

Abstract
Objective:
The aim of this study was to determine the percentage of 5-year-old preschoolers in Sharjah, affected by dental erosion and to assess the predictors.
Materials and Methods:
A total of 403 5-year-old children were examined of which 48.14% (n = 194) were boys and 51.86% (n = 209) were girls; 31.27% (n = 126) were Emirati and 68.73% (n = 277) were non-Emirati Arabs. Examination of dental erosion was confined to palatal surfaces of maxillary incisors using the erosion index described in the UK National Survey of Children's Dental Health, 1993. Dental caries was charted using the World Health Organization 1997 criteria.
Results:
In the sample of 403 5-year-old preschoolers examined, dental erosion was apparent in 237 (58.80%) children, with 55.09% showing the dissolution of enamel and 3.72% exhibiting exposed dentin. Predictors of dental erosion as determined by logistic regression concluded that compared to Emirati citizens other Arab nationalities have 0.27 times the odds (95% confidence interval [CI] =0.18–0.42) of having tooth erosion (P < 0.05). Children with caries experience have 0.28 times the odds (95% CI = 0.16–0.51) of having tooth erosion compared to children with no caries experience (P < 0.05). Children who drink sugary or carbonated beverages have 0.30 times the odds (95% CI = 0.19–0.41) of having dental erosion compared to children who drink water (P < 0.05).
Conclusions:
The findings of this study indicate that 58.80% of 5-year-old preschoolers in Sharjah, United Arab Emirates, were affected by dental erosion. Caries experience and consumption of acidic drinks were associated with dental erosion.
Keywords: Beverages, caries experience, dental erosion, preschoolers
INTRODUCTION
The dissolution of the coronal tooth structure caused by acids from dietary or intrinsic sources (gastric acid reflux) results in dental erosion.[1] The demineralization of enamel occurs due to acid released from fermentable sugars in the bacterial plaque resulting in dental caries.[2] Dental caries is a predominant oral health concern in children, according to surveys conducted in the United States[3] and the United Arab Emirates.[4] The consumption of carbonated beverages and unhealthy dietary habits has been associated with dental caries and tooth erosion according to previous studies.[5]
In recent times, dental erosion has been identified as a major oral health problem among school-aged children.[6] Previous studies on preschoolers have reported the incidence of dental erosion to be at 15.1% in Shanghai (China),[7] 34% in Riyadh (Saudi Arabia),[8] and 47% in Cork City (Ireland).[9] The prevalence of dental caries in the primary dentition in 5–6-year-old has been reported in the region of 72.9–76.1% in Ajman, United Arab Emirates.[4,10] However, information on the frequency and severity of dental erosion among preschoolers in the United Arab Emirates remains limited.
One of the etiological causes of dental caries is frequent snacking and the consumption of acidic dietary foods and liquids.[11] It is important to note that dietary factors contributing to dental erosion/caries tend to correspond.[11] It appears that dental caries and dental erosion are the principal etiological factors of tooth destruction. Studies have revealed that biofilm protection is removed by acidic dietary foods and liquids. Hence, erosion and caries reflect an imbalance within the oral biofilm.[12] Dental complications of erosion include a reduction in the thickness of the enamel affecting esthetics, enamel fracture reducing occlusal vertical dimension and dentin sensitivity.[13] Dental erosion that progresses quite rapidly could result in pulp inflammation and exposure.[13]
The nutritional assessment of children in the United Arab Emirates has revealed that consumption of sugar-sweetened beverages could be a leading cause of dental erosion.[14] The information on the prevalence of dental erosion among preschoolers living in Sharjah is scarce. Hence, the present study was undertaken to determine the percentage of 5-year-old preschoolers affected by dental erosion and to assess the predictors.
MATERIALS AND METHODS
The study was carried out on 5-year-old preschoolers attending kindergarten in Sharjah. Based on a convenience sample, four kindergartens were selected, two of which consisted of only Emirati children and the other two comprised children of Arab ethnicity. A consent form was signed by the parents who granted permission to have their children undergo an oral health examination. This study was conducted with the approval of the Research and Ethics Committee, University of Sharjah, in accordance with the Helsinki Declaration.
