

Abstract
Elastofibromas are rare benign, soft-tissue slow-growing tumors seen predominantly in elderly females. The most common location is the infrascapular region. These benign tumors require resection only in symptomatic cases. We present a case of elastofibroma in a 46-year-old female. She presented with gradually increasing soft-tissue swelling of 8 cm × 6 cm in the right inferior subscapular region for the last 2 years. She underwent excisional biopsy and the histopathology was reported as elastofibroma. Microscopically, the mass showed numerous characteristic eosinophilic, beaded elastic fibers. These fibers were highlighted by the Verhoeff's elastic stain. We present this uncommon case to emphasize the important role of histopathology in diagnosis. A definitive diagnosis helps to avoid unnecessary wide and radical resection.
KEYWORDS: Elastic fibers, elastofibroma, soft-tissue, Verhoeff's stain
INTRODUCTION
Elastofibroma is a rare benign soft-tissue tumor. It is a slow-growing tumor, predominantly seen in elderly females. It often has bilateral location in the thoracic wall. The most common site is in the infrascapular region beneath the muscular tissue.[1] In magnetic resonance imaging (MRI), a preferable noninvasive investigation, elastofibromas typically appear as a solitary, poorly circumscribed, heterogeneous, soft-tissue mass.[2,3] In the absence of a reliable preoperative diagnostic investigation, histopathological examination of biopsy is necessary to confirm the diagnosis in cases of unilateral elastofibromas.
CASE REPORT
A 46-year-old female presented with the complaint of diffuse soft-tissue swelling in the back. The swelling was present since the last 2 years and was gradually increasing in size. It was nontender.
On examination, the mass was present in the right inferior subscapular region. It measured 8 cm × 6 cm in size. The surface of the swelling was smooth [Figure 1]. The routine hematological and biochemical examinations were within normal limits. The MRI was reported as showing focal ill-defined altered signal intensity lesion in right posterolateral chest wall deep to serratus anterior muscle [Figure 2a–d]. The patient underwent fine needle aspiration (FNA) cytology examination that was reported as lipoma. Following this, she underwent excisional biopsy. Grossly, the lesion was irregular, not capsulated, and measured 7 cm × 5 cm in size. The cut section was firm with grayish-white areas [Figure 3].
Figure 1.

Right inferior subscapular swelling
Figure 2.
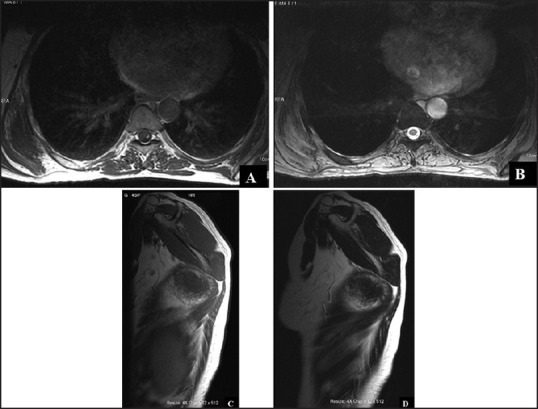
(a and b) MRI image showing focal ill-defined altered signal intensity lesion in the right posterolateral chest wall deep to serratus anterior muscle. The lesion is isointense to muscle in T1 and T2WI images (axial) (c and d) T1 and T2WI images (sagittal) of the lesion
Figure 3.
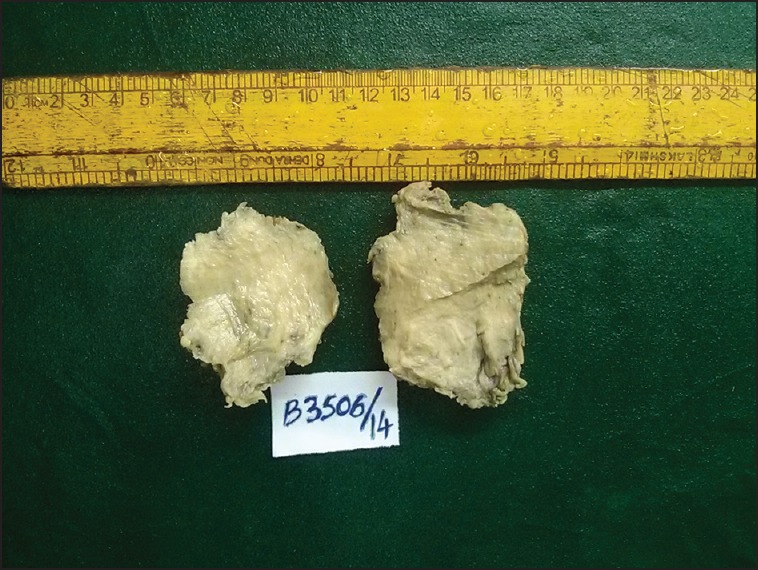
Cut section of the mass with grayish-white areas
Microscopically, the lesion was poorly circumscribed and showed an admixture of collagenous tissue with mature adipocytes. The striking feature in the lesion was the presence of numerous elastic fibers. The elastic fibers were large, coarse, and deeply eosinophilic in nature. Additionally, there were many fragmented ones, which gave the appearance of beads on a string. There was no area of necrosis or increased mitotic activity [Figure 4a and b]. The Verhoeff's elastic stain confirmed the elastic nature of the fibers [Figure 5a and b].
