

Abstract
Purpose
To highlight teaching hospitals' efforts to reduce readmissions by describing interventions implemented to improve care transitions for heart failure (HF) patients and the variability in implemented HF-specific and care transition interventions.
Method
In 2012, the authors surveyed a network of 17 teaching hospitals to capture information about the number, type, stage, and structure of 4 HF-specific and 21 care transition (pre-discharge, bridging, and post-discharge) interventions implemented to reduce readmissions among patients with HF. The authors summarized data using descriptive statistics, including the mean number of interventions implemented and the frequency and stage of specific interventions, and descriptive plots of the structure of two common interventions (multidisciplinary rounds and follow-up telephone calls).
Results
Sixteen hospitals (94%) responded. The number and stage of the HF-specific and care transition interventions implementation varied across institutions. The mean number of interventions at an advanced stage of implementation (i.e., implemented for ≥ 75% of HF patients on the cardiology service or on all services) was 10.9 (SD = 4.3). Overall, predischarge interventions were more common than bridging or postdischarge interventions. There was variability in the personnel involved in multi-disciplinary rounds and in the processes/content of follow-up telephone calls.
Conclusions
Teaching hospitals have implemented a wide range of interventions aimed at reducing hospital readmissions, but there is substantial variability in the types, stages, and structure of their interventions. This heterogeneity highlights the need for collaborative efforts to improve understanding of intervention effectiveness.
Hospital readmissions can indicate poor quality of care, and they generate excess costs for the U.S. health care system. Jencks et al, for example, showed that one-fifth of Medicare beneficiaries experienced a rehospitalization within 30 days of discharge, at a cost of more than $17 billion dollars in 2004.1 Although readmissions are prevalent across all conditions, heart failure (HF) is especially relevant. For example, among Medicare beneficiaries admitted to the hospital for all causes, the unadjusted 30-day rate of all-cause readmission was 23% in 2006 and HF was the most frequent cause of readmission.2
Increased regulatory focus has shined a brighter light on readmissions in the form of public reporting and financial penalties. The Centers for Medicare and Medicaid Services publicly reports hopsitals' risk-standardized readmission rates for patients admitted for selected conditions, including HF.1,3–5 Teaching hospitals are not exempt from this scrutiny and, compared with non-teaching hospitals, face increased odds (odds ratio = 1.56; 95% confidence interval, 1.04 to 2.32) of reduced levels of reimbursement for increased rates of 30-day readmissions.6,7
In an attempt to reduce readmissions among patients with HF, hospitals have implemented broad range of HF-specific and care transition interventions. Care transition interventions include predischarge interventions (e.g., multidisciplinary rounds), “bridging” interventions that span the hospital and post-hospital settings (e.g., transitions coach), and postdischarge interventions (e.g., follow-up telephone calls).8 While the menu of care transition interventions is expansive, findings related to the efficacy of any single intervention have been mixed. 8–12 Hospitals, therefore, are trying to reduce readmission rates while relying on mixed evidence to guide their improvement efforts.13 This may result in considerable variations in the interventions implemented, which may, in turn, lead to variable quality of care and variable outcomes.14–16
Teaching hospitals, therefore, have a significant incentive to reduce their readmission rate and a number of potential interventions that they can employ to reduce readmissions. It is unclear, however, how teaching hospitals are responding to the environment of increasing accountability for readmissions. Establishing baseline knowledge of the interventions they are employing may demonstrate the level of teaching hospital engagement in efforts to reduce rehospitalization rates and potentially stimulate collaboration across institutions. In addition, describing current structures and processes of care transition interventions may illuminate the challenges of allocating resources when evidence is limited.
To highlight teaching hospitals' efforts to reduce readmissions, we surveyed a network of teaching hospitals to (a) describe interventions being implemented to improve care transitions for patients hospitalized with HF and (b) understand what variability, if any, exists in the number, type, implementation stage, and structure of selected HF-specific and care transition interventions.
Method
Hospital sample selection
We surveyed a teaching hospital network known as the Variations Collaborative Study Group. This was a convenience sample, organized by the Association of American Medical Colleges, to evaluate resource utilization and outcomes in HF patients. The study group consisted of 14 U.S. academic medical centers, representing 17 affiliated teaching hospitals. Participation in the study group and in this study were voluntary. The research was approved by Vanderbilt University's institutional review board.
Questionnaire development
At the time of questionnaire development, there were no validated organizational-level survey instruments to explicitly examine care transition interventions. Therefore, we did not draw specific questions from prior surveys; rather, questions were informed by the published literature8–10,17–20 and input from an advisory group composed of hospital executives, clinicians, investigators, and content experts from the Variations Collaborative Study Group. The interventions included in the questionnaire were determined by group consensus.
The initial version of the questionnaire included 4 HF-specific interventions and 21 care transition interventions (predischarge, bridging, and post-discharge) that fell within 11 of the 12 intervention categories described by Hansen et al in their recent systematic review of interventions aimed at reducing 30-day rehospitalizations.8 Categorization was not strictly defined but it served as a framework to broadly understand the range of interventions, from in-hopital to home-based. The 11 categories were patient education, discharge planning, medication management, appointment scheduling before discharge, timely primary care provider communication, timely clinic follow-up, follow-up telephone calls, home visitation, transition coach, patient-centered discharge instructions, and provider continuity. (Hansen et al's twelfth category, telephone hotline, was not explicitly included in our survey.) Based upon experts' recommendations, we added a category of advance care planning to address exploring care goals with patients with advanced HF.21,22 These goals may include palliative care and/or hospice options rather than repeat hospitalization.