A total of 403 children aged 5 years were examined, of these 48.14% (n = 194) were boys and 51.86% (n = 209) were girls; 31.27% (n = 126) were Emiratis and 68.73% (n = 277) were other Arab nationals. The dental examination was done on a portable dental chair with good light illumination. A single calibrated examiner (VKG) carried out the examinations on erosion and dental caries. The daily consumption of beverages was taken into account according to the information provided by the parents.
The examination of dental erosion was confined to palatal surfaces of maxillary incisors[15] using the erosion index described in the UK National Survey of Children's Dental Health.[16] Maxillary incisors with no erosion were scored as 0 whereas score 1 was allocated for loss of enamel surface and score 2 for extensive loss of enamel with dentin involvement. Score 3, which is pulp involvement, was not identified in the present sample and hence excluded. Dental caries was charted using the World Health Organization 1997 criteria.[17]
Statistical analysis
The Chi-square test was used to analyze the null hypothesis that equal proportions of children were with no erosion, enamel erosion, and exposed dentin within the conditions tested. The Mann–Whitney test was used to determine the significance between dmft score values in children with no erosion and erosion. The significance of gender and nationality with erosion/caries was tested using Fisher's exact test. The relationship between consumption of fruit or fizzy drinks with dental erosion was tested using the Chi-square test. Additional multivariate logistic regression analysis was used to assess the predictors of dental erosion. All analyses were conducted using IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp., in which the significant alpha level was 0.05 (two-tailed).
RESULTS
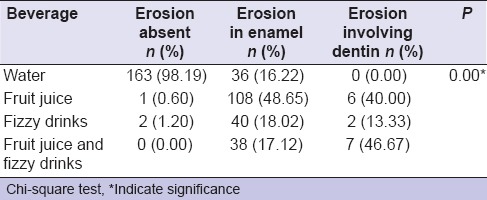
In the sample of 403 5-year-old preschoolers examined, dental erosion was apparent in 237 (58.80%) children, with 55.09% showing the dissolution of enamel and 3.72% exhibiting exposed dentin [Table 1]. Children with erosion had a significantly higher mean dmft score value of 7.11 ± 4.99 (P = 0.00) [Table 2]. While comparing gender and nationality with erosion/caries, it should be noted that children of other Arab nationalities had significantly higher erosion than Emirati nationals (P = 0.00) [Table 3]. Consumption of fruit juice and fizzy drinks was associated with erosion when compared with children who drink water (P = 0.00) [Table 4].
Table 1.
Percentage of children with dental erosion
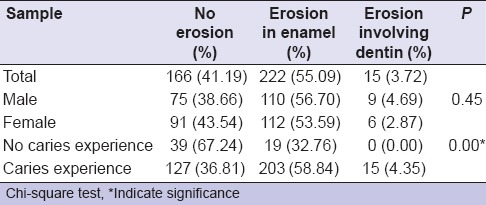
Table 2.
Mean of decayed teeth, missed teeth, filled teeth, and decayed missed filled teeth in the sample
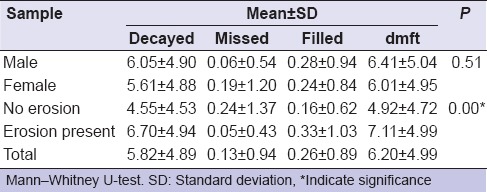
Table 3.
Comparing percentage of erosion and caries experience with gender and nationality

Table 4.
Association of dental erosion with consumption of beverage
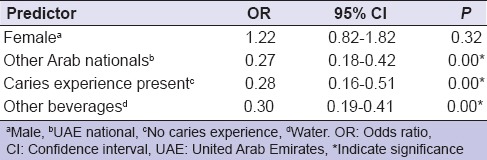
Predictors of dental erosion as determined by logistic regression [Table 5] concluded that compared to Emirati preschoolers, other preschoolers of Arab ethnicity have 0.27 times the odds (95% confidence interval [CI] =0.18–0.42) of having erosion (P = 0.00). Children with caries experience have 0.28 times the odds (95% CI = 0.16–0.51) of having erosion compared to children with no caries experience (P = 0.00). Those who consume fruit juice and fizzy drinks have 0.30 times the odds (95% CI = 0.19–0.41) of having erosion compared to those children who drink water (P = 0.00).