Figure 4.

(a) Lesion with admixture of collagen fibers and adipose tissue with characteristic elastic fibers (Hematoxylin and eosin 10×) (b) The rounded and beaded elastic fibers (Hematoxylin and eosin 40×)
Figure 5.

(a) Verhoeff's elastic stain showing elastic fibers (Verhoeff's elastic stain 10×) (b) The rounded and beaded elastic fibers (Verhoeff's elastic stain 40×)
Based on the characteristic histopathological features and histochemical staining with Verhoeff's stain highlighting elastic fibers, the lesion was diagnosed as a case of elastofibroma. The patient had an uneventful postoperative period.
DISCUSSION
The term elastofibroma was first described by Jarvi and Saxon in 1961.[1,4] It is a rare, benign slow growing soft-tissue tumor. But there is geographic variation and elastofibroma is common in the Japanese population.[5] In Indian medical literature, the data regarding elastofibroma is scant.[6] Though, it has a marked predilection for elderly females, it is often reported in the age group ranging from 35-94 years. The typical location is infrascapular region, occurring predominantly on the right side, but, is bilateral in 30% of the cases.[1,2,7]
Majority of the patients are asymptomatic.[8] Rarely, when symptoms are present, they are pain, scapular snapping, limitation of motion, clunking sensation in the shoulder adduction-abduction movement.[7,8] Majority of the patients are asymptomatic. The present case is a 46-year-old female who presented with a slow growing nontender swelling in the right subscapular region.
Elastofibroma dorsi (ED) is used as a synonym and it is the name given to those lesions in the periscapular region.[1,2] Histogenesis of ED is debatable. Some authors consider it to be a true neoplasm, whereas others presume it a result of reactive hyperproliferation of connective tissue exposed to repetitive minor trauma or friction between the lower scapula and the underlying chest wall.[1,2] According to Nagamine et al., who reported a large series from Japan, genetic factors are implicated in the pathogenesis.[5] However, our patient did not give any family history of similar infrascapular swelling.
The nature of elastic fibers is disputed. Theories suggest that they may be caused by abnormal elastogenesis or by degeneration as a secondary process, or may be by a combination of both processes.[5]
Plain radiographs do not show specific changes apart from a possible soft-tissue signal intensity or elevated scapula.[3] In ultrasonogram, the lesions show alternating pattern of hyperechogenic and hypoechogenic lines. MRI is the investigation of choice and shows a heterogeneous fibrous mass of intermediate density with entrapped signals of higher intensity.[2] Computed tomography (CT) is less sensitive for visualizing the strands of fatty tissue. On positron emission tomography (PET)-CT radiotracer accumulation of the hypermetabolic tumor has been described. Due to its muscle-like appearance in nearly all the imaging procedures, diagnosis of elastofibroma remains challenging.[3] In the present case, the lesion was located on the right side only and no lesion clinically or radiologically was identified on the other side.
It is difficult to distinguish elastofibroma from other benign and malignant soft-tissue tumors of thoracic wall due its rarity. Preoperative procedures such as FNAC and frozen sections are not helpful. FNAC is not recommended as these lesions are hypocellular in nature and in frozen sections, the elastic fibers are difficult to detect.[2]
In the absence of a definitive preoperative diagnosis, there is a chance of inappropriate treatment in the form of radical surgery.[1,8] The clues for the presumptive diagnosis of elastofibroma are advanced age of the patients, the typical localization, female gender, or bilateral manifestation.[9] For a definitive diagnosis of elastofibroma, the role of biopsy is indisputable. A diagnostic biopsy helps to avoid unnecessary radical treatment.