We pilot tested the initial version of the questionnaire across participating study group sites. Based on the feedback received, we clarified items and added questions about respondent characteristics; no new interventions were added. It was believed that, although many hospitals conduct similar types of interventions, it was important for the survey to capture implementation stages at individual hospitals. In addition, we wanted to capture that HF care occurs in multiple care units (e.g. cardiology unit, general medical ward). Therefore, in the final version of the questionnaire, we asked respondents to rate the stage of intervention implementation according to a 5-point Likert scale that ranged from targeted to the broadest populations, as follows: 1 = not implemented or being considered, 2 = pilot testing only, 3 = advanced HF patients only, 4 = ≥ 75% of all HF patients on the cardiology service, and 5 = ≥ 75% of patients with HF on all services. We chose 75% as the cutoff to reflect implementation for “most” patients with HF. Finally, for two commonly implemented interventions, we asked for additional information about intervention structure: the personnel who participate in multidisciplinary rounds and the processes/content of post-discharge follow-up telephone calls. For these two interventions, in the Results, we also report stage of implementation to provide a qualitative assessment of the variability of implementation across an intervention.
Survey distribution and participants
We e-mailed the final questionnaire and consent forms to a representative at each of the 17 teaching hospitals in the Variations Collaborative Study Group, beginning on May 1, 2012. In the survey instructions we asked that a single questionnaire per hospital be completed, by a leader or leaders who could readily describe staff organization, inpatient HF-specific interventions, and care transition interventions. We encouraged respondents to seek assistance if others could provide more complete and accurate responses to specific questions. We asked respondents to answer all questions referenced to May 2012. The final completed survey was received by the investigative team in October 2012.
Hospital characteristics
Hospital respondent data were linked with data from the University HealthSystem Consortium (UHC) databases.23 We assessed hospital characteristics--including staffed beds, annual HF admissions, and geographic location. We also obtained individual hospital outcomes from 2012, including risk-standardized HF in-hospital mortality and unadjusted all-cause HF readmission rates from the UHC databases. We included outcomes for descriptive purposes only, because the large number of interventions compared with the smaller sample of study hospitals limited multivariable process-outcomes analyses (i.e., lack of statistical power).
Statistical analysis and intervention variability
We performed bivariable analyses to compare organizational characteristics of respondent hospitals with those of other UHC-member U.S. teaching hospitals. We compared continuous data with Student's t-tests or Mann-Whitney tests and categorical data with chi-square tests, as appropriate.
We then described multiple forms of variability in the HF-specific and care transition interventions across the respondent hospitals, as indicated below. All analyses were conducted in Stata/SE version 11.2 (StataCorp LP, College Station, Texas).
Number of interventions
We calculated the mean and standard deviation (SD) of the total number of interventions implemented across hospitals that were reported as being at an advanced stage of implementation (i.e., ≥ 75% of all HF patients on the cardiology service or on all services). This was assessed for HF-specific interventions as well as predischarge, bridging, and post-discharge care transition interventions. We ordered hospitals according to number of interventions implemented at an advanced stage, labeling hospitals from “A” (the most) to “P” (the fewest).
Types of interventions
To understand the most and least commonly implemented interventions, we determined the number and percentage of respondent hospitals at which each intervention was at an advanced stage of implementation (i.e., ≥ 75% of all HF patients on the cardiology service or on all services). This was assessed for HF-specific interventions as well as predischarge, bridging, and post-discharge care transition interventions.
Stage of implementation
For two care transition interventions, multidisciplinary rounds and follow-up telephone calls, we described the stage of implementation using the same 5-point Likert scale as above (1 = not implemented or being considered, 2 = pilot testing only, 3 = advanced HF patients only, 4 = ≥ 75% of all HF patients on the cardiology service, and 5 = ≥ 75% of patients with HF on all services) to indicate the qualitative differences in stage of implementation.
Intervention structure—personnel and processes/content
We created a descriptive plot of the hospital-specific personnel who participate in multidisciplinary rounds (e.g., nurse, pharmacist). We also created a descriptive plot of the specific processes/content of post-discharge follow-up telephone calls (e.g., dietary counseling).
Results
Hospital characteristics and survey respondents
Responses were received from 16 of the 17 affiliated hospitals in the Variations Collaborative Study Group (response rate 94%). All 14 academic medical centers in the study group were represented.
The median number of staffed beds at the respondent hospitals was 683 (interquartile range [IQR], 515 to 890) (see Table 1). The mean (SD) all-cause 30-day readmission rate for patients with HF was 21.3% (5.0%). All respondent hospitals were urban and most were in the Western U.S. Census region. Compared with other U.S. teaching hospitals in the UHC database, respondent hospitals had more staffed beds, admitted more patients with HF, and were more likely to have a heart transplant program (all significant at P < .001). There were no statistically significant differences in readmission and mortality outcomes.