Table 5.
Logistic regression on the predictors of dental erosion
DISCUSSIONS
In the present study, we observed 58.80% dental erosion in 5-year-old preschoolers in Sharjah from a sample of 403 children. The percentage of children affected by dental erosion in the present study is higher when compared to previous reports of 34% in 5–6-year-old in Saudi Arabia;[8] 15.1% in 3–6-year-old in China;[7] and 47% in 5-year-olds in Ireland.[9] In the Irish study[9] conducted in Cork City, 21% of children with erosion had it progress to dentin or pulp whereas the present finding showed only 3.72% with dentin involvement and with no pulp exposures. In similar studies that have assessed erosion in children around the age of 5 years, Taylor[18] reported 98%, which is higher than the present study whereas Walker et al.[19] reported 58% that is comparable. Although the percentage of boys with erosion was higher than girls, it was not significant in the present finding that is supported by the previous survey.[19] Variations in the percentage of children affected by dental erosion noted in previous studies compared to this study could be attributed to lifestyle and urbanization. Hence, dentists should diagnose this condition early and educate parents and children on its prevention and treatment.
A significantly high percentage (54%) of 5-year-old preschoolers with caries experience reported dental erosion. The mean dmft scores in children with erosion in the maxillary incisors were 7.11 ± 4.99 compared with dmft scores of 4.92 ± 4.72 in children with no erosion [Table 2]. This difference of dmft = 2.19 noticed, indicates the child's caries experience is significantly associated with dental erosion (P = 0.00). The present finding is comparable to the report of 2–5-year-old residing in Saudi Arabia with caries experience, who had 33% erosion while compared to caries free children reporting only 27% erosion.[20] It can be presumed that the consumption of cariogenic foods, frequent snacking, and acidic beverages may explain the link observed between dental caries and erosion in the present study.[21]
Examining whether the difference in Arab ethnicity could influence dental erosion, we observed that expatriate Arab nationals living in the United Arab Emirates had 68.59% erosion whereas only 37.30% of Emiratis were affected [Table 3]. Findings similar to these have been observed among different races. Studies conducted in the United States[22] showed Caucasians had more erosion than other races. Similarly, in the United Kingdom,[23] Caucasians had a higher percentage of dental erosion. It can be speculated that in the present study differences noted within the Arab ethnicity could be attributed to cultural and sociodemographic characteristics needing further investigation.
In evaluating the impact of beverage consumption in 5-year-old preschoolers, it was noted that dental erosion was present in 84.81% of the children who consumed fruit/fizzy drinks and in only 15.19% of those who drink water. The results of this study indicated an association between fruit/fizzy drink consumption with erosion (P = 0.00). The findings of the present study are in correlation with studies that showed consumption of carbonated drinks, fruit syrup, and fruit juice are the risk factors for the development of dental erosion.[11,15,23] The reasons for preschoolers being affected by dental erosion when consuming water calls for detailed investigation into their general health (gastroesophageal reflux), snacking, salivary parameters, oral hygiene, and the composition of primary teeth.[24,25]
The factors that were found to have a significant association with tooth erosion in 5-year-old preschoolers that included children of other Arab nationalities living in the United Arab Emirates, caries experience and consumption of fruit/fizzy drinks as determined by logistic regression [Table 5]. Hence, steps should be taken to educate, prevent, and treat this condition. Parental advice should be given toward the treatment of underlying medical disorders, if any. Controlling the frequency of snacking and consumption of acidic drinks along with the professional application of fluoride varnish may further reduce erosion.[26] The fluoride strip treatment has been shown to form CaF2 and fluoride containing apatites at the enamel surface appear to be an effective means to reduce dental erosion.[27] Research has revealed that phosphate salts in the presence of a salivary coating[28] and green tea extracts[29] act as agents to reharden the tooth structure.
