

Abstract
Objectives The purpose of this study is to experimentally evaluate the use of concentric tube continuum robots in endonasal skull base tumor removal. This new type of surgical robot offers many advantages over existing straight and rigid surgical tools including added dexterity, the ability to scale movements, and the ability to rotate the end effector while leaving the robot fixed in space. In this study, a concentric tube continuum robot was used to remove simulated pituitary tumors from a skull phantom.
Design The robot was teleoperated by experienced skull base surgeons to remove a phantom pituitary tumor within a skull. Percentage resection was measured by weight. Resection duration was timed.
Setting Academic research laboratory.
Main Outcome Measures Percentage removal of tumor material and procedure duration.
Results Average removal percentage of 79.8 ± 5.9% and average time to complete procedure of 12.5 ± 4.1 minutes (n = 20).
Conclusions The robotic system presented here for use in endonasal skull base surgery shows promise in improving the dexterity, tool motion, and end effector capabilities currently available with straight and rigid tools while remaining an effective tool for resecting the tumor.
Keywords: skull base, endoscopic, transnasal, pituitary, Cushing adenoma, surgical robotics, robot, concentric tube continuum robot, active cannula
Introduction
Pituitary adenomas are common, accounting for 15 to 20% of all diagnosed primary brain tumors,1 with autopsy studies suggesting a prevalence of upward of 20%. The techniques and approaches used for the excision of pituitary adenomas continue to evolve. The latest approaches are endoscopic transsphenoidal techniques that many argue are becoming the standard of care. However, all transnasal approaches for pituitary disorders, as well as most other parasellar and skull base diagnoses, suffer from the geometric limitations of operating through a relatively long narrow corridor. Any target at the terminus of the approach that is not largely coaxial with the operative corridor presents a progressive challenge as it moves away from the line of sight of the endoscope. This is further complicated by the fact that most associated instruments and optics in common use for these procedures are straight and rigid. This has been addressed to some degree with endoscopes and instruments with fixed angles, but flexible instruments with actively bending tool shafts are desirable. Some flexible instruments have recently come to market that offer extended reach (e.g., SerpENT [Entrigue Surgical, San Antonio, TX, United States] and XprESS LoProfile [Entellus Medical, Plymouth, MN, United States]), but dexterity at the surgical site is still limited, particularly with respect to axial rotation of the tip of a curved tool at the surgical site.
To address this limitation and provide additional advantages, we describe the use of a custom-built surgical robot for this application. Endonasal surgery is a particularly challenging application for a surgical robot due to the required thinness of each instrument so several of them can pass through a nostril simultaneously, combined with the dexterity required at the surgical site. Prior work on robots for this application has therefore focused not on the coordination of multiple instruments for tumor dissection, but rather on the manipulation of single instruments including the drill used to approach the surgical site2 and the surgical endoscope.3 Thus both of these prior results complement our current approach4 in which a multi-arm robot is deployed after initial preparation with the surgical drill. We believe a robot-assisted approach to endonasal skull base surgery has the potential to surmount technical barriers and broaden the pathology that can safely be addressed via a transnasal approach. As a first step toward demonstrating this potential, in this article we report our experiment exploring whether the system can accomplish pituitary tumor resection with realistic anatomical constraints.
To understand the potential long-term advantages of a robotic system in this application, one can examine how the use of robots has benefited other surgical applications. Robots have been able to manipulate small tools accurately,5 6 enhance surgical dexterity in constrained operative fields,7 8 and scale down surgeon movements to enhance accuracy.9 Robotic systems have been introduced specifically for middle ear,5 laryngeal surgery,7 cardiac surgery,10 among others. We demonstrate in the context of anterior skull base surgery how our robot enables added dexterity, the ability to scale movements, and the ability to rotate the instrument tip axially while holding the instrument tip position stationary on a curved instrument.
Materials and Methods
We used a concentric tube continuum robot made up of a series of concentric precurved tubes, typically made from the superelastic material nitinol (Fig. 1).11 12 13 The tubes rotate and translate inside one another creating a tentacle-like motion. These devices can be made in a wide variety of sizes because nitinol tubing is available in diameters from 0.15 to 14 mm based on manufacturers' stock lists. The robot prototype used in this study consists of three tubes with diameters of 2.4, 1.7, and 1.2 mm, each of which can be translated and rotated by the robot's motors, so the robot has a total of 6 degrees of freedom. Thus the tip of the robot may be positioned in XYZ space and the roll, pitch, and yaw orientation may also be controlled. The modeling of the robot is well established11 14 15 and used here to accurately control the tip of the manipulator. We previously segmented the anatomical workspace available through a single nostril in an average adult skull base surgery patient and designed the robot specifically for skull base surgery.4
Fig. 1.
