

Abstract
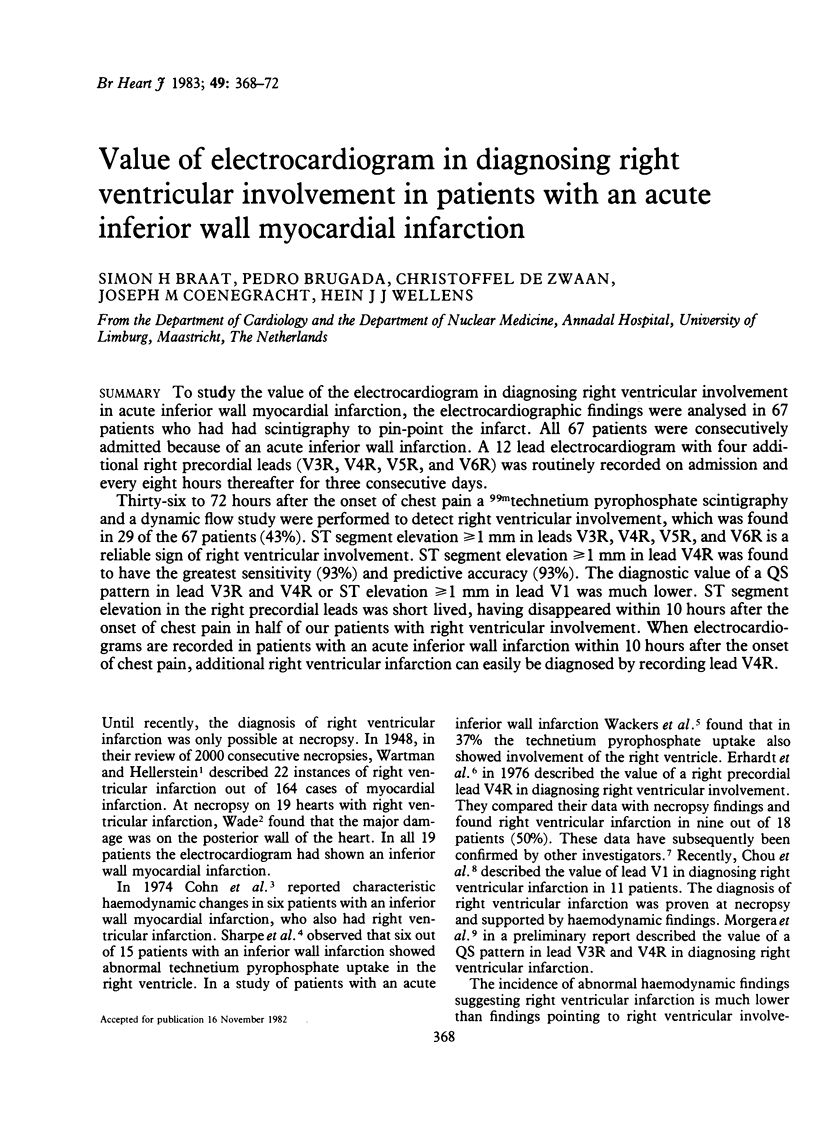
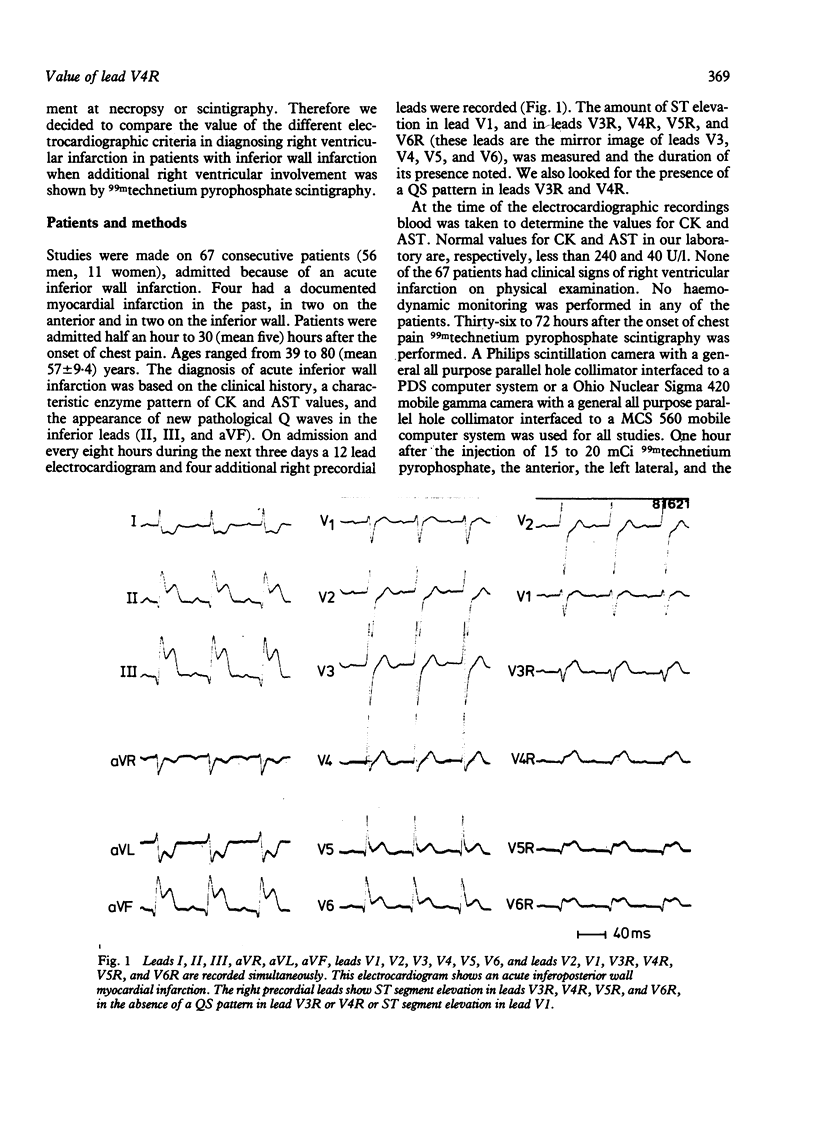
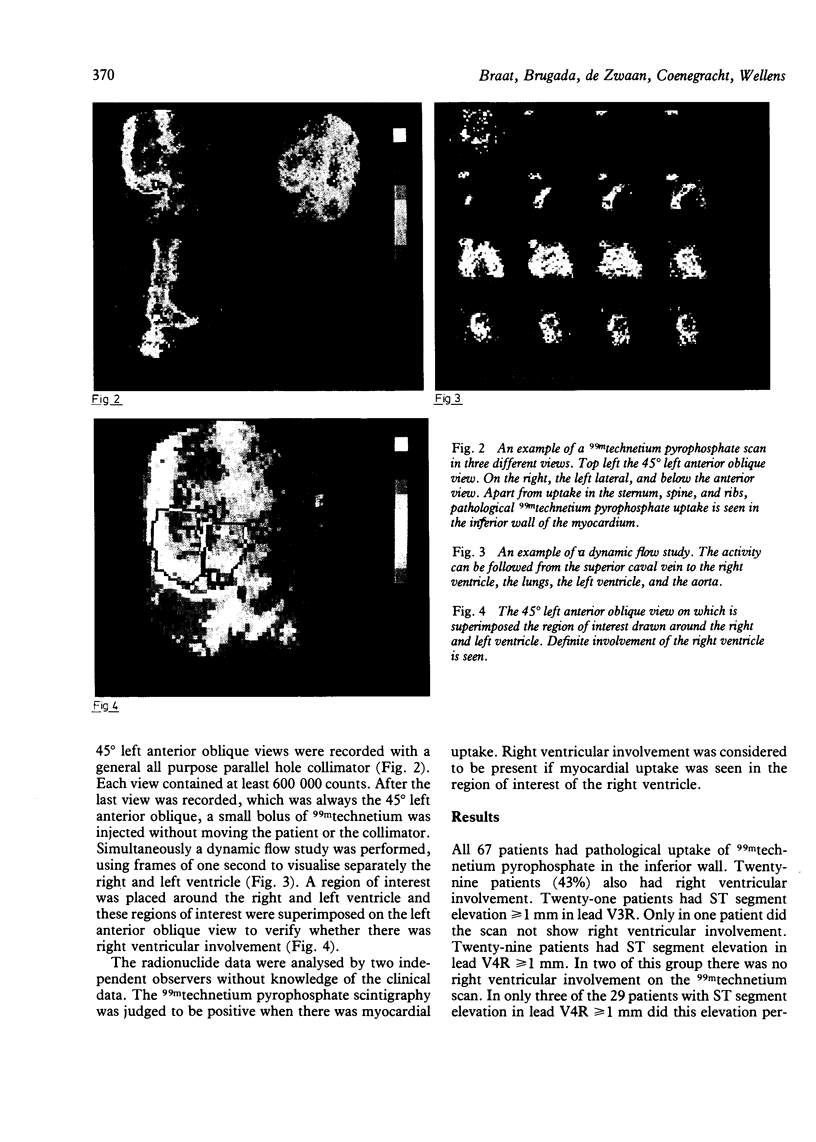
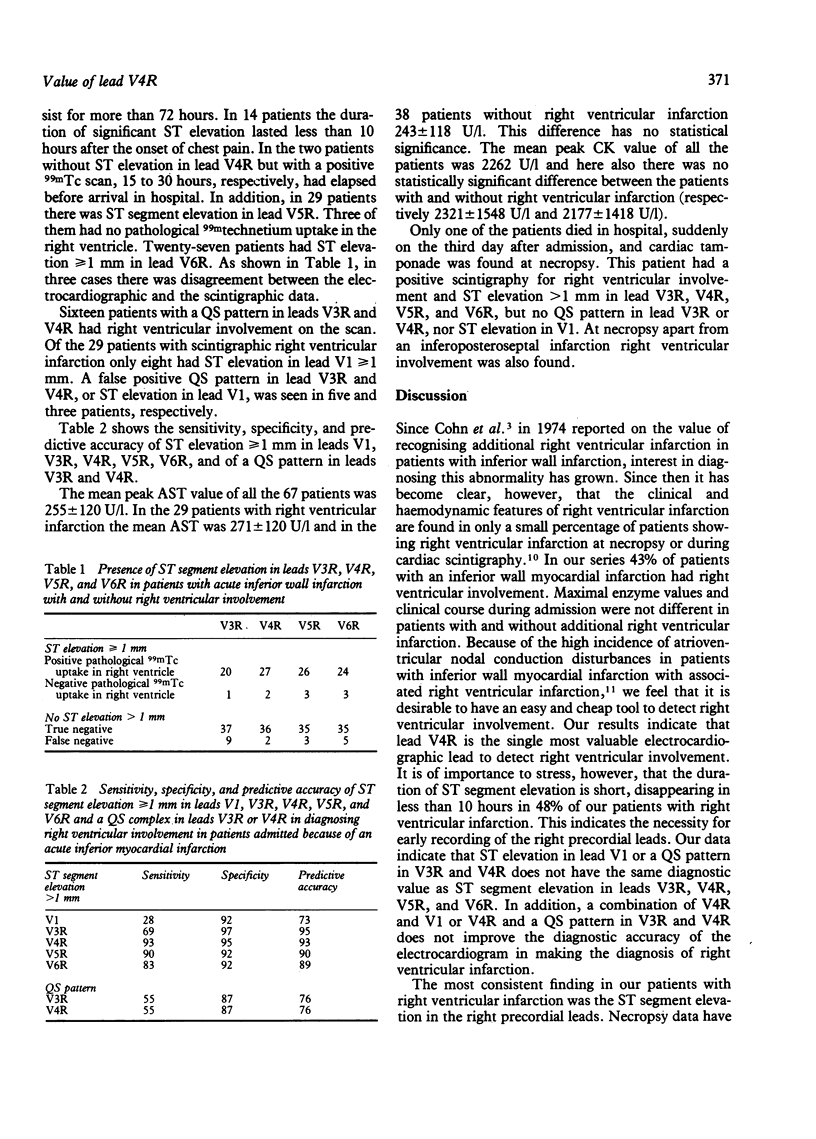
To study the value of the electrocardiogram in diagnosing right ventricular involvement in acute inferior wall myocardial infarction, the electrocardiographic findings were analysed in 67 patients who had had scintigraphy to pin-point the infarct. All 67 patients were consecutively admitted because of an acute inferior wall infarction. A 12 lead electrocardiogram with four additional right precordial leads (V3R, V4R, V5R, and V6R) was routinely recorded on admission and every eight hours thereafter for three consecutive days. Thirty-six to 72 hours after the onset of chest pain a 99mtechnetium pyrophosphate scintigraphy and a dynamic flow study were performed to detect right ventricular involvement, which was found in 29 of the 67 patients (43%). ST segment elevation greater than or equal to 1 mm in leads V3R, V4R, V5R, and V6R is a reliable sign of right ventricular involvement. ST segment elevation greater