

Abstract
Patterned hair loss is the most common cause of hair loss seen in both the sexes after puberty. Numerous classification systems have been proposed by various researchers for grading purposes. These systems vary from the simpler systems based on recession of the hairline to the more advanced multifactorial systems based on the morphological and dynamic parameters that affect the scalp and the hair itself. Most of these preexisting systems have certain limitations. Currently, the Hamilton-Norwood classification system for males and the Ludwig system for females are most commonly used to describe patterns of hair loss. In this article, we review the various classification systems for patterned hair loss in both the sexes. Relevant articles were identified through searches of MEDLINE and EMBASE. Search terms included but were not limited to androgenic alopecia classification, patterned hair loss classification, male pattern baldness classification, and female pattern hair loss classification. Further publications were identified from the reference lists of the reviewed articles.
KEYWORDS: Androgenic alopecia, classification, patterned hair loss
INTRODUCTION
Patterned hair loss is the most common cause of hair loss seen in both the sexes after puberty, typically presenting with progressive thinning, miniaturization, and loss of hair at the affected sites. The hair loss varies in extent and severity and numerous stages exist between the stages of early frontotemporal recession to the stage of residual occipital band. Numerous researchers have proposed different classification systems for patterned hair loss in both males and females based on the evolutionary stage of hair loss ranging from a simple two-stage classification proposed by Beek in 1950 to the recent advanced basic and specific (BASP) classification. In this article, we review the various classification systems for pattern hair loss described in the literature. Relevant articles were identified through searches of MEDLINE and EMBASE. Search terms included but were not limited to androgenic alopecia classification, patterned hair loss classification, male pattern baldness classification, and female pattern hair loss classification. Further publications were identified from the reference lists of the reviewed articles.
CLASSIFICATIONS OF MALE PATTERN HAIR LOSS
Beek (1950)
Beek evaluated 1,000 Caucasian males with patterned hair loss and classified them into two types — frontal baldness and frontovertical baldness, based on the stage of evolution.[1] It was a simple classification, which described only two stages of hair loss and did not take into account the various evolutionary stages but is important as this was the first attempt to classify hair loss.
Hamilton (1951)
Hamilton, an anatomist, studied more than 300 males with hair loss and proposed a detailed classification system based on frontoparietal and frontal recessions and frontal thinning, which consisted of eight evolutionary aspects and three subgroups [Figure 1]. The various categories of hair loss described by Hamilton include a) scalps, which are not bald (Types I-III) and b) scalps, which are bald (Types IV-VIII), which are defined as follows.
Figure 1.
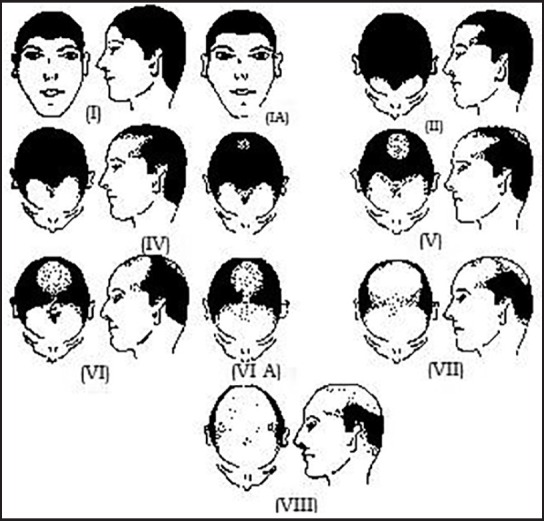
Hamilton classification of male pattern hair loss. Type III has not been included in this figure as a large variety of conditions were included in this type[2]
Type I: There is an absence of bilateral recessions along the anterior border of the hairline in the frontoparietal regions. In this, there is a variant form in which the entire anterior border of the hairline lies high on the forehead, which is referred to as Type IA.
Type II: The anterior border of the hairline in the frontoparietal regions has triangular areas of recession, which tend to be symmetrica1 and extend no farther posteriorly than a point 3 cm anterior to a line drawn in a coronal plane between the external auditory meatuses. Hair is also lost, or sparse, along the midfrontal border of the scalp but the depth of the affected area is much less than in the frontoparietal regions.
Type III: Borderline cases were listed separately as Type III, which also included scalps in which classification is rendered inaccurate due to scars, lateral asymmetry in denudation, unusual types of sparseness and thinning of the hair, and other factors.