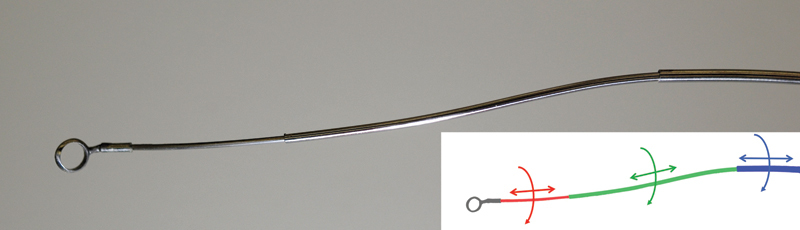
A concentric tube continuum robot made from three precurved superelastic nitinol tubes. The robot is able to move like a tentacle by rotating and translating the tubes inside one another. Each of the 6 degrees of freedom is shown in the inset drawing. An angled ring curette, which can be axially rotated, is attached to the tip of the robot, similar to the curettes used in endonasal pituitary tumor removals.
The nitinol tubes are grasped at their respective bases and rotated and translated using the actuation unit shown in Fig. 2. This prototype consists of two manipulator arms, each with 6 degrees of freedom, with one arm outfitted with a gripper and the other with an angled ring curette taken from a standard Hardy transsphenoidal curette (P/N SP0007011, Codman [Codman, Raynham, MA, United States]). The mechanical design of the robot was described previously,4 and advanced versions are under development.16 A new feature added to the robotic system for this study, not described in previous work, is the ability to change the axial orientation of the angled ring curette without changing the tip position or orientation of the robot. To do this, a nitinol wire that can be axially rotated is passed through the manipulator and the curette is attached to the wire, enabling the surgeon to rotate the curette as desired. This capability is shown in Fig. 3.
Fig. 2.
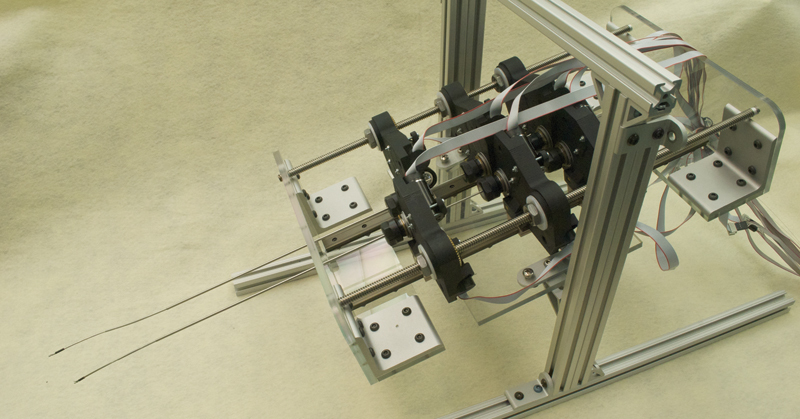
The actuation unit used to translate and rotate the tubes. Each tube is grasped at its base and may be translated and rotated independently of the others, creating a tentacle-like motion.
Fig. 3.

The ability to rotate the ring curette axially while the robot arm remains stationary is illustrated in this image via a semitransparent overlay of a second configuration of the curette.
We implemented teleoperative control of the robot as described previously,4 such that the robot is able to move in a manner that, from the surgeon's perspective, is similar to the da Vinci interface of Intuitive Surgical, Inc. (Sunnyvale, California, United States). In our system, the surgeon manipulates a user interface (Phantom Omni, Sensable, Wilmington, Massachusetts, United States) that controls the position and orientation of the robot manipulator (Fig. 4). The surgeon presses a button on the interface to “clutch in” and begin controlling the tip of the manipulator. The surgeon can “clutch out” by releasing the button to reposition his or her hands to a more comfortable position without moving the robot. Using software, we scaled down the commanded motions from the user interface by 80%, minimizing the effects of hand tremor and enabling the surgeon to make more precise movements. Visualization in this study is provided to the surgeon through a standard straight rigid 4-mm endoscope with a view angle of 30 degrees. Although a rigid endoscope was selected for this pilot study, a flexible endoscope is likely to be used in future design iterations.