Table 1. Characteristics Of Respondent Teaching Hospitals, 2012 Survey On Implementation Of Heart Failure (Hf)-Specific And Care Transition Interventions For Hf Patientsa.
| Hospital characteristicb | Respondent hospitals (n =16) | Other UHC hospitals (n = 191) | P valuec |
|---|---|---|---|
| U.S. Census region, no. (%) | .80 | ||
| West | 7 (44) | 62 (32) | |
| Northeast | 4 (25) | 54 (28) | |
| South | 3 (19) | 52 (27) | |
| Midwest | 2 (13) | 23 (12) | |
| Urban location, no. (%) | 16 (100) | 174 (91) | .21 |
| No. of staffed hospital beds, median (IQR) | 683 (515 to 890) | 403 (158 to 553) | < .001 |
| Annual no. of HF admissions, median (IQR) | 729 (433 to 937) | 462 (205 to 672) | < .001 |
| Hospital-owned/managed home health service, no. (%) | .02 | ||
| Yes | 7 (44) | 36 (19) | |
| No | 9 (56) | 112 (59) | |
| Unknown | 0 (0) | 43 (23) | |
| Hospital-owned/managed hospice service, no. (%) | .23 | ||
| Yes | 5 (31) | 34 (18) | |
| No | 11 (69) | 112 (59) | |
| Unknown | 0 (0) | 42 (22) | |
| Presence of non-ICU-based inpatient HF unit, no. (%)d | 5 (36) | N/A | |
| Heart transplant program, no. (%) | 12 (75) | 50 (26) | <.001 |
| Annual no.of heart transplant patients, median (IQR) | 25 (12 to 45) | 20 (10 to 25) | .03 |
| 30-day all cause HF readmission rate, mean (SD) | 21.3 (5.0) | 20.0 (4.8) | .30 |
| Risk-standardized HF in-hospital mortality, mean (SD) | 2.9 (1.3) | 3.0 (2.1) | .85 |
Abbreviations: UHC indicates University HealthSystem Consortium;IQR, interquartile range; ICU, intensive care unit; SD, standard deviation.
The respondent hospitals were part of the Variations Collaborative Study Group, a convenience sample of teaching hospitals organized to evaluate resource utilization and outcomes in HF patients. This teaching hospital network included 14 U.S. academic medical centers, representing 17 affiliated hospitals. All of the study group hospitals were part of the UHC.
Data source: UHC databases,23 unless otherwise noted.
Pvalues based on chi-square test of statistical independence for categorical data, Student's t-test for parametric data, or Mann-Whitney rank sum test for non-parametric data.
Data from study survey; not available from UHC databases.
Nineteen individuals (mean = 1.1 respondents per hospital) completed the questionnaire. The largest number of respondents held leadership positions in HF programs (n = 8, 42%), followed respondents who were leaders in quality and safety programs (n = 4, 21%) and cardiology faculty (n = 4, 21%). Respondents' professional backgrounds varied, with the largest number being physicians (n = 9, 47%). Respondents had been in their current position for a median of 4.5 years (IQR, 2.0 to 7.5) (see Supplemental Digital Appendix 1 at [LWW INSERT LINK].)
Intervention variability
Number of interventions
There was variability across respondent sites in the total number of interventions at an advanced stage of implementation (i.e., implemented for ≥75% of HF patients on the cardiology service or on all services) (Figure 1). The mean number of interventions implemented at an advanced stage, including HF-specific and care transition interventions, for this population was 10.9 (SD = 4.3) of a possible 25.
Figure 1.
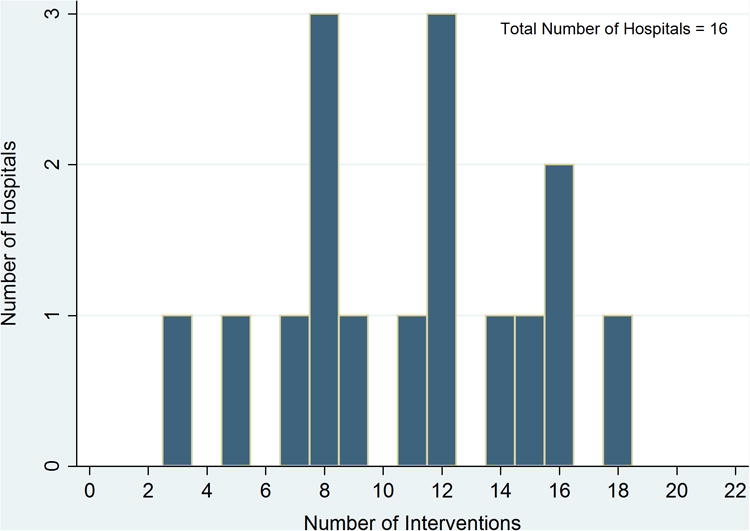
Distribution of the total number of heart-failure specific and care transition interventions implemented for at least 75% of heart failure patients on the cardiology service, across the 16 respondent U.S. teaching hospitals, as of May 2012.
Types of interventions
There was variability across respondent sites in the types of interventions at an advanced stage of implementation. Of the HF-specific interventions (Table 2), the majority of hospitals had dedicated inpatient HF teams (n = 12; 75%), whereas few had an emergency department HF management protocol (n = 3; 19%). Among care transitions interventions, the most common predischarge interventions (Table 3) were the initiation of early discharge planning beginning in the first 48 hours (n = 16, 100%) and daily multidisciplinary rounds (n = 13, 81%) (Table 3). Among the bridging interventions (Table 4), use of personal health records was the most common (n = 4, 25%). The most common post-discharge intervention (Table 5) was the arrangement of clinic follow-up appointments within 14 days (n = 12, 75%). Overall, predischarge interventions were more commonly implemented compared with bridging or post-discharge interventions.