Type IV: It represents the minimal hair loss considered sufficient to represent baldness. There are deep frontotemporal recessions, usually symmetrical, and are either bare or very sparsely covered by hair. These recessions extend farther posteriorly than a point, which lies 3 cm anterior to a coronal line drawn between the external auditory meatuses. If hair is sparse or lacking as a broad band along the entire anterior border of the hairline, it is classified as Type IVA.
Type V: It includes extensive frontoparietal and frontal recessions with a sparseness or absence of hair on the crown.
Type VI: In this type, the tonsural region of alopecia remains separated from more anteriorly located areas of denudation by a laterally-directed bar of scalp in which the hair is only slightly sparse. An island of hair lies in the midline anterior to this laterally-directed hairy bridge. In the variant pattern, Type VIA, the peninsula or island of mid-frontal hair is sparse or lost.
Type VII and VIII: In these types, the horseshoe-shaped area of sparse hair or of denudation is unbroken by any well-haired, laterally-directed bridge of scalp. These are a result of the spread and confluence of the tonsural and the anteriorly located regions of alopecia.[2]
Hamilton classification set a benchmark for future classifications of male patterned hair loss as it had elaborately described the various evolutionary stages of hair loss and had based the classification on them but it did not describe a few rare patterns of hair loss, which were later on added by Norwood to give the commonly used Hamilton-Norwood classification.
Ogata (1953)
Ogata distinguished 15 different subtypes of patterned hair loss and classified them into six different subtypes based on the study of Japanese men. The first column shows a normal hairline for Japanese men according to Ogata. The second, third, and fourth columns represent early, intermediate, and late stages of patterned baldness, respectively [Figure 2]. The classification system is somewhat different from the classification systems produced based on Caucasian men, suggesting that the development of patterned baldness in Japanese men may be distinct from Caucasians.[3]
Figure 2.

Ogata classification of patterned hair loss[3]
Setty (1970)
Hamilton classification was based on the study of mostly white males with hair loss. Setty studied 300 white and 300 black males and gave a different classification in which he simplified Hamilton's classification into three different subtypes keeping into account the patterns of hair loss in Blacks as well. The classification system proposed by Setty is as follows:
Totopilosis (corresponding to Hamilton Type I): The entire scalp is covered with hair. Temporal and frontal indentations are approximately equal at the greatest length from the anterior end to posterior end and the anterior hair margin of the scalp forms a serpentine or zigzag line that extends obliquely forward across the side of the head.
Indentato-pilosis (Hamilton Types II-IV): Frontal indentation is longer than temporal indentation at the greatest length from the anterior end to the posterior end. Hairs in midline of the scalp begin at a point as far anteriorly or not as far anteriorly as that in totopilose pattern.
-
Indentato-circulo-pilosis (Hamilton Types VI-VII) — Almost same as the indentato-pilose pattern with a circular arrangement of hair around the vertex of the head. Area void of hair on the vertex is at least approximately 2.54 cm in diameter. Hair in the midline of the head begins at a point not as far anteriorly as that in the totopilose pattern. There are two varieties of indentato-circulo-pilose pattern:
- “confluent” characterized by the frontal indentation of baldness being separated from the apical area of baldness by a strip of hair that connects the medial hair and lateral hair
- “nonconfluent” characterized by a bare strip of at least 2.54 cm width connecting the frontal bald area and the apical area.
The indentato-pilose pattern had the highest incidence in both White males and Negro males, and the totopilose was over four times more common in the Negroes than in the Whites.[4]
Setty's classification was an improvement over Hamilton's classification as it incorporated the patterns of hair loss in Black males also but it lacked the detailed staging of the evolution of hair loss, so it failed to find much favor with the clinicians.
Norwood (1975)
Dr. O’Tar Norwood, a dermatologist and hair transplant surgeon, revised Hamilton's classification in 1975 after studying patterned hair loss in 1,000 males. The Norwood classification is the most widely used classification for hair loss in men and it defines two major patterns and several less common types. Norwood observed that thinning starts in the temples as well as the crown/vertex and slowly progresses to encompass the entire top of the scalp, and so he based his classification on this pattern [Figure 3]. The various grades of hair loss described by Norwood include the following.
Figure 3.

Norwood's classification of patterned hair loss in males[5]
Type I: There is minimal or no recession of the hairline.