Fig. 4.
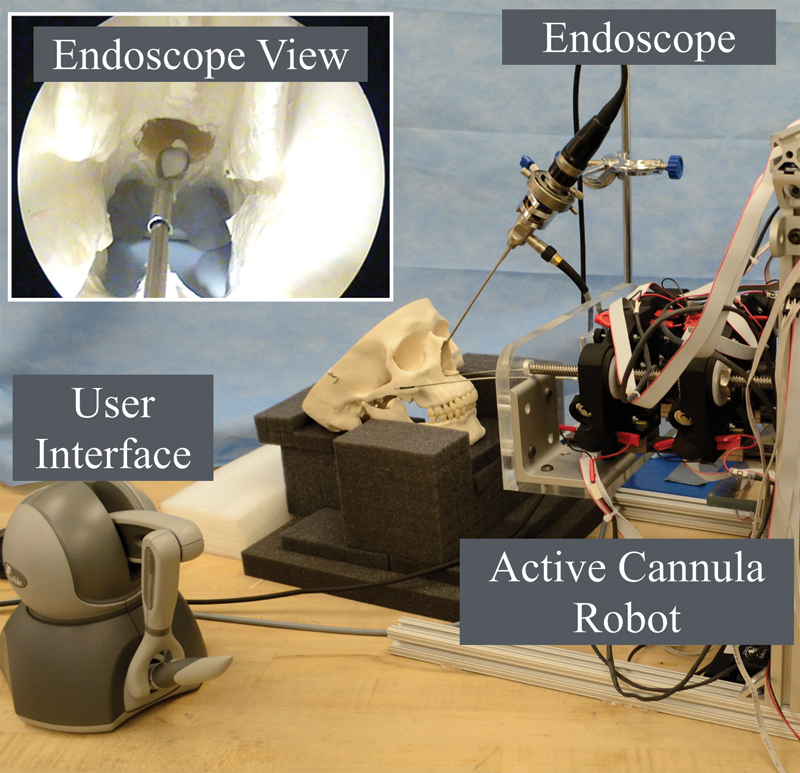
Experimental setup for phantom tumor resection experiments.
We constructed the phantom material using SIM-TEST (Corbin, White City, OR, United States), mixed with water in a ratio of 1 part SIM-TEST to 5 parts water. Qualitatively, the phantom tumor closely resembled a pituitary tumor in consistency. We had previously determined the forces experienced during skull base pituitary tumor removal,17 and the forces are similar to those experienced when resecting a phantom tumor prepared in this way. The phantom tumor was placed in the skull base of an anatomical skull model (#A20, American 3B Scientific, Tucker, GA, United States) that the surgeon prepared to closely replicate an enlarged sella as commonly found in pituitary tumor patients. The longitudinal axis of the prepared sella had a length of 3.18 cm, the vertical axis had a length of 2.11 cm, and the lateral axis had a length of 1.97 cm. The total volume of the sella cavity was ∼ 6.92 cm3. The surgeon navigated the robot through the nasal passage and was tasked with removing as much of the phantom tumor as possible, using only the endoscope view for visualization. Both the endoscope and the skull were fixed in place during the procedure. Manual suction was used to clean the curette from time to time but not to remove phantom tissue directly from within the sella.
Results
Using the robot previously described and shown in Fig. 2, an experienced skull base surgeon performed 20 removals of a phantom pituitary tumor. The skull was weighed to determine the baseline weight and then weighed again after a phantom tumor was inserted into it. Upon completion of the removal, the skull (and any remaining phantom material still in it) was weighed. This allowed us to calculate the percentage removal, and we also recorded the total time for each removal. Fig. 5 shows the percentage removal and time for each removal. The average percentage removal was 79.8 ± 5.9% and the average time to complete the removal was 12.5 ± 4.1 minutes. A thin film of the phantom tumor that covered the surface of the sella was all that was typically left behind after each trial.
Fig. 5.