Table 2. Heart Failure (HF)-Specific Interventions at an Advanced Stage of Implementation,Across Respondent Hospitals (n = 16), 2012 Surveya.
| HF-specific interventionb | Hospitalc | No. (%) of hospitals | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | C | D | E | H | I | B | K | G | F | J | L | M | N | O | P | ||
| Inpatient HF team | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 12 (75) | ||||
| HF admission order set | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (63) | ||||||
| Advanced HF clinic | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 7 (44) | |||||||||
| Emergency department HF management protocol | ✓ | ✓ | ✓ | 3 (19) | |||||||||||||
| Total no.of interventions | 4 | 4 | 4 | 3 | 3 | 3 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | — |
Respondent hospitals were part of the Variations Collaborative Study Group, a convenience sample of 14 U.S. academic medical centers, representing 17 affiliated hospitals.
Interventions are ordered from the most common to the least common (top to bottom).
Each check mark represents an advanced stage of implementation of the specified intervention (i.e., for ≥75% of heart failure patients on the cardiology service or on all services) as of May 2012.Hospitals are ordered from those that implemented the most HF-specific interventions to those that implemented the fewest (left to right). Hospital letters correspond to the total number of HF-specific and care transition interventions implemented at an advanced stage, from the most (Hospital A) to the fewest (Hospital P).
Table 3. Predischarge Care Transition Interventions at an Advanced Stage of Implementation,Across Respondent Hospitals (n = 16), 2012 Surveya.
| Predischarge interventionb | Hospitalc | No. (%) of hospitals | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | A | C | D | F | G | H | E | I | M | J | L | N | K | P | O | ||
| Initiation of early discharge planning in first 48 hours | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 16 (100) |
| Daily multi-disciplinary rounds | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 13 (81) | |||
| Verification of financial means to fill prescription | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 12 (75) | ||||
| Reconciled medication list in patient-friendly language | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 11 (69) | |||||
| Routine assessment of advance directives | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 11 (69) | |||||
| Daily teach backd | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (63) | ||||||
| Discharge teach backd | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (63) | ||||||
| Medications provided to those without financial means | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 8 (50) | ||||||||
| Routine pharmacist counseling | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 6 (38) | ||||||||||
| Transportation arrangements confirmed | ✓ | 1 (13) | |||||||||||||||
| Pill box for patients | ✓ | 1 (13) | |||||||||||||||
| Standing home health orders | 0 (0) | ||||||||||||||||
| Total no.of interventions | 9 | 8 | 8 | 8 | 8 | 8 | 8 | 6 | 6 | 6 | 5 | 5 | 5 | 4 | 3 | 2 | — |
Respondent hospitals were part of the Variations Collaborative Study Group, a convenience sample of 14 U.S. academic medical centers, representing 17 affiliated hospitals.
Interventions are ordered from the most common to the least common (top to bottom).
Each check mark represents an advanced stage of implementation of the specified predischarge intervention (i.e., for ≥75% of heart failure patients on the cardiology service or on all services) as of May 2012. Hospitals are ordered from those that implemented the most predischarge interventions to those that implemented the fewest (left to right). Hospital letters correspond to the total number of HF-specific and care transition interventions implemented at an advanced stage, from the most (Hospital A) to the fewest (Hospital P).
Teach back refers to provider assessment of patient/caregiver understanding of the discharge plan by asking them to teach it back.
Table 4. Bridging Care Transition Interventions at an Advanced Stage of Implementation,Across Respondent Hospitals (n = 16), 2012 Surveya.
| Bridging interventionb | Hospitalc | No. (%) of hospitals | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | E | G | I | M | B | C | D | F | H | J | K | L | N | O | P | ||
| Personal health records are provided | ✓ | ✓ | ✓ | ✓ | 4 (25) | ||||||||||||
| Provider from team accompanies patient to clinic | ✓ | 1 (6) | |||||||||||||||
| Nurse visits patient if discharged to SNF | ✓ | 1 (6) | |||||||||||||||
| Physician visits patient if discharged to SNF | ✓ | 1 (6) | |||||||||||||||
| Total no.of interventions | 3 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | — |
Abbreviation: SNF indicates skilled nursing facility.
Respondent hospitals were part of the Variations Collaborative Study Group, a convenience sample of 14 U.S. academic medical centers, representing 17 affiliated hospitals.
Bridging interventions span the hospital and post-hospital settings. Interventions are ordered from the most common to the least common (top to bottom).
Each check mark represents an advanced stage of implementation of the specified intervention (i.e., for ≥75% of heart failure patients on the cardiology service or on all services)as of May 2012. Hospitals are ordered from those that implemented the most bridging interventions to those that implemented the fewest (left to right).Hospital letters correspond to the total number of HF-specific and care transition interventions implemented at an advanced stage, from the most (Hospital A) to the fewest (Hospital P).