Type II: There are triangular, usually symmetrical, areas of recession at the frontotemporal hairline.
Type III: This represents the minimal extent of hair loss sufficient to be considered as baldness according to Norwood. There are deep symmetrical recession at the temples that are bare or only sparsely covered by hair. In Type III vertex, the hair loss is primarily from the vertex with limited recession of the frontotemporal hairline that does not exceed the degree of recession seen in Type III.
Type IV: The frontotemporal recession is more severe than in Type III and there is sparse hair or no hair on the vertex. The two areas of hair loss are separated by a band of moderately dense hair that extends across the top. This band connects with the fully haired fringe on the sides of the scalp.
Type V: The vertex hair loss region is still separated from the frontotemporal region but it is less distinct. The band of hair across the crown is narrower and sparser and the vertex and frontotemporal regions of hair loss are bigger.
Type VI: The bridge of hair that crosses the crown is gone with only sparse hair remaining. The frontotemporal and vertex regions are joined together and the extent of hair loss is greater.
Type VII: The most severe form of hair loss and only a narrow band of hair in a horseshoe shape remains on the sides and back of the scalp. This hair is usually not dense and may be quite fine.
Norwood also defined a Type A variant from his standard classification system, which is distinguished by two major features and two minor features.
The major features are: 1) the anterior border of the hairline progresses to the rear without leaving an island of hair in the mid-frontal region and 2) there is no simultaneous development of a bald area on the vertex. Instead, the frontal hairline recession keeps progressing to the rear of the scalp.
The minor features are: 1) there is a persistent sparse hair scattering in the area of hair loss and 2) the horseshoe-shaped fringe areas of hair that remain on the side and back of the scalp tend to be wider and reach higher on the head compared to Norwood's standard. The various Type A variants described by Norwood are as follows:
Type IIA: The hairline is anterior to the coronal plane 2 cm anterior to the external auditory meatus.
Type IIIA: The hairline has receded back to a point between the limit of Type IIA and the level of the external auditory meatus.
Type IVA: The hairline has receded beyond the external auditory meatus but has not reached the vertex.
Type VA: The area of denudation includes the vertex. Hair loss more severe than Type VA cannot be distinguished from Types VI or VII.[5]
Norwood classification is one of the most detailed classification systems for male patterned hair loss and is the most widely used classification worldwide but is too detailed, divided, and complicated to be used for various surgical operations. Moreover, it also does not list some peculiar types of baldness (a balding patch on the vertex or occiput with a preserved anterior hairline) and is not very helpful in determining the surgical method. Numerous researchers proposed newer classification systems keeping the simplicity of classification and surgical aspects of treatment in mind.
Bouhanna (1976)
Based on observations in European Caucasians, Bouhanna designed a much simplified male patterned baldness classification system in 1976, which included just three basic hair loss presentation with two variants as follows [Figure 4]:
Figure 4.

Bouhanna classification of hair loss among European Caucasians[6]
Stage 1
Type a: Symmetric recession of the frontal margin forming two temporal areas of recession of varying depth
Type b: Sparseness at the cranial summit or vertex
Stage 2
Type a: Uniform recession of the frontal margin as far as the cranial summit
Type b: With associated vertex
Stage 3
The ultimate stage of alopecia, with only a remnant temporo-occipital crown.[6]
Bouhanna's classification was a simplified classification system based on the extent of hair loss and allowed a precise evaluation of surgical indication of hair transplantation but was not helpful in deciding the type of surgical procedure required, which was later addressed by Bouhanna himself in a multifactorial classification.
Blanchard and Blanchard (1984)
Blanchard proposed a different classification with six evolutional stages determined by six measurements: glabello-frontal, superciliary frontal, interparietal, fronto-vertical, helicon-vertical, and nucho-vertical distances [Figure 5].[7] This classification system is not so commonly used as it was difficult to apply and required taking multiple measurements in every patient for classification purpose, which is a tedious task.
Figure 5.

Blanchard's evolutionary staging of hair loss[7]
Dynamic classification of Dardour and Bouhanna (1996)
They proposed a classification system, which included all the parameters, both morphological and dynamic, that affect the scalp and the hair itself. This classification includes for each heading a symbol followed by a number, which indicates its situation. The various parameters included in this system include the stage of hair loss, density of hair, laxity of the scalp, aspect of hair, color and thickness of hair, and rate of hair growth.[8] This classification was more detailed than the previously described systems and it took into account various parameters, which were not considered by Hamilton such as the covering power of hair, density in each region, and rate of growth of hair but it was too complicated and difficult to apply in routine practice as it involved a large number of measurements and parameters.
