

Abstract
Adult intussusception is rare and laparotomy is required in most of the cases due to the potential pathologic underlying reasons. Although it is technically challenging, single-incision laparoscopic surgery can work as an alternative to laparotomy. Here we report the case of a 45-year-old man with intermittent right lower quadrant abdominal pain for 1 month. Abdominal enhanced computed tomography (CT) scan was performed and ileo-ileal intussusception was found, with lipoma as a likely leading point. Ileal resection was performed using the single-incision laparoscopic-assisted technique. Multiple trocars in the umbilical incision technique and conventional instruments were used. After identification of the ileo-ileal intussusception, the involved small bowel was extracted from the umbilical incision, and resection and anastomosis were performed extracoporeally. The operation time was 65 min and the post-operative hospital stay was 2 days. The patient recovered uneventfully, with better cosmetic results.
Keywords: Adult intussusception, ileal polyp, single-incision laparoscopic surgery
INTRODUCTION
Intussusception rarely occurs in adults and almost 90% of adult intussusceptions are secondary to a pathologic condition.[1,2,3] Laparotomy therefore remains the major management of adult intussusception. Although it has been adopted to manage adult intussusception, the laparoscopic approach does not evolve very quickly due to technical challenges, especially in those for whom intestinal resection is required. However, the advantages of the laparoscopic approach, including confirmation of the diagnosis, rapid recovery, less pain and better cosmetic results, are still appealing.[4] More recently, single-incision laparoscopic surgery (SILS) has been applied to different disciplines including cholecystectomy and appendectomy. Compared with conventional laparoscopy, it is not necessary for SILS to make another big incision on the abdominal wall. All the procedures, including identifying the lesion, extracting the involved bowel and performing the anastomosis can be accomplished through the umbilical incision. Here we report ileal resection in an adult patient with ileo-ileal intussusception using SILS-assisted technique with a good result.
CASE REPORT
A 45-year-old male presented with intermittent right lower quadrant abdominal pain for one month. There was no positive sign for physical examination. Abdominal enhanced computed tomography (CT) scan was performed and ileo-ileal intussusception was found. The ileal lipoma was diagnosed as the possible leading point. [Figure 1a and b]. Single-incision laparoscopic surgery was performed with the approval of the patient.
Figure 1.
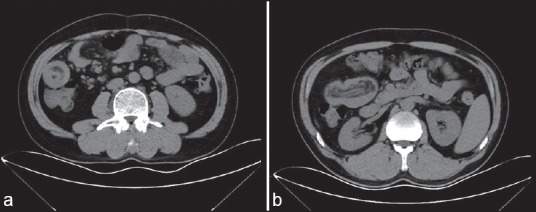
(a) Image of ileo-ileal intussusception on CT (b) Image of ileo-ileal intussusception on CT
The patient was placed in supine position under general anaesthesia. The conventional laparoscopic instruments were used. After pneumoperitonium was established, a 10-mm trocar was placed in the umbilical incision for camera access. An ileo-ileal intussusception was found through careful laparoscopic inspection [Figure 2]. The umbilical incision was then enlarged to 3 cm without cutting the anterior sheath of the rectus abdominis or linea alba in case of air leakage. Two other 5-mm trocars were implanted in the same incision [Figure 3]. The ileocecal region was identified first and the small bowel was gently detected to locate the lesion using two atraumatic forceps.
Figure 2.