than or equal to 1 mm in lead V4R was found to have the greatest sensitivity (93%) and predictive accuracy (93%). The diagnostic value of a QS pattern in lead V3R and V4R or ST elevation greater than or equal to 1 mm in lead V1 was much lower. ST segment elevation in the right precordial leads was short lived, having disappeared within 10 hours after the onset of chest pain in half of our patients with right ventricular involvement. When electrocardiograms are recorded in patients with an acute inferior wall infarction within 10 hours after the onset of chest pain, additional right ventricular infarction can easily be diagnosed by recording lead V4R.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Candell-Riera J., Figueras J., Valle V., Alvarez A., Gutierrez L., Cortadellas J., Cinca J., Salas A., Rius J. Right ventricular infarction: relationships between ST segment elevation in V4R and hemodynamic, scintigraphic, and echocardiographic findings in patients with acute inferior myocardial infarction. Am Heart J. 1981 Mar;101(3):281–287. doi: 10.1016/0002-8703(81)90191-5. [DOI] [PubMed] [Google Scholar]
- Chou T. C., Van der Bel-Kahn J., Allen J., Brockmeier L., Fowler N. O. Electrocardiographic diagnosis of right ventricular infarction. Am J Med. 1981 Jun;70(6):1175–1180. doi: 10.1016/0002-9343(81)90824-x. [DOI] [PubMed] [Google Scholar]
- Cohn J. N., Guiha N. H., Broder M. I., Limas C. J. Right ventricular infarction. Clinical and hemodynamic features. Am J Cardiol. 1974 Feb;33(2):209–214. doi: 10.1016/0002-9149(74)90276-8. [DOI] [PubMed] [Google Scholar]
- Croft C. H., Nicod P., Corbett J. R., Lewis S. E., Huxley R., Mukharji J., Willerson J. T., Rude R. E. Detection of acute right ventricular infarction by right precordial electrocardiography. Am J Cardiol. 1982 Sep;50(3):421–427. doi: 10.1016/0002-9149(82)90305-8. [DOI] [PubMed] [Google Scholar]
- Erhardt L. R., Sjögren A., Wahlberg I. Single right-sided precordial lead in the diagnosis of right ventricular involvement in inferior myocardial infarction. Am Heart J. 1976 May;91(5):571–576. doi: 10.1016/s0002-8703(76)80141-x. [DOI] [PubMed] [Google Scholar]