Koo (2000)
As the Norwood classification method is too detailed and complicated to be used for various surgical operations and also does not list some peculiar types of baldness, it is not very helpful in determining the surgical procedures. Koo et al. studied more than 1,700 Korean males with patterned hair loss and proposed a new simpler classification method. In this classification, the male patterned baldness is classified into six subtypes by the English alphabetical letter shape of the bald area [Figure 6]. The various subtypes in this classification include the following
Figure 6.
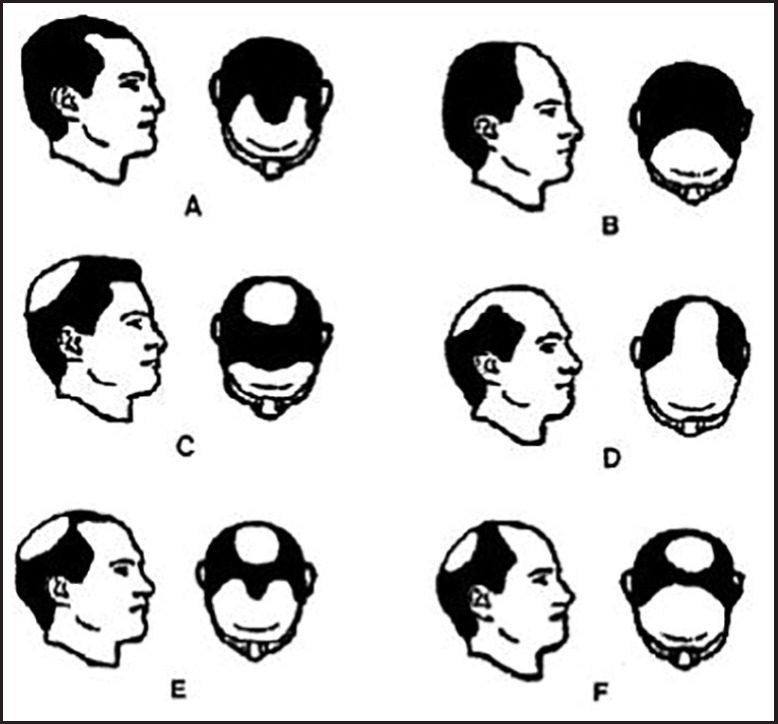
Koo's classification of male pattern baldness. (a) M type (b) C type (c) O type (d) U type (e) MO type (f) CO type[9]
Type M: When both sides of the frontotemporal hairlines look triangular or like the letter M
Type C: When the anterior hairline looks like a half-circle or the letter C. M and C types of male pattern baldness do not have hair loss on the vertex.
Type O: When there is a round or ovoid bald patch on the vertex or occiput while the anterior hairline is well-preserved
Type U: When the recession of the anterior hairline progresses over the vertex, which looks like a horseshoe or the letter U.
Types MO and CO: When recession of the frontotemporal hairline exists, with a bald patch on the vertex, as combined patterns, these are types MO and CO, according to the shape of the recession of the anterior hairline[9]
This classification system has advantages over the previous classification as it is simpler, easy to apply, does not require complex measurements, and is useful in planning surgery.
CLASSIFICATIONS OF FEMALE PATTERN HAIR LOSS
Ludwig (1977)
Ludwig observed 468 females with hair loss and proposed a classification based on the stage of evolution [Figure 7]. The classification consisted of three grades of hair loss, which include:
Figure 7.

Ludwig's classification of hair loss among females[10]
Grade I: Perceptible thinning of the hair on the crown, limited in the front by a line situated 1-3 cm behind the frontal hairline
Grade II: Pronounced rarefaction of the hair on the crown within the area seen in Grade I.
Grade III: Full baldness (total denudation) within the area seen in Grades I and II.[10]
Ludwig emphasized preservation of the frontal fringe despite progressive centrifugal loss over the top of the scalp but did not incorporate the accentuation of frontovertical alopecia, which was later on included by Olsen. Moreover, the females with male patterned hair loss also could not be classified with this system.