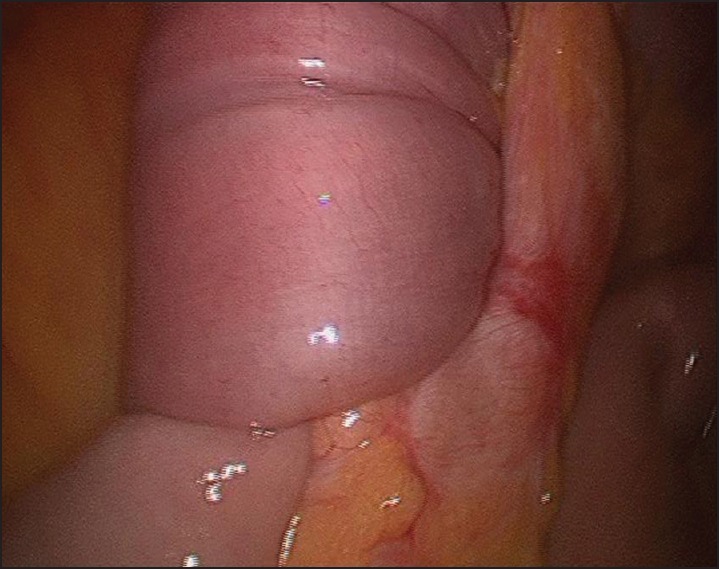
Identification of ileo-ileal intussusception under laparoscopy
Figure 3.

Multiple-trocar use in single umbilical incision and conventional instruments
The ileo-ileal intussusception was located 60 cm away from the ileocecal region. Attempts to reduce the intussusception failed [Figure 4]. The holes for trocar access were connected to make a 3-cm incision. A disposable incision protector (Qingdao Huaren Mecial Product Co. Ltd, Qingdao, China) was inserted into the incision and the involved ileum was pulled out of the incision [Figure 5]. Ileal resection was performed the same as open procedures. An approximately 20-cm-long involved ileum was removed. After the anastomosis, the ileum was returned to the abdominal cavity. After careful inspection of the abdominal cavity for leakage or blooding, the umbilical incision was closed carefully using absorbable monofilament sutures.
Figure 4.
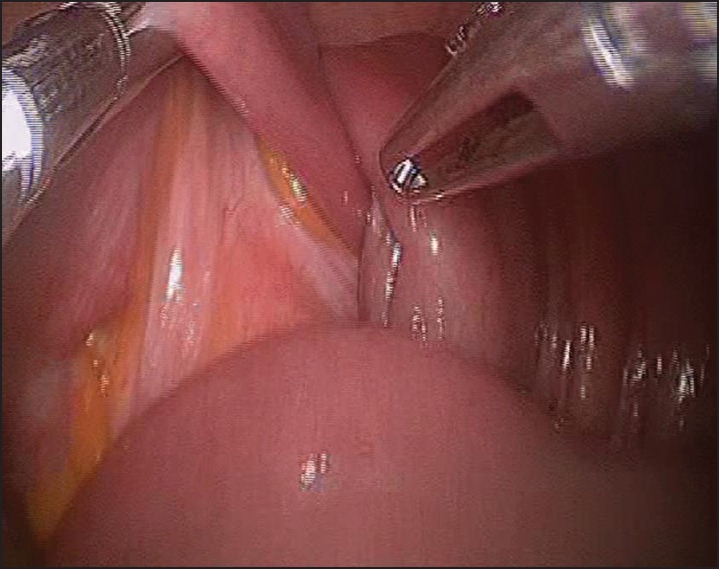
The attempt to reduce the intussusception under laparoscopy
Figure 5.
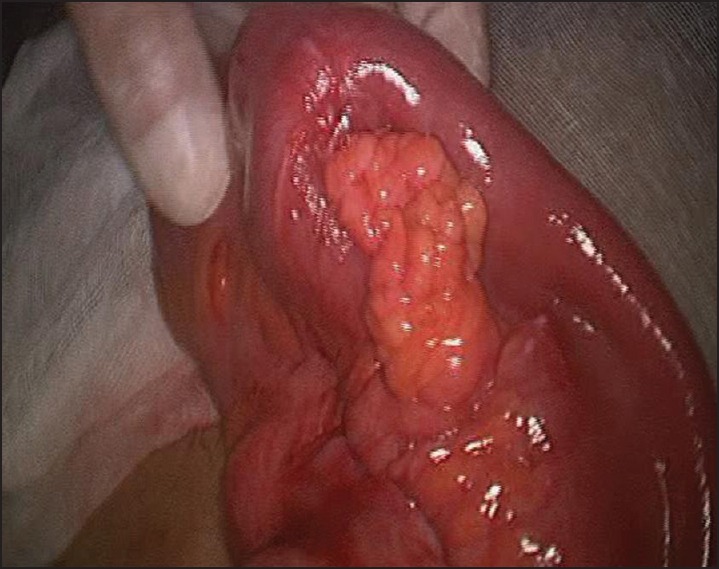
The involved small bowel was extracted out through umbilical incision
The operation time was 65 min and the blood lost was 10 mL. The post-operative time before the patient left the bed was 6 h and 40 mg parecoxib was used after the surgery. Bowel function recovered and the gastric tube was removed the following morning. The patient was discharged on post-operative day 3 without any complication. A microscopic examination revealed inflammatory polyp [Figure 6a and b]. The patient was extremely satisfied with the cosmetic results [Figure 7a and b].