Table 5. Post-discharge Care Transition Interventions at an Advanced Stage of Implementation,Across Respondent Hospitals (n = 16), 2012 Surveya.
| Postdischarge interventionb | Hospitalc | No. (%) of hospitals | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | C | E | A | D | F | G | J | K | L | O | H | I | N | M | P | ||
| Follow-up clinic appointment arranged within 14 days | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 12 (75) | ||||
| Discharge summary sent to receiving MD within 24 hours | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (63) | ||||||
| Follow-up telephone call made in first week | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 7 (44) | |||||||||
| Remote physiologic monitoring | ✓ | ✓ | ✓ | ✓ | 4 (25) | ||||||||||||
| Home health worker visits, even if patient does not meet CMS reimbursement requirements | ✓ | ✓ | 2 (13) | ||||||||||||||
| Total no. of interventions | 5 | 4 | 4 | 3 | 3 | 3 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | — |
Abbreviations: MD, indicates physician; CMS, Centers for Medicare and Medicaid Services
Respondent hospitals were part of the Variations Collaborative Study Group, a convenience sample of 14 U.S. academic medical centers, representing 17 affiliated hospitals.
Interventions are ordered from the most common to the least common (top to bottom).
Each check mark represents an advanced stage of implementation of the specified intervention (i.e., for ≥75% of heart failure patients on the cardiology service or on all services) as of May 2012. Hospitals are ordered from those that implemented the most post-discharge interventions to those that implemented the fewest (left to right).Hospital letters correspond to the total number of HF-specific and care transition interventions implemented at an advanced stage, from the most (Hospital A) to the fewest (Hospital P).
Stage of implementation
Across respondent hospitals, there was variability in the stage of implementation of multidisciplinary rounds and post-discharge follow-up telephone calls (see Supplemental Digital Appendixes 2 and 3, respectively, at [LWW INSERT LINK]). The implementation stage for each of these interventions ranged from not implemented to implemented for ≥ 75% of all patients with HF, although greater numbers of hospitals reported the latter (multidisplinary rounds: not implemented = 1 [6%] vs. implemented for ≥ 75% of patients with HF on all services = 10 [63%]; follow-up telephone call: not implemented = 2 [13%] vs implemented for ≥ 75% of patients with HF on all services = 6 [38%]).
Intervention structure--personnel and processes/content
Multidisciplinary rounds team composition varied across hospitals (see Supplemental Digital Appendix 2 at [LWW INSERT LINK]). The most common team members were cardiologists (n = 15, 94%), bedside nurses (n = 14, 88%), pharmacists (n = 13, 81%), and advanced practice nurses (n = 12, 75%); less common team members included physical therapists (n = 5, 31%) and dieticians (4, 25%). Similar variability was seen in the processes/content of post-discharge follow-up telephone calls (see Supplemental Digital Appendix 3 at [LWW INSERT LINK]). For example, more than three-quarters of respondent hospitals (n = 13, 81%) confirmed that patients had follow-up appointments, but fewer than half (n = 6, 38%) routinely confirmed that patients had transportation to reach these appointments.
Discussion
There is concern regarding hospitals' readmission rates, particularly for patients with HF, and teaching hospitals' rates are among the highest. It has been unclear how teaching hospitals are responding to this problem. Our survey data suggest that, despite limited progress in reducing readmission rates,24 teaching hospitals are engaging in a wide range of care transition interventions aimed at reducing readmissions for HF patients. However, there is considerable variability in the number, type, implementation stage, and structure of these interventions. Future studies to understand the effects of care transition interventions on readmission rates must therefore consider not only which interventions are in place, but also how each is delivered.
Although multiple patient-related factors have been found to predict hospital readmission,25 several systematic reviews have been unable to consistently identify specific interventions that may reduce readmissions.11,26,27 For example, Hansen et al's systematic review highlighted three care transition domains (predischarge, bridging, and post-discharge) and 12 intervention categories, but concluded that no single intervention consistently reduced readmission risk.8 Kociol et al employed a similar framework in their survey of institutions participating in the Get with the Guidelines–Heart Failure program.28 Their study demonstrated variability across sites in the implementation of more than 19 interventions. Less clear in that study was the variability in implementation stage and in intervention structure at the participating teaching hospitals. Similar to Kociol et al, we found variability in the number and types of care transition interventions for HF patients in our sample of teaching hospitals. The variability identified in both of these survey studies may have resulted from the combination of pressure to reduce readmissions and limited high-quality evidence regarding how to do so.29 Without clear evidence, leaders may be influenced by local experience and expertise, intervention costs, and a “hunch” that a specific intervention should work.
Our data suggest that teaching hospitals are devoting attention to improving care transitions for HF patients, despite the absence of consistent evidence of benefit. For example, we found that the post-discharge follow-up telephone call was at some stage of implementation at most sites (88%). A systematic review, however, could not draw firm conclusions about the efficacy of such calls.30 The review's authors did note heterogeneity in how telephone follow-up calls were performed and felt this contributed to the mixed results. Heterogeneity was similarly apparent across our respondent hospitals. For instance, although most of the hospitals utilized post-discharge telephone calls, the processes/content of the calls varied and only 44% provided this intervention to ≥75% of HF patients on the cardiology services or on all services. Although the term “follow-up telephone call” appears straightforward, the way in which the call is delivered can affect outcomes.31–33 This example highlights a challenge that hospital leaders face when deciding where to focus limited resources. Future comparative effectiveness research must consider important implementation issues, including the “who” and “how” of interventions.32 In addition, enhanced descriptions of intervention structure should be provided to improve interpretation of outcomes and guide clinical leaders in designing interventions.