Ebling and Rook (1975)
They developed a five-stage classification system for female patterned baldness [Figure 8]. The first two stages are the same as the Ludwig system. Type I shows perceptible thinning of the hair on the crown. Type II shows pronounced rarefaction of the hair on the crown within the area seen in Type I. Type III shows continued diffuse hair loss in the region defined in Types I and II but also the initial loss of hair from the frontotemporal hair line. Type IV shows a continuation of this diffuse loss and frontotemporal recession and in Type V, there is complete loss of hair on the top of the scalp resembling a male pattern of baldness.
Figure 8.

Ebling and Rook five-stage classification of female pattern of hair loss
This classification system was an improvement over the Ludwig classification as unlike the three-stage Ludwig classification, Ebling and Rook took into account that women could have both a diffuse form of alopecia and also a male pattern with recession of the frontotemporal hair line, which was not described by Ludwig.
Savin (1992)
Savin came up with nine computer images, which are now typically referred to as the Savin scale, as a pictorial classification scale to quantify patterned hair loss clinically in women which into eight stages of increasing crown balding, in addition to a special subcategory to detect frontal anterior recession [Figure 9]. These staged illustrations provided a finer visual gradient of hair loss pattern and density than the previous classification scale for women with pattern baldness. Savin scale is a useful tool for assessing degrees of hair loss in women, which is fairly consistent with different investigators using the same scale, which adds degrees of hair loss that were missing in the Ludwig grading but this system also did not address the progressive frontal hair loss (Christmas tree pattern).[11]
Figure 9.

Savin's pictorial grading of female pattern hair loss[11]
Olsen (1994)
Olsen proposed a classification, which was similar to Ludwig classification but incorporated the accentuation of frontovertical alopecia, which has a triangular or “Christmas tree” pattern. Olsen observed that hair loss in women may occur in a subtle pattern of loss that is only apparent when one performs a midline part where there is often a progressive decrease in hair density from the vertex to the front of the scalp, which he described as a “Christmas tree” distribution of loss. This pattern is visible both in the early as well as advanced stages of hair loss.[12]
Sinclair (2004)
It is a self-report photographic measure of patients’ perceptions of the severity of their hair loss, which comprises five color photographs of women's scalps with the hair parted centrally. The first photograph is of a normal scalp and the photographs 2-5 are of scalps of women with increasingly severe hair loss [Figure 10]. The photographs are numbered from 1 to 5 and respondents are required to circle the number of the photograph that they feel most closely resembles the appearance of their own hair when parted in the center. Women with stages 1 and 2 hair loss tend to present with either episodic or continuous increased hair shedding with a reduction in the volume of the hair when held in a ponytail. Women with stages 3, 4, and 5 hair loss may present with either loss of volume of hair over the scalp with widening of the central part, episodic increased hair shedding, or continuous hair shedding.[13]
