31.Baba M, Shimbo T, Horio M, Ando M, Yasuda Y, Komatsu Y, et al. Longitudinal study of the decline in renal function in healthy subjects. PLoS One. 2015;10:e0129036. doi: 10.1371/journal.pone.0129036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.van den Brand JA, van Boekel GA, Willems HL, Kiemeney LA, den Heijer M, Wetzels JF. Introduction of the CKD-EPI equation to estimate glomerular filtration rate in a Caucasian population. Nephrol Dial Transplant. 2011;26:3176–81. doi: 10.1093/ndt/gfr003. [DOI] [PubMed] [Google Scholar]
- 33.Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJ, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet. 2012;380:1662–73. doi: 10.1016/S0140-6736(12)61350-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, et al. Age and association of kidney measures with mortality and end-stage renal disease. JAMA. 2012;308:2349–60. doi: 10.1001/jama.2012.16817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mahmoodi BK, Matsushita K, Woodward M, Blankestijn PJ, Cirillo M, Ohkubo T, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: a meta-analysis. Lancet. 2012;380:1649–61. doi: 10.1016/S0140-6736(12)61272-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375:2073–81. doi: 10.1016/S0140-6736(10)60674-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Coresh J, Eknoyan G, Levey AS. Estimating the prevalence of low glomerular filtration rate requires attention to the creatinine assay calibration. J Am Soc Nephrol. 2002;13:2811–2. doi: 10.1097/01.asn.0000037420.89149.c9. [DOI] [PubMed] [Google Scholar]
- 38.de Lusignan S, Tomson C, Harris K, van Vlymen J, Gallagher H. Creatinine fluctuation has a greater effect than the formula to estimate glomerular filtration rate on the prevalence of chronic kidney disease. Nephron Clin Pract. 2011;117:c213–c224. doi: 10.1159/000320341. [DOI] [PubMed] [Google Scholar]
- 39.Inker LA, Tighiouart H, Aspelund T, Gudnason V, Harris T, Indridason OS, et al. Lifetime risk of stage 3–5 CKD in a community-based sample in Iceland. Clin J Am Soc Nephrol. 2015;10:1575–84. doi: 10.2215/CJN.00180115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.De Nicola L, Donfrancesco C, Minutolo R, Lo Noce C, Palmieri L, De Curtis A, et al. Prevalence and cardiovascular risk profile of chronic kidney disease in Italy: results of the 2008–12 National Health Examination Survey. Nephrol Dial Transplant. 2015;30:806–14. doi: 10.1093/ndt/gfu383. [DOI] [PubMed] [Google Scholar]
- 41.Minutolo R, Lapi F, Chiodini P, Simonetti M, Bianchini E, Pecchioli S, et al. Risk of ESRD and death in patients with CKD not referred to a nephrologist: a 7-year prospective study. Clin J Am Soc Nephrol. 2014;9:1586–93. doi: 10.2215/CJN.10481013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.James MT, Hemmelgarn BR, Wiebe N, Pannu N, Manns BJ, Klarenbach SW, et al. Glomerular filtration rate, proteinuria, and the incidence and consequences of acute kidney injury: a cohort study. Lancet. 2010;376:2096–103. doi: 10.1016/S0140-6736(10)61271-8. [DOI] [PubMed] [Google Scholar]
- 43.Delanaye P, El Nahas M, Glassock RJ. The myth of the future burden of CKD in United States. Am J Kidney Dis. 2015;66:171–2. doi: 10.1053/j.ajkd.2015.01.035. [DOI] [PubMed] [Google Scholar]
- 44.Hoerger TJ, Simpson SA, Yarnoff BO, Pavkov ME, Rios BN, Saydah SH, et al. The future burden of CKD in the United States: a simulation model for the CDC CKD Initiative. Am J Kidney Dis. 2015;65:403–11. doi: 10.1053/j.ajkd.2014.09.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305. doi: 10.1056/NEJMoa041031. [DOI] [PubMed] [Google Scholar]