The variability in intervention types, implementation stages, and intervention structures across our respondent hospitals shows that teaching hospitals are attempting to improve care transitions for HF patients in many ways. Without direct comparisons, we cannot state if teaching hospitals are more or less engaged than non-teaching hospitals in efforts to reduce readmissions. However, the large number of interventions that are being implemented at multiple hospitals indicates there are opportunities for teaching hospitals to collaborate as learning organizations.34 By working together, teaching hospitals could provide multi-center data needed to further the understanding of how to improve care transitions and reduce readmissions. Without multi-center data, it is difficult for policymakers and hospitals to target resources appropriately toward reducing readmissions. Poor allocation of resources, in turn, may have unintended consequences, such as the delivery of unnecessary interventions that may provide no benefit, cause harm, or divert resources away from other quality and safety efforts.35
There is reason to believe collaborations aimed at reducing readmissions could be effective. Hospitals have collaborated successfully on projects unrelated to readmissions. For example, 27 neonatal intensive care units participated in a clinical trial, conducted by the Vermont Oxford Network, which showed improved outcomes with early use of continuous positive airway pressure.36 Similar collaborations could test interventions aimed at reducing readmissions, and some are in their beginning stages.37,38 These efforts could advance the science of care transitions while improving patient outcomes. Furthermore, collaborations could improve benchmarking of readmission rates across sites and improve understanding of acceptable targets for readmissions.
Moving forward, hospitals should not only collaborate in the design and implementation of interventions, but they should also coordinate their outcome definitions, with a focus toward preventable readmissions. Currently, most outcomes examine all-cause 30-day readmissions, whereas only a subset of readmissions are preventable and amenable to interventions.39 Without clear preventability definitions, readmission reduction targets for inteventions may remain clouded.39 In addition, supplementary outcomes need to be considered. Unchanged all-cause readmission rates may not always reflect intervention failure, especially among hospitals that have implemented interventions that may reduce preventable readmissions, reduce mortality rates, or improve patient quality of life measures.40
There are a number of limitations of this work that deserve consideration. First, we surveyed an established working group; our sample of U.S. teaching hospitals was not randomly selected. Therefore, our sample does not represent the entire population of teaching hospitals and may be biased toward those with greater interest in care transitions. It is also important to note that survey responses depend upon the knowledge, experience, and perceptions of respondents and do not provide validated measures of the presence or absence of interventions at respondent institutions. There is potential for misclassification of intervention types or implementation stages; however, we do not believe the bias would be in a specific direction. Another limitation is that our survey was not inclusive of all interventions aimed at reducing readmissions for HF patients, including additional HF-specific interventions (e.g., specific dietary guidance) or organization-level interventions (e.g., use of prediction tools to identify high-risk patients, development of improved provider networks across the care continuum) that do not fit into the taxonomy described by Hansen et al.8 Despite this, our survey included a broad set of measures, informed by the literature and experts in care transitions, that help demonstrate the variability of interventions across teaching hospitals. Finally, a larger sample of teaching hospitals would be more suitable for drawing inferences about interventions and readmission outcomes.
Conclusions
The pressure to reduce readmissions among HF patients has recently increased, culminating in the initiation of financial penalties for excessive readmission rates.7 Not surprisingly, hospital administrators and clinical leaders have ranked the reduction of 30-day readmissions as a top priority.41 The priority placed on this goal is exemplified by the large number of HF-specific and care transition interventions being implemented in teaching hospitals. The variability we identified in the number, types, implementation stage, and structure of care transition interventions shows the need for collaborative efforts that will advance our understanding of the best practices for care transitions. Teaching hospitals' continued movement toward a learning organization model36–38 may help improve our understanding of the efficacy of such interventions as well as improve and reduce unnecessary variation in care transitions through the sharing and implementation of best practices.
Supplementary Material
Acknowledgments
The authors would like to acknowledge Meaghan Quinn for her administrative and organizational assistance for the Variations Collaborative Study Group and Anne Axon for her review of an earlier version of the paper.
Funding/Support: Funding for E.E. Vasilevskis was provided by the National Institutes of Health (K23 AG040157) and the Tennessee Valley Geriatric Research, Education and Clinical Center (GRECC). The Variations Collaborative Study Group additionally received support from the Robert Wood Johnson Foundation (RWJF 67627).
Other disclosures: The Variations Collaborative Study Group was organized by the Association of American Medical Colleges, which had no influence on the methodology, findings, or interpretation of the data.
Footnotes
Ethical approval: This study was approved by the Vanderbilt University Institutional Review board (IRB # 110180, March 3, 2011).
Disclaimer: The views expressed in this article are those of the authors and do not necessarily represent the views of the National Institutes of Health or the U.S. Department of Veterans Affairs.
Supplemental digital content for this article is available at [LWW INSERT LINK].
Contributor Information
Eduard E. Vasilevskis, Section of Hospital Medicine, Division of General Internal Medicine and Public Health, Department of Medicine, Vanderbilt University, and a staff physician, Geriatric Research, Education and Clinical Center (GRECC), VA Tennessee Valley Health Care System, Nashville, Tennessee.