CONCLUSION
The findings of this study indicate that the prevalence of dental erosion among 5-year-old preschoolers living in Sharjah, United Arab Emirates, stands at 58.80%. Caries experience and the consumption of acidic drinks are the key factors leading to dental erosion.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest
Acknowledgment
We would like to thank Dr. Marwa Moustafa for her help in data analysis and statistics.
REFERENCES
- 1.Scheutzel P. Etiology of dental erosion – Intrinsic factors. Eur J Oral Sci. 1996;104(2 (Pt 2)):178–90. doi: 10.1111/j.1600-0722.1996.tb00066.x. [DOI] [PubMed] [Google Scholar]
- 2.Nunn J, Shaw L, Smith A. Tooth wear – Dental erosion. Br Dent J. 1996;180:349–52. doi: 10.1038/sj.bdj.4809084. [DOI] [PubMed] [Google Scholar]
- 3.Beltrán-Aguilar ED, Barker LK, Canto MT. Centers for disease control and prevention (CDC). Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis – United States, 1988-1994 and 1999-2002. MMWR Surveill Summ. 2005;54:1–43. [PubMed] [Google Scholar]
- 4.Hashim R, Thomson WM, Ayers KM, Lewsey JD, Awad M. Dental caries experience and use of dental services among preschool children in Ajman, UAE. Int J Paediatr Dent. 2006;16:257–62. doi: 10.1111/j.1365-263X.2006.00746.x. [DOI] [PubMed] [Google Scholar]
- 5.Hasselkvist A, Johansson A, Johansson AK. Association between soft drink consumption, oral health and some lifestyle factors in Swedish adolescents. Acta Odontol Scand. 2014;72:1039–46. doi: 10.3109/00016357.2014.946964. [DOI] [PubMed] [Google Scholar]
- 6.Corica A, Caprioglio A. Meta-analysis of the prevalence of tooth wear in primary dentition. Eur J Paediatr Dent. 2014;15:385–8. [PubMed] [Google Scholar]
- 7.Tao DY, Hao G, Lu HX, Tian Y, Feng XP. Dental erosion among children aged 3-6 years and its associated indicators. J Public Health Dent. 2015;75:291–97. doi: 10.1111/jphd.12098. doi: 10.1111/jphd.12098. [DOI] [PubMed] [Google Scholar]
- 8.Al-Majed I, Maguire A, Murray JJ. Risk factors for dental erosion in 5-6 year old and 12-14 year old boys in Saudi Arabia. Community Dent Oral Epidemiol. 2002;30:38–46. doi: 10.1034/j.1600-0528.2002.300106.x. [DOI] [PubMed] [Google Scholar]
- 9.Harding MA, Whelton H, O'Mullane DM, Cronin M. Dental erosion in 5-year-old Irish school children and associated factors: A pilot study. Community Dent Health. 2003;20:165–70. [PubMed] [Google Scholar]
- 10.Hashim R, Williams S, Thomson WM. Severe early childhood caries and behavioural risk indicators among young children in Ajman, United Arab Emirates. Eur Arch Paediatr Dent. 2011;12:205–10. doi: 10.1007/BF03262808. [DOI] [PubMed] [Google Scholar]
- 11.Al-Malik MI, Holt RD, Bedi R. The relationship between erosion, caries and rampant caries and dietary habits in preschool children in Saudi Arabia. Int J Paediatr Dent. 2001;11:430–9. [PubMed] [Google Scholar]
- 12.Kaidonis J, Townsend G. The 'sialo-microbial-dental complex' in oral health and disease. Ann Anat. 2016;203:85–9. doi: 10.1016/j.aanat.2015.02.002. [DOI] [PubMed] [Google Scholar]
- 13.Harley K. Tooth wear in the child and the youth. Br Dent J. 1999;186:492–6. doi: 10.1038/sj.bdj.4800150. [DOI] [PubMed] [Google Scholar]