- 46.Shlipak MG, Matsushita K, Ärnlöv J, Inker LA, Katz R, Polkinghorne KR, et al. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369:932–43. doi: 10.1056/NEJMoa1214234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367:20–9. doi: 10.1056/NEJMoa1114248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Rule AD, Bailey KR, Turner ST. What is the goal with endogenous filtration markers--estimation of GFR or prediction of kidney outcomes? Am J Kidney Dis. 2011;58:865–7. doi: 10.1053/j.ajkd.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 49.Mangione F, Dal Canton A. The epidemic of chronic kidney disease: looking at ageing and cardiovascular disease through kidney-shaped lenses. J Intern Med. 2010;268:449–55. doi: 10.1111/j.1365-2796.2010.02289.x. [DOI] [PubMed] [Google Scholar]
- 50.Roderick PJ, Atkins RJ, Smeeth L, Mylne A, Nitsch DD, Hubbard RB, et al. CKD and mortality risk in older people: a community-based population study in the United Kingdom. Am J Kidney Dis. 2009;53:950–60. doi: 10.1053/j.ajkd.2008.12.036. [DOI] [PubMed] [Google Scholar]
- 51.O’Hare AM, Bertenthal D, Covinsky KE, Landefeld CS, Sen S, Mehta K, et al. Mortality risk stratification in chronic kidney disease: one size for all ages? J Am Soc Nephrol. 2006;17:846–53. doi: 10.1681/ASN.2005090986. [DOI] [PubMed] [Google Scholar]
- 52.Muntner P, Bowling CB, Gao L, Rizk D, Judd S, Tanner RM, et al. Age-specific association of reduced estimated glomerular filtration rate and albuminuria with all-cause mortality. Clin J Am Soc Nephrol. 2011;6:2200–7. doi: 10.2215/CJN.02030311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Stengel B, Metzger M, Froissart M, Rainfray M, Berr C, Tzourio C, et al. Epidemiology and prognostic significance of chronic kidney disease in the elderly--the Three-City prospective cohort study. Nephrol Dial Transplant. 2011;26:3286–95. doi: 10.1093/ndt/gfr323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382:339–52. doi: 10.1016/S0140-6736(13)60595-4. [DOI] [PubMed] [Google Scholar]
- 55.Malmgren L, McGuigan FE, Berglundh S, Westman K, Christensson A, Åkesson K. Declining estimated glomerular filtration rate and its association with mortality and comorbidity over 10 years in elderly women. Nephron. 2015;130:245–55. doi: 10.1159/000435790. [DOI] [PubMed] [Google Scholar]
- 56.Mandelli S, Riva E, Tettamanti M, Detoma P, Giacomin A, Lucca U. Mortality prediction in the oldest old with five different equations to estimate glomerular filtration rate: The Health and Anemia Population-based Study. PLoS One. 2015;10:e0136039. doi: 10.1371/journal.pone.0136039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Xie Y, Bowe B, Xian H, Balasubramanian S, Al-Aly Z. Rate of kidney function decline and risk of hospitalizations in stage 3A CKD. Clin J Am Soc Nephrol. 2015;10:1946–55. doi: 10.2215/CJN.04480415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Raymond NT, Zehnder D, Smith SC, Stinson JA, Lehnert H, Higgins RM. Elevated relative mortality risk with mild-to-moderate chronic kidney disease decreases with age. Nephrol Dial Transplant. 2007;22:3214–20. doi: 10.1093/ndt/gfm396. [DOI] [PubMed] [Google Scholar]
- 59.Quinn MP, Cardwell CR, Kee F, Maxwell AP, Savage G, McCarron P, et al. The finding of reduced estimated glomerular filtration rate is associated with increased mortality in a large UK population. Nephrol Dial Transplant. 2011;26:875–80. doi: 10.1093/ndt/gfq505. [DOI] [PubMed] [Google Scholar]
- 60.Thompson S, James M, Wiebe N, Hemmelgarn B, Manns B, Klarenbach S, et al. Cause of death in patients with reduced kidney function. J Am Soc Nephrol. 2015;26:2504–11. doi: 10.1681/ASN.2014070714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Ricardo AC, Flessner MF, Eckfeldt JH, Eggers PW, Franceschini N, Go AS, et al. Prevalence and correlates of CKD in Hispanics/Latinos in the United States. Clin J Am Soc Nephrol. 2015;10:1757–66. doi: 10.2215/CJN.02020215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.O’Hare AM, Choi AI, Bertenthal D, Bacchetti P, Garg AX, Kaufman JS, et al. Age affects outcomes in chronic kidney disease. J Am Soc Nephrol. 2007;18:2758–65. doi: 10.1681/ASN.2007040422. [DOI] [PubMed] [Google Scholar]