Figure 6.
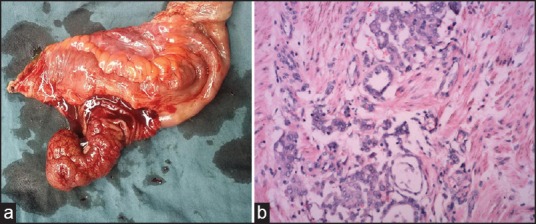
(a) The resected specimen (b) the microscopic pathology examination
Figure 7.
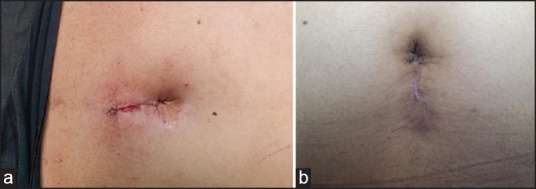
(a) The incision right after the surgery (b) the wound 1 month later
DISCUSSION
Intussusception is common in children but rare in adults. Most of the cases of adult intussusception have a leading point such as lipoma, gastrointestinal stroma tumour or submucosal fibroma.[5,6,7] Surgical resection of the involved bowel, therefore, is regarded as the treatment of choice in adult intussusception.
Due to the proven advantages of laparoscopic surgeries, such as minimal incision, less pain and faster recovery, the laparoscopic approach has been increasingly adopted for the treatment of adult intussusception in recent years.[8,9] However, when bowel resection is required, an additional incision has to be made.
Single-incision laparoscopic surgery has been approved to be safe and feasible in surgeries such as cholecystectomy,[10] appendectomy[11] and colectomy,[12] with better cosmetic results and less pain. In addition, one slightly bigger incision makes it possible to pull the bowel out of the abdominal cavity without extra incisions as in traditional laparoscopy.
We report a case in which the ingested foreign body was removed through the single-incision laparoscopic technique, with very good results.[13]
In this case, we made the diagnosis before the surgery thanks to the CT scan. The leading point was also preoperatively located in the ileum. Although the nature of the lesion could not be confirmed, the incidence of a benign tumour or an inflammatory condition is more common than malignancy in small-bowel intussusception compared with colonic intussusception.[14]
The identification of the involved ileum was easy. Intracorporeal reduction was carefully performed, but it failed. Mandatory reduction is not recommended so as to avoid bowel perforation and the potential seeding of malignant cells to other sites.[15] It is also important to insert a protective cover to protect the incision before the ileum is extracted in the potential malignant case. After the returning of the ileum, careful inspection is also important to avoid future leakage and blooding.
In addition to the rapid recovery and short hospital stay, the better cosmetic result was the biggest advantage for this case.