- 14.Ali HI, Ng SW, Zaghloul S, Harrison GG, Qazaq HS, El Sadig M, et al. High proportion of 6 to 18-year-old children and adolescents in the United Arab Emirates are not meeting dietary recommendations. Nutr Res. 2013;33:447–56. doi: 10.1016/j.nutres.2013.03.008. [DOI] [PubMed] [Google Scholar]
- 15.Luo Y, Zeng XJ, Du MQ, Bedi R. The prevalence of dental erosion in preschool children in China. J Dent. 2005;33:115–21. doi: 10.1016/j.jdent.2004.08.007. [DOI] [PubMed] [Google Scholar]
- 16.O'Brien M. Office of Population Censuses and Surveys. London: HMSO; 1994. Children's Dental Health in the United Kingdom 1993. [Google Scholar]
- 17.World Health Organization. Oral Health Surveys: Basic Methods. 4th ed. Geneva: WHO; 1997. pp. 40–5. [Google Scholar]
- 18.Taylor CL. MCDH Dissertation. University of Birmingham; 1996. The Prevalence and Distribution of Dental Erosion in 5-Year-Old Children Attending Schools in North Warwickshire. [Google Scholar]
- 19.Walker A, Gregory J, Bradnock G, Nunn J, White D. National Diet and Nutrition Survey: Young People Aged 4 to 18 Years. London: HMSO; 2000. [Google Scholar]
- 20.Al-Malik M, Holt RD, Bedi R. Erosion, caries and rampant caries in Saudi preschool children. J Dent Res. 2000;79:610. [Abs 3734] [Google Scholar]
- 21.Zhang S, Chau AM, Lo EC, Chu CH. Dental caries and erosion status of 12-year-old Hong Kong children. BMC Public Health. 2014;14:7. doi: 10.1186/1471-2458-14-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McGuire J, Szabo A, Jackson S, Bradley TG, Okunseri C. Erosive tooth wear among children in the United States: Relationship to race/ethnicity and obesity. Int J Paediatr Dent. 2009;19:91–8. doi: 10.1111/j.1365-263X.2008.00952.x. [DOI] [PubMed] [Google Scholar]
- 23.Dugmore CR, Rock WP. A multifactorial analysis of factors associated with dental erosion. Br Dent J. 2004;196:283–6. doi: 10.1038/sj.bdj.4811041. [DOI] [PubMed] [Google Scholar]
- 24.Johansson AK, Lingström P, Birkhed D. Comparison of factors potentially related to the occurrence of dental erosion in high- and low-erosion groups. Eur J Oral Sci. 2002;110:204–11. doi: 10.1034/j.1600-0447.2002.11211.x. [DOI] [PubMed] [Google Scholar]
- 25.Moss SJ. Dental erosion. Int Dent J. 1998;48:529–39. doi: 10.1111/j.1875-595x.1998.tb00488.x. [DOI] [PubMed] [Google Scholar]
- 26.Amaechi BT, Higham SM. Dental erosion: Possible approaches to prevention and control. J Dent. 2005;33:243–52. doi: 10.1016/j.jdent.2004.10.014. [DOI] [PubMed] [Google Scholar]
- 27.Lee BS, Chou PH, Chen SY, Liao HY, Chang CC. Prevention of enamel demineralization with a novel fluoride strip: Enamel surface composition and depth profile. Sci Rep. 2015;5:13352. doi: 10.1038/srep13352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.do Amaral JG, Delbem AC, Pessan JP, Manarelli MM, Barbour ME. Effects of polyphosphates and fluoride on hydroxyapatite dissolution: A pH-stat investigation. Arch Oral Biol. 2015;63:40–6. doi: 10.1016/j.archoralbio.2015.11.023. [DOI] [PubMed] [Google Scholar]
- 29.DE Moraes MD, Carneiro JR, Passos VF, Santiago SL. Effect of green tea as a protective measure against dental erosion in coronary dentine. Braz Oral Res 2016;30. 2016;30:pii. doi: 10.1590/1807-3107BOR-2016.vol30.0013. S1806-83242016000100213. [DOI] [PubMed] [Google Scholar]