Figure 10.
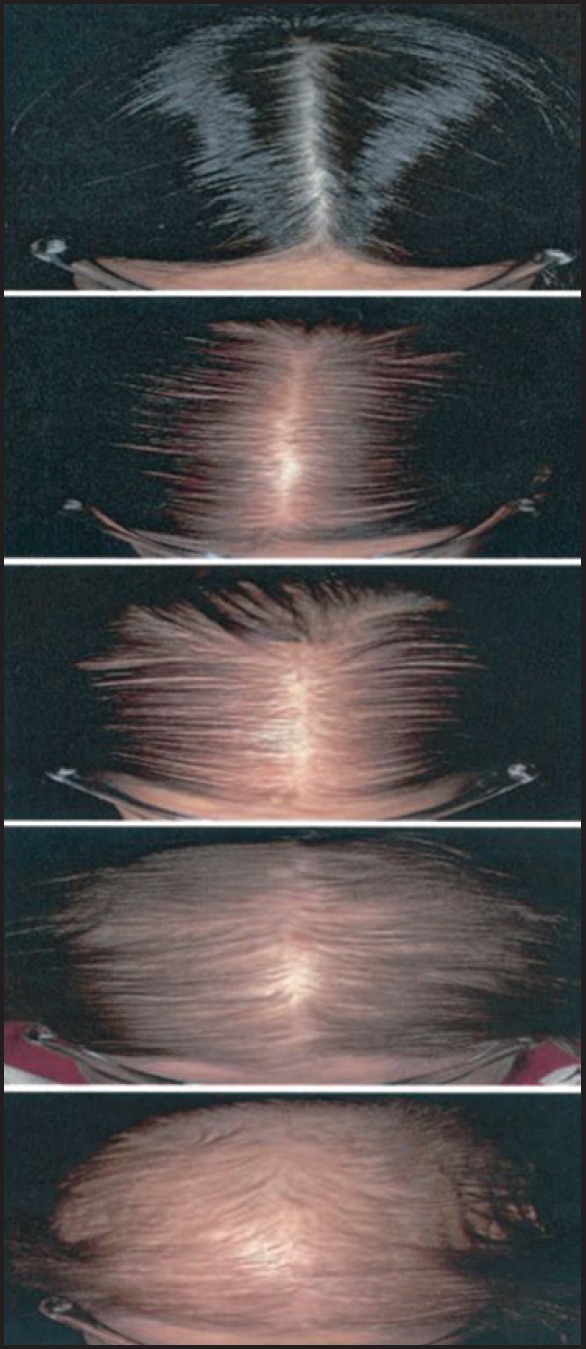
Sinclair's self-reporting photographic measure of female pattern of hair loss[13]
Sinclair grading is a simple grading system and can be used with ease both by the clinicians and patients alike for defining the extent of hair loss and for assessing the response to treatment.
CLASSIFICATION IRRESPECTIVE OF SEX
Bouhanna (2000)
Bouhanna proposed a multifactorial classification for both male and female patterned hair loss, integrating several parameters, which included extension of bald and hair-bearing areas, elasticity and density of scalp, and hair characteristics such as diameter, length, shape, and color, which contribute to the covering power of the hair. This classification has proved useful in assessing the changes in hair parameters during the course of medical treatment and also in deciding the indication of hair transplantation for the surgical management.[14]
This classification system is a detailed classification system taking into consideration different parameters, which could be quantified and computerized but the inclusion of numerous parameters and measurements also makes it time-consuming and difficult to apply in routine practice.
Basic and specific classification (2007)
The BASP classification is a novel stepwise and universal classification system for patterned hair loss regardless of sex, which is based on observed patterns of hair loss including the shape of the anterior hairline and the density of hair on the frontal and vertex areas. Lee et al. evaluated more than 2,200 subjects with patterned this classification system, which consists of the basic type and the specific type. The basic (BA) type represents the shape of the anterior hairline, and the specific type (SP) represents the density of hair on distinct areas (frontal and vertex). There are four basic types (L, M, C, and U) and two specific types (F and V) and each of the various types is subdivided into 3 or 4 grades (subtypes) according to its severity [Figure 11]. The final type is decided by the combination of the determined basic and specific types. The various types of hair loss according to BASP classification include the following:
Figure 11.
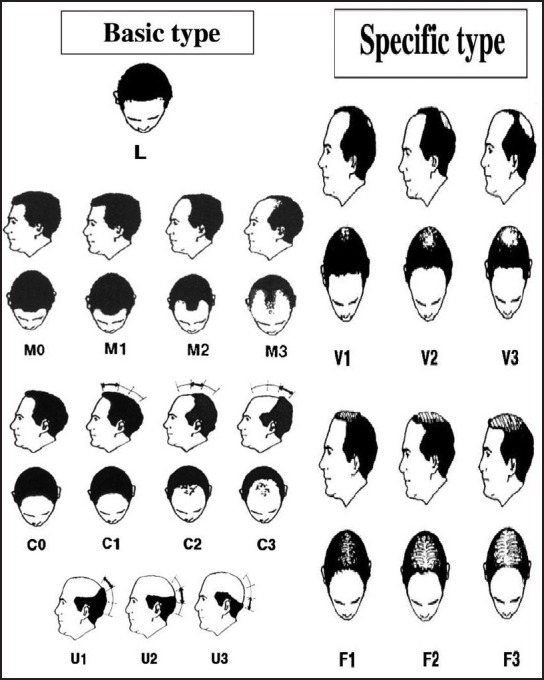
Basic and specific (BASP) classification of hair loss[15]
a. Basic types
Type L: No recession is observed along the anterior border in the frontotemporal region resembling a linear line and usually means that there is no hair loss.
Type M: Recession in the frontotemporal hairline is more prominent than the mid-anterior hairline and the hairline resembles the letter M. It is further divided into four subtypes depending on the severity of baldness.