Sunil Kripalani, Center for Clinical Quality and Implementation Research, Section of Hospital Medicine, Division of General Internal Medicine and Public Health, Department of Medicine, Vanderbilt University, Nashville, Tennessee.
Michael K. Ong, Department of Medicine, University of California, Los Angeles, Los Angeles, California.
J. Thomas Rosenthal, University of California, Los Angeles Health System, Los Angeles, California.
David E. Longnecker, University of Pennsylvania, Philadelphia, Pennsylvania, and executive director, Coalition to Transform Advanced Care, Washington, D.C.
Brian Harmon, Children's Hospital and Clinics of Minnesota, Minneapolis, Minnesota.
Samuel F. Hohmann, University HealthSystem Consortium, Chicago, Illinois.
Kelly Wright, Section of Hospital Medicine, Division of General Internal Medicine and Public Health, Department of Medicine, Vanderbilt University, Nashville, Tennessee.
Jeanne T. Black, Health Policy Research, Cedars-Sinai Medical Center, Los Angeles, California.
References
- 1.Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. doi: 10.1056/NEJMsa0803563. [DOI] [PubMed] [Google Scholar]
- 2.Vashi AA, Fox JP, Carr BG, et al. Use of hospital-based acute care among patients recently discharged from the hospital. JAMA. 2013;309(4):364–371. doi: 10.1001/jama.2012.216219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bratzler DW, Normand SLT, Wang Y, et al. An administrative claims model for profiling hospital 30-day mortality rates for pneumonia patients. PLoS ONE. 2011;6(4):e17401. doi: 10.1371/journal.pone.0017401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Keenan PS, Normand SL, Lin Z, et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1(1):29–37. doi: 10.1161/CIRCOUTCOMES.108.802686. [DOI] [PubMed] [Google Scholar]
- 5.Krumholz HM, Brindis RG, Brush JE, et al. Standards for statistical models used for public reporting of health outcomes. Circulation. 2006;113(3):456–462. doi: 10.1161/CIRCULATIONAHA.105.170769. [DOI] [PubMed] [Google Scholar]
- 6.Joynt KE, Jha AK. Characteristics of hospitals receiving penalties under the Hospital Readmissions Reduction Program. JAMA. 2013;309(4):342–343. doi: 10.1001/jama.2012.94856. [DOI] [PubMed] [Google Scholar]
- 7.Patient Protection and Affordable Care Act of 2010. Pub L No. 111-148, 124 Stat 408, S3025. Hospital Readmissions Reduction Program. 2010 [Google Scholar]
- 8.Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med. 2011;155(8):520–528. doi: 10.7326/0003-4819-155-8-201110180-00008. [DOI] [PubMed] [Google Scholar]
- 9.Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303(17):1716–1722. doi: 10.1001/jama.2010.533. [DOI] [PubMed] [Google Scholar]
- 10.Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure. N Engl J Med. 2010;363(24):2301–2309. doi: 10.1056/NEJMoa1010029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rennke S, Nguyen OK, Shoeb MH, Magan Y, Wachter RM, Ranji SR. Hospital-initiated transitional care interventions as a patient safety strategy: A systematic review. Ann Intern Med. 2013;158:433–440. doi: 10.7326/0003-4819-158-5-201303051-00011. [DOI] [PubMed] [Google Scholar]
- 12.Stephanie Rennke, Kesh S, Neeman N, Sehgal NL. Complementary telephone strategies to improve postdischarge communication. Am J Med. 2012;125(1):28–30. doi: 10.1016/j.amjmed.2011.05.011. [DOI] [PubMed] [Google Scholar]
- 13.Kripalani S, Theobald CN, Anctil B, Vasilevskis EE. Reducing hospital readmission rates: Current strategies and future directions. Annual Review of Medicine. 2014;65(1):471–485. doi: 10.1146/annurev-med-022613-090415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wennberg JE. Unwarranted variations in healthcare delivery: Implications for academic medical centres. BMJ. 2002;325(7370):961–964. doi: 10.1136/bmj.325.7370.961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bradley EH, Curry L, Horwitz LI, et al. Contemporary evidence about hospital strategies for reducing 30-day readmissions: A national study. J Am Coll Cardiol. 2012;60(7):607–614. doi: 10.1016/j.jacc.2012.03.067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6(4):444–450. doi: 10.1161/CIRCOUTCOMES.111.000101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kashiwagi DT, Burton MC, Kirkland LL, Cha S, Varkey P. Do timely outpatient follow-up visits decrease hospital readmission rates? Am J Med Qual. 2011;27(1):11–15. doi: 10.1177/1062860611409197. [DOI] [PubMed] [Google Scholar]
- 18.Coleman EA, Parry C, Chalmers S, Min S. The Care Transitions Intervention: Results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828. doi: 10.1001/archinte.166.17.1822. [DOI] [PubMed] [Google Scholar]
- 19.McAlister FA, Stewart S, Ferrua S, McMurray JJJV. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: Systematic review of randomized trials. J Am Coll Cardiol. 2004;44(4):810–819. doi: 10.1016/j.jacc.2004.05.055. [DOI] [PubMed] [Google Scholar]
- 20.Phillips CO, W S. Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: A meta-analysis. JAMA. 2004;291(11):1358–1367. doi: 10.1001/jama.291.11.1358. [DOI] [PubMed] [Google Scholar]
- 21.Adler ED, Goldfinger JZ, Kalman J, Park ME, Meier DE. Palliative care in the treatment of advanced heart failure. Circulation. 2009;120(25):2597–2606. doi: 10.1161/CIRCULATIONAHA.109.869123. [DOI] [PubMed] [Google Scholar]
- 22.Bakitas M, MacMartin M, Trzepkowski K, et al. Palliative care consultations for heart failure patients: How many, when, and why? J Card Care. 2013;19(3):193–201. doi: 10.1016/j.cardfail.2013.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.University HealthSystem Consortium. Clinical Data Base/Resource Manager (CDB/RM) [Accessed September 16, 2015];2015 https://www.uhc.edu/performance-intelligence.