- Lorell B., Leinbach R. C., Pohost G. M., Gold H. K., Dinsmore R. E., Hutter A. M., Jr, Pastore J. O., Desanctis R. W. Right ventricular infarction. Clinical diagnosis and differentiation from cardiac tamponade and pericardial constriction. Am J Cardiol. 1979 Mar;43(3):465–471. doi: 10.1016/0002-9149(79)90001-8. [DOI] [PubMed] [Google Scholar]
- Sharpe D. N., Botvinick E. H., Shames D. M., Schiller N. B., Massie B. M., Chatterjee K., Parmley W. W. The noninvasive diagnosis of right ventricular infarction. Circulation. 1978 Mar;57(3):483–490. doi: 10.1161/01.cir.57.3.483. [DOI] [PubMed] [Google Scholar]
- Wackers F. J., Lie K. I., Sokole E. B., Res J., Van der Schoot J. B., Durrer D. Prevalence of right ventricular involvement in inferior wall infarction assessed with myocardial imaging with thallium-201 and technetium-99m pyrophosphate. Am J Cardiol. 1978 Sep;42(3):358–362. doi: 10.1016/0002-9149(78)90928-1. [DOI] [PubMed] [Google Scholar]
- Wade W. G. THE PATHOGENESIS OF INFARCTION OF THE RIGHT VENTRICLE. Br Heart J. 1959 Oct;21(4):545–554. doi: 10.1136/hrt.21.4.545. [DOI] [PMC free article] [PubMed] [Google Scholar]