CONCLUSION
The single-incision laparoscopic-assisted technique is safe and feasible in the treatment of adult intussusception, with good cosmetic results.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
REFERENCES
- 1.Honjo H, Mike M, Kusanagi H, Kano N. Adult intussusception: A retrospective review. World J Surg. 2015;39:134–8. doi: 10.1007/s00268-014-2759-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lianos G, Xeropotamos N, Bali C, Baltoggiannis G, Ignatiadou E. Adult bowel intussusception: Presentation, location, etiology, diagnosis and treatment. G Chir. 2013;34:280–3. [PMC free article] [PubMed] [Google Scholar]
- 3.Wang N, Cui XY, Liu Y, Long J, Xu YH, Guo RX, et al. Adult intussusception: A retrospective review of 41 cases. World J Gastroenterol. 2009;15:3303–8. doi: 10.3748/wjg.15.3303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Goldstein L, Iqbal A, Tan S. Laparoscopic treatment of adult intussusception. Am Surg. 2014;80:e187–8. [PubMed] [Google Scholar]
- 5.Gelabert C, Torradas J, Nelson M. Ileocolic intussusception secondary to gastrointestinal stromal tumor in a 61-year-old. Am J Emerg Med. 2014;32:1301.e1–2. doi: 10.1016/j.ajem.2014.03.037. [DOI] [PubMed] [Google Scholar]
- 6.Joyce KM, Waters PS, Waldron RM, Khan I, Orosz ZS, Németh T, et al. Recurrent adult jejuno-jejunal intussusception due to inflammatory fibroid polyp — Vanek's tumour: A case report. Diagn Pathol. 2014;9:127. doi: 10.1186/1746-1596-9-127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Namikawa T, Hokimoto N, Okabayashi T, Kumon M, Kobayashi M, Hanazaki K. Adult ileoileal intussusception induced by an ileal lipoma diagnosed preoperatively: Report of a case and review of the literature. Surg Today. 2012;42:686–92. doi: 10.1007/s00595-011-0092-6. [DOI] [PubMed] [Google Scholar]
- 8.Kang SI, Kang J, Kim MJ, Kim IK, Lee J, Lee KY, et al. Laparoscopic-assisted resection of jejunojejunal intussusception caused by a juvenile polyp in an adult. Case Rep Surg 2014. 2014 doi: 10.1155/2014/856765. 856765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tartaglia D, Bertolucci A, Palmeri M, Kauffmann EF, Napoli N, Galatioto C, et al. The role of laparoscopy in adult bowel obstruction caused by intussusception. Ann Ital Chir. 2014;85:328–31. [PubMed] [Google Scholar]
- 10.Chang SK, Wang YL, Shen L, Iyer SG, Madhavan K. A randomized controlled trial comparing post-operative pain in single-incision laparoscopic cholecystectomy versus conventional laparoscopic cholecystectomy. World J Surg. 2015;39:897–904. doi: 10.1007/s00268-014-2903-6. [DOI] [PubMed] [Google Scholar]
- 11.Xu AM, Huang L, Li TJ. Single-incision versus three-port laparoscopic appendectomy for acute appendicitis: Systematic review and meta-analysis of randomized controlled trials. Surg Endosc. 2015;29:822–43. doi: 10.1007/s00464-014-3735-z. [DOI] [PubMed] [Google Scholar]
- 12.Carus T. Current advances in single-port laparoscopic surgery. Langenbecks Arch Surg. 2013;398:925–9. doi: 10.1007/s00423-013-1113-2. [DOI] [PubMed] [Google Scholar]
- 13.Yu H, Wu S, Yu X, Zhang Q. Single-incision laparoscopic surgery for ingested foreign body removal. Am J Emerg Med. 2014;32:290. e1–3. doi: 10.1016/j.ajem.2013.10.007. [DOI] [PubMed] [Google Scholar]
- 14.Potts J, Al Samaraee A, El-Hakeem A. Small bowel intussusception in adults. Ann R Coll Surg Engl. 2014;96:11–4. doi: 10.1308/003588414X13824511650579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kim BS, Kang KH, Park HC, Lee BH. Laparoscopic colectomy of colonic intussusceptions in adults. J Korean Surg Soc. 2012;83:397–402. doi: 10.4174/jkss.2012.83.6.397. [DOI] [PMC free article] [PubMed] [Google Scholar]