- 24.Dartmouth Atlas Project, PerryUndem Research & Communications. The Revolving Door: A Report on U.S Hospital Readmissions. Robert Wood Johnson Foundation. [Accessed August 27, 2015];2013 Feb; http://www.rwjf.org/en/research-publications/find-rwjf-research/2013/02/the-revolving-door--a-report-on-u-s--hospital-readmissions.html.
- 25.Kansagara D, Englander H, Salanitro A, et al. Risk prediction models for hospital readmission: A systematic review. JAMA. 2011;306(15):1688–1698. doi: 10.1001/jama.2011.1515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hesselink G, Schoonhoven L, Barach P, et al. Improving patient handovers from hospital to primary care: A systematic review. Ann Intern Med. 2012;157(6):417–428. doi: 10.7326/0003-4819-157-6-201209180-00006. [DOI] [PubMed] [Google Scholar]
- 27.Leppin AL, Gionfriddo MR, Kessler M, et al. Preventing 30-day hospital readmissions: A systematic review and meta-analysis of randomized trials. JAMA Intern Med. 2014;174(7):1095–1107. doi: 10.1001/jamainternmed.2014.1608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kociol RD, Peterson ED, Hammill BG, et al. National survey of hospital strategies to reduce heart failure readmissions: Findings from the Get with the Guidelines-Heart Failure Registry. Circ Heart Fail. 2012;5:680–687. doi: 10.1161/CIRCHEARTFAILURE.112.967406. [DOI] [PubMed] [Google Scholar]
- 29.Burke RE, Kripalani S, Vasilevskis EE, Schnipper JL. Moving beyond readmission penalties: Creating an ideal process to improve transitional care. J Hosp Med. 2012;8:102–109. doi: 10.1002/jhm.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for postdischarge problems in patients discharged from hospital to home. Cochrane Database of Systematic Reviews. 2006;4:CD004510. doi: 10.1002/14651858.CD004510.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ovretveit JC, Shekelle PG, Dy SM, et al. How does context affect interventions to improve patient safety? An assessment of evidence from studies of five patient safety practices and proposals for research. BMJ Qual Saf. 2011 doi: 10.1136/bmjqs.2010.047035. [DOI] [PubMed] [Google Scholar]
- 32.Hulscher MEJL, Schouten LMT, Grol RPTM, Buchan H. Determinants of success of quality improvement collaboratives: What does the literature show? BMJ Qual Saf. 2013;22(1):19–31. doi: 10.1136/bmjqs-2011-000651. [DOI] [PubMed] [Google Scholar]
- 33.Hulscher MEJL, Laurant MGH, Grol RPTM. Process evaluation on quality improvement interventions. Qual Saf Health Care. 2003;12(1):40–46. doi: 10.1136/qhc.12.1.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Carroll JS, Edmondson AC. Leading organisational learning in health care. Qual Saf Health Care. 2002;11(1):51–56. doi: 10.1136/qhc.11.1.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Joynt KE, Jha AK. Thirty-day readmissions — Truth and consequences. N Engl J Med. 2012;366(15):1366–1369. doi: 10.1056/NEJMp1201598. [DOI] [PubMed] [Google Scholar]
- 36.Dunn MS, Kaempf J, Klerk A de, et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics. 2011;128(5):e1069–e1076. doi: 10.1542/peds.2010-3848. [DOI] [PubMed] [Google Scholar]
- 37.Auerbach AD, Patel MS, Metlay JP, et al. The Hospital Medicine Reengineering Network (HOMERuN): A learning organization focused on improving hospital care. Acad Med. 2013;89(3):415–420. doi: 10.1097/ACM.0000000000000139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Centers for Medicare & Medicaid Services. The partnership for patients. [Accessed August 27, 2015]; http://partnershipforpatients.cms.gov/
- 39.Lavenberg JG, Leas B, Umscheid CA, Williams K, Goldmann DR, Kripalani S. Assessing preventability in the quest to reduce hospital readmissions: hospital readmissions and preventability. J Hosp Med. 2014;9(9):598–603. doi: 10.1002/jhm.2226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med. 2010;363(3):297–298. doi: 10.1056/NEJMc1001882. [DOI] [PubMed] [Google Scholar]
- 41.Ahmad FS, Metlay JP, Barg FK, Henderson RR, Werner RM. Identifying hospital organizational strategies to reduce readmissions. Am J Med Qual. 2013;28(4):278–285. doi: 10.1177/1062860612464999. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.