Type M0: The original hairline is preserved and no hair loss has occurred.
Type M1: Frontotemporal recession extends posteriorly but not beyond the anterior third of a virtual line connecting the original hairline and the top of the vertex.
Type M2: Frontotemporal recession extends further posteriorly but not beyond the middle third of a virtual line connecting the original hairline and the top of the vertex.
Type M3 - Frontotemporal recession extends beyond the middle third section into the posterior third of the area of a virtual line connecting the original hairline and the top of the vertex.
Type C: Recession in the mid-anterior hairline is more prominent than the frontotemporal hairline. The entire anterior hairline regresses posteriorly in the shape of half-circle, resembling the letter C. It is further divided into four subtypes depending on the severity.
Type C0: The original anterior hairline is preserved and no hair loss is visible.
Type C1: The mid-anterior hairline recedes to the anterior one-third of the virtual line connecting the original hairline and the top of the vertex.
Type C2: The mid-anterior hairline recedes to the middle one-third of the virtual line.
Type C3: The mid-anterior hairline recedes to the posterior one-third of the virtual line.
Type U: The anterior hairline recedes posteriorly beyond the vertex forming a horseshoe shape resembling the letter U. It is the most severe type of hair loss. It is further divided into three subtypes depending on the severity of baldness.
Type U1: The anterior hairline recedes to lie within the superior one-third of the virtual line connecting vertex and the posterior occipital protuberance.
Type U2: The anterior hairline recedes to lie within the middle one-third of the virtual line connecting the vertex and the posterior occipital protuberance.
Type U3: The anterior hairline recedes to lie within the inferior one-third of the virtual line connecting the vertex and the posterior occipital protuberance.
b. Specific types
Type F: It represents a general decrease in the density of hair over the entire top of the scalp regardless of the anterior hairline and is usually more marked over the frontal area of the scalp.
Type F1: Thinning of the hair on the crown is perceptible (mild change).
Type F2: Thinning of the hair on the crown is pronounced (moderate change).
Type F3: The hair on the crown is very sparse or absent (severe change).
Type V: The hair around the vertex is notably sparser and hair loss is seen more distinctly in the vertex than in the frontal area.
Type V1: Thinning of the hair around the vertex is perceptible (mild change).
Type V2: Thinning of the hair around the vertex is pronounced (moderate change).
Type V3: Thinning of the hair around the vertex is very sparse or absent (severe change).
The final type is decided by a combination of the basic and specific type. e.g., basic type (C1) + specific type (V1) denotes final type C1V1.[15]
This classification system offers numerous advantages over the preexisting systems as it is more comprehensive and systematic and can be used irrespective of the gender. Moreover, this system is easy to memorize and practice and has better reproducibility and repeatability than the previous classifications in routine clinical practice.[16]
Practical applications of classification systems:
These classification systems, especially the common ones such as the Norwood-Hamilton and Ludwig system have been widely used by patients and practitioners for determining the stage of hair loss and assessing the response to therapy. Apart from these, a few classification systems have been helpful in determining the surgical procedure for hair loss management. Few authors have described indications for different surgical techniques depending on the stage of hair loss. Bouhanna[6] devised the following operative indications based on his own classification system.
Stage 1A: For restoration of original frontal line, two small preauricular flaps are used if the laxity of donor site is adequate or two strip grafts are combined with minigraft transplantation if the laxity is inadequate.
Stage 1B: If vertex laxity is adequate, scalp reduction with minigraft transplantation is arranged in a spiral or transposition of one or two flaps with excision of residual bald zones. If vertex scalp is taut, 300-400 minigrafts are transplanted.
Stage IIA: If laxity is adequate, two preauricular flaps combined with a concave and a straight flap along with 150-200 minigrafts are advised. If laxity is inadequate, 500-800 minigrafts are advised.
Stage IIB and III: If laxity is adequate, the appropriate treatment is transposition of two, three, or four superior pedicled, nonautonomized flaps, along with excision of the bald area or transplantation of minigrafts in the bald areas between the flaps. If laxity is inadequate, placement of two expanders followed by transposition of two flaps is advised.
Koo et al.[9] also devised surgical indications for the various stages of hair loss according to their classification system. For type M, hair transplantation or a preauricular flap can be performed. For types O, MO, and CO, scalp reduction with or without an expander followed by hair transplantation can be performed. For type U, expanded triple advancement transposition or bilateral advancement transposition or scalp reduction are the primary options while hair transplantation remains the secondary option. For type C, scalp advancement after expansion, scalp flap, or hair transplantation can be performed according to the patient's preference.
CONCLUSION
Although a large number of classification systems are available today, all of them have certain limitations as they either do not describe the complete evolutionary stages of hair loss or are too detailed for practical use. Hence, the clinician should assess all of them and choose the classification system as per his/her own convenience and requirement.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Beek CH. A study on extension and distribution of the human body-hair. Dermatologica. 1950;101:317–31. doi: 10.1159/000257143. [DOI] [PubMed] [Google Scholar]
- 2.Hamilton JB. Patterned loss of hair in man: Types and incidence. Ann N Y Acad Sci. 1951;53:708–28. doi: 10.1111/j.1749-6632.1951.tb31971.x. [DOI] [PubMed] [Google Scholar]
- 3.Ogata T. Development of patterned alopecia. Sogo Rinsho. 1953;2:101–6. [Google Scholar]
- 4.Setty LR. Hair patterns of the scalp of white and Negro males. Am J Phys Anthropol. 1970;33:49–56. doi: 10.1002/ajpa.1330330108. [DOI] [PubMed] [Google Scholar]
- 5.Norwood OT. Male pattern baldness: Classification and incidence. South Med J. 1975;68:1359–65. doi: 10.1097/00007611-197511000-00009. [DOI] [PubMed] [Google Scholar]
- 6.Bouhanna P, Nataf J. A propos des transplantations de cuir chevelu. Critiques et propositions. Rev Chir Esthet. 1976;7:17–23. [Google Scholar]
- 7.Blanchard G, Blanchard B. A topographical approach to hair transplantation and scalp reduction. Ann Chir Plast Esthet. 1984;29:152–61. [PubMed] [Google Scholar]
- 8.Bouhanna P, Dardour JC. Male baldness: Dynamic classification of Dardour and Bouhanna. In: Bouhanna P, Dardour JC, editors. Hair Replacement Surgery. Berlin: Springer-Verlag; 1996. pp. 33–4. [Google Scholar]
- 9.Koo SH, Chung HS, Yoon ES, Park SH. A new classification of male pattern baldness and a clinical study of the anterior hairline. Aesthetic Plast Surg. 2000;24:46–51. doi: 10.1007/s002669910009. [DOI] [PubMed] [Google Scholar]
- 10.Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J Dermatol. 1977;97:247–54. doi: 10.1111/j.1365-2133.1977.tb15179.x. [DOI] [PubMed] [Google Scholar]
- 11.Savin RC. A method for visually describing and quantitating hair loss in male pattern baldness. J Invest Dermatol. 1992;98:604. [Google Scholar]
- 12.Olsen EA. Androgenetic alopecia. In: Olsen EA, editor. Disorders of Hair Growth: Diagnosis and Treatment. New York: McGraw-Hill; 1994. pp. 257–83. [Google Scholar]
- 13.Sinclair R, Jolley D, Mallari R, Magee J. The reliability of horizontally sectioned scalp biopsies in the diagnosis of chronic diffuse telogen hair loss in women. J Am Acad Dermatol. 2004;51:189–99. doi: 10.1016/s0190-9622(03)00045-8. [DOI] [PubMed] [Google Scholar]
- 14.Bouhanna P. Multifactorial classification of male and female androgenetic alopecia. Dermatol Surg. 2000;26:555–61. doi: 10.1046/j.1524-4725.2000.00009.x. [DOI] [PubMed] [Google Scholar]
- 15.Lee WS, Ro BI, Hong SP, Bak H, Sim WY, Kim do W, et al. A new classification of pattern hair loss that is universal for men and women: Basic and specific (BASP) classification. J Am Acad Dermatol. 2007;57:37–46. doi: 10.1016/j.jaad.2006.12.029. [DOI] [PubMed] [Google Scholar]
- 16.Hong H, Ji JH, Lee Y, Kang H, Choi GS, Lee WS. Reliability of the pattern hair loss classifications: A comparison of the basic and specific and Norwood-Hamilton classifications. J Dermatol. 2013;40:102–6. doi: 10.1111/1346-8138.12024. [DOI] [PubMed] [Google Scholar]