- 63.O’Hare AM, Hotchkiss JR, Kurella TM, Larson EB, Hemmelgarn BR, Batten A, et al. Interpreting treatment effects from clinical trials in the context of real-world risk information: end-stage renal disease prevention in older adults. JAMA Intern Med. 2014;174:391–7. doi: 10.1001/jamainternmed.2013.13328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tangri N, Stevens LA, Griffith J, Tighiouart H, Djurdjev O, Naimark D, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011;305:1553–9. doi: 10.1001/jama.2011.451. [DOI] [PubMed] [Google Scholar]
- 65.Qaseem A, Hopkins RH, Jr, Sweet DE, Starkey M, Shekelle P. Screening, monitoring, and treatment of stage 1 to 3 chronic kidney disease: A clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159:835–47. doi: 10.7326/0003-4819-159-12-201312170-00726. [DOI] [PubMed] [Google Scholar]
- 66.El-Nahas M. Cardio-Kidney-Damage: a unifying concept. Kidney Int. 2010;78:14–8. doi: 10.1038/ki.2010.123. [DOI] [PubMed] [Google Scholar]
- 67.Elseviers MM, Verpooten GA, De Broe ME, De Backer GG. Interpretation of creatinine clearance. Lancet. 1987;1:457. doi: 10.1016/s0140-6736(87)90167-x. [DOI] [PubMed] [Google Scholar]
- 68.Ma YC, Zuo L, Chen L, Su ZM, Meng S, Li JJ, et al. Distribution of measured GFR in apparently healthy Chinese adults. Am J Kidney Dis. 2010;56:420–1. doi: 10.1053/j.ajkd.2010.05.005. [DOI] [PubMed] [Google Scholar]
- 69.Jafar TH, Islam M, Jessani S, Bux R, Inker LA, Mariat C, et al. Level and determinants of kidney function in a South Asian population in Pakistan. Am J Kidney Dis. 2011;58:764–72. doi: 10.1053/j.ajkd.2011.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Swanney MP, Ruppel G, Enright PL, Pedersen OF, Crapo RO, Miller MR, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008;63:1046–51. doi: 10.1136/thx.2008.098483. [DOI] [PubMed] [Google Scholar]
- 71.James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8) JAMA. 2014;311:507–20. doi: 10.1001/jama.2013.284427. [DOI] [PubMed] [Google Scholar]
- 72.Coresh J, Levey AS, Levin A, Stevens P. A stable definition of chronic kidney disease improves knowledge and patient care. BMJ. 2013;347:f5553. doi: 10.1136/bmj.f5553. [DOI] [PubMed] [Google Scholar]
- 73.Levey AS, Inker LA, Coresh J. Chronic kidney disease in older people. JAMA. 2015;314:557–8. doi: 10.1001/jama.2015.6753. [DOI] [PubMed] [Google Scholar]
- 74.Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med. 1993;329:1456–62. doi: 10.1056/NEJM199311113292004. [DOI] [PubMed] [Google Scholar]
- 75.Pottel H, Vrydags N, Mahieu B, Vandewynckele E, Croes K, Martens F. Establishing age/sex related serum creatinine reference intervals from hospital laboratory data based on different statistical methods. Clin Chim Acta. 2008;396:49–55. doi: 10.1016/j.cca.2008.06.017. [DOI] [PubMed] [Google Scholar]
- 76.Schaeffner ES, Ebert N, Delanaye P, Frei U, Gaedeke J, Jakob O, et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann Intern Med. 2012;157:471–81. doi: 10.7326/0003-4819-157-7-201210020-00003. [DOI] [PubMed] [Google Scholar]
- 77.Moyer VA. Screening for chronic kidney disease: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:567–70. doi: 10.7326/0003-4819-157-8-201210160-00533. [DOI] [PubMed] [Google Scholar]
- 78.Span P. A diagnosis of dubious meaning. New York Times; Tuesday: Sep 15, 2015. p. D5. [Google Scholar]