Macroscopically, elastofibroma appear as an irregular, poorly defined, unencapsulated, fibroelastic mass with firm, rubbery consistency. Cut surface reveals whitish fibroelastic tissue admixed with yellowish adipose tissue.[2,3] Histologically, they are dermal in location, unencapsulated, hypocellular masses composed of fibrocollagenous strands mixed with adipose tissue. The collagenous areas showed spindle-shaped nuclei with fine chromatin. The elastic fibers are seen scattered in the collagenous areas. They are deeply eosinophilic serrated or beaded bands and globoid structures. The elastic fibers stain positively with Verhoeff's elastic stain.[2,3]
Immunohistochemically, elastofibromas stain positively for vimentin but negatively for smooth muscle actin, S-100, desmin, and p53. They are frequently positive for cluster of differentiation (CD) 34 and lysozyme.[10] Because the histopathology and Verhoeff's stain findings were classical cases of elastofibroma, we did not perform immunohistochemistry. Ultrastructurally, the elastic fibers appear as granular or fibrillary aggregates of electron-dense material surrounded by an amorphous matrix with scattered microfibrils.[10]
The differential diagnoses include various benign and malignant soft-tissue tumors such as nuchal fibroma, fibrolipoma, fibroma, spindle cell lipoma, and pleomorphic lipoma, aggressive fibromatoses, sarcoma, and subcutaneous metastasis.[2,9] However, the characteristic findings of elastofibroma such as the presence of elastic fibers in a collagenized fibrous tissue with entrapped adipose tissue helps in arriving at the correct diagnosis.
Complete surgical excision in symptomatic patients remains the treatment of choice.[11] These tumors rarely recur and malignant transformation has not been described so far;[2,9] therefore, in asymptomatic lesions there is no need for excision. The role of diagnostic biopsy is to exclude malignancy and to reassure the asymptomatic patient that no radical surgical treatment is necessary.
We present this additional rare case of elastofibroma with its characteristic histopathological findings.
Acknowledgement
The authors wish to thank senior technician Mrs. Ushanandini for her help.
REFERENCES
- 1.Pilge H, Hesper T, Holzapfel BM, Prodinger PM, Straub M, Krauspe R. Elastofibroma: Clinical results after resection of a rare tumor entity. Orthop Rev (Pavia) 2014;6:5329. doi: 10.4081/or.2014.5329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Go PH, Meadows MC, Deleon EM, Chamberlain RS. Elastofibroma dorsi: A soft tissue masquerade. Int J Shoulder Surg. 2010;4:97–101. doi: 10.4103/0973-6042.79797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kransdorf MJ, Meis JM, Montgomery E. Elastofibroma: MR and CT appearance with radiologic-pathologic correlation. AJR Am J Roentgenol. 1992;159:575–9. doi: 10.2214/ajr.159.3.1503030. [DOI] [PubMed] [Google Scholar]
- 4.Järvi OH, Länsimies PH. Subclinical elastofibromas in the scapular region in an autopsy series. Acta Pathol Microbiol Scand A. 1975;83:87–108. doi: 10.1111/j.1699-0463.1975.tb01361.x. [DOI] [PubMed] [Google Scholar]
- 5.Nagamine N, Nohara Y, Ito E. Elastofibroma in Okinawa. A clinicopathologic study of 170 cases. Cancer. 1982;50:1794–805. doi: 10.1002/1097-0142(19821101)50:9<1794::aid-cncr2820500925>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 6.Srinivasan KG, Gaikwad A, Ushanandini KP, Ritesh K. Musculoskeletal. Indian J Radiol Imaging. 2007;17:223–4. [Google Scholar]
- 7.Sarici IS, Basbay E, Mustu M, Eskut B, Kala F, Agcaoglu O, et al. Bilateral elastofibroma dorsi: A case report. Int J Surg Case Rep. 2014;5:1139–41. doi: 10.1016/j.ijscr.2014.10.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lococo F, Cesario A, Mattei F, Petrone G, Vita LM, Petracca-Ciavarella L, et al. Elastofibroma dorsi: Clinicopathological analysis of 71 cases. Thorac Cardiovasc Surg. 2013;61:215–22. doi: 10.1055/s-0032-1328932. [DOI] [PubMed] [Google Scholar]
- 9.Daigeler A, Vogt PM, Busch K, Pennekamp W, Weyhe D, Lehnhardt M, et al. Elastofibroma dorsi - Differential diagnosis in chest wall tumours. World J Surg Oncol. 2007;5:15. doi: 10.1186/1477-7819-5-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gun BD, Bahadir B, Behzatoglu K, Gun MO, Ozdamar SO. Elastofibroma: A clinicopathologic and immunohistochemical study of seven cases and literature review. APMIS. 2007;115:115–9. doi: 10.1111/j.1600-0463.2007.apm_525.x. [DOI] [PubMed] [Google Scholar]
- 11.Nagano S, Yokouchi M, Setoyama T, Sasaki H, Shimada H, Kawamura I, et al. Elastofibroma dorsi: Surgical indications and complications of a rare soft tissue tumor. Mol Clin Oncol. 2014;2:421–4. doi: 10.3892/mco.2014.257. [DOI] [PMC free article] [PubMed] [Google Scholar]