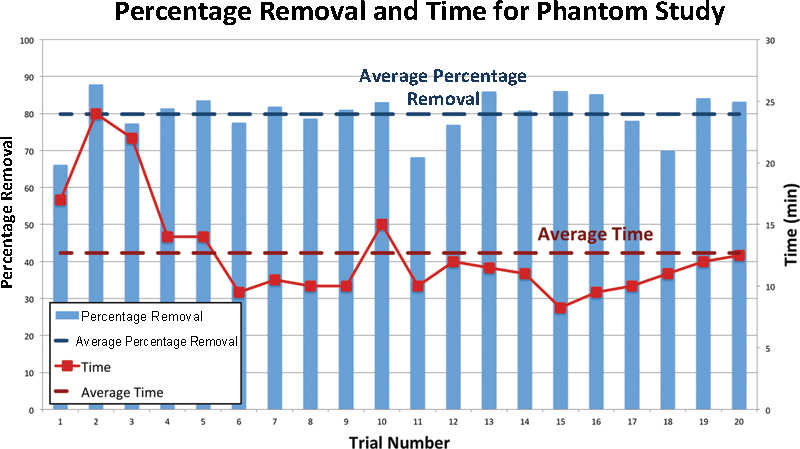
Percentage removal and time to complete removal are shown for all 20 removals. The average percentage removal and average time for removal are overlaid on the data.
Discussion
The results presented here demonstrate that concentric tube continuum robots can provide many of the benefits of robotic surgery to endonasal pituitary tumor resection shown in this phantom pilot study. The average removal time of 12.5 minutes is clinically reasonable. Taken in the context of the total time spent in the operating room, it is a small percentage of the total time. The data suggest the presence of a short learning curve, demonstrated by increased completion time needed in the first few trials. A strong relationship between the percentage removed and the completion time is also evident in trials 1 through 3, followed by a marked decrease in time with relatively steady removal percentages in trials 4 through 6. The operator was familiar with the robot and the teleoperation but had not used the system for 5 months before the beginning of trial 1. Excluding this initial learning period and considering only trials 6 through 20, the standard deviation of the completion time is reduced to 1.6 minutes. Operator fatigue likely explains the increasing times in trials 15 through 20 because trials 6 through 20 were performed in one session.
The 80% average tumor removal is a successful outcome and appears comparable with current resection rates. In one study, “definite tumor remnants or at least suspicious findings” were found in postoperative magnetic resonance imaging scans in 42% of patients.18 Additionally, the results of the experiment are conservative because the experiment did not replicate the effects of hydrostatic pressure in the head, which in live patients exerts a force on the back of the tumor, tending to aid in removal. In comparison with previous results,19 the addition of the axial wrist that allows the curette to rotate axially at the end of the robot enabled a shorter procedure duration and increased the average removal percentage.
In future work, we will design this robot for biocompatibility and sterilizability,20 and provide a simple interface for quickly changing out tools. We will also add multiple manipulator arms to deliver suction, irrigation, and visualization to the surgical site, and will add a wrist to the manipulators that bends in multiple directions to provide even more dexterity to the system. Using methods similar to those previously presented,21 we can prevent tool collisions as well as collisions with bone or other critical anatomical structures, thus reducing some of the mental burden currently required by the surgeon when manipulating multiple tools through a single nostril. In addition to preventing tool collisions, our system can, in principle, implement “no-fly zones” in which the surgeon selects areas of the anatomy on preoperative image data that should be off limits to the manipulators,22 such as the optic nerves in endonasal skull base surgery. We are also interested in comparing the percentage removal and removal time as a function of both surgeon experience with the robot and surgeon training level.
Conclusions
Our experimental results suggest that concentric tube robots can be used to perform pituitary tumor resections. In the longer term, we believe the concentric tube paradigm promises to bring the many benefits typically associated with the da Vinci surgical robot to neurosurgery, particularly skull base surgery, by providing thin and dexterous surgical instruments.
Funding
This work was supported in part by the National Science Foundation (Award IIS-1054331) and in part by the National Institutes of Health (Award R01 EB017467).
References
- 1.American Brain Tumor Association (ABTA) 2011 Available at:http://abta.org/brain-tumor-information/types-of-tumors/pituitary.html. Accessed March 8, 2011
- 2.Matinfar M Baird C Batouli A Clatterbuck R Kazanzides P Robot-assisted skull base surgery IEEE/RSJ International Conference on Intelligent Robots and Systems; 2007865–870.. Available at: http://ieeexplore.ieee.org/xpl/articleDetails.jsp?arnumber=4399012
- 3.Nimsky Ch, Rachinger J, Iro H, Fahlbusch R. Adaptation of a hexapod-based robotic system for extended endoscope-assisted transsphenoidal skull base surgery. Minim Invasive Neurosurg. 2004;47(1):41–46. doi: 10.1055/s-2003-812465. [DOI] [PubMed] [Google Scholar]
- 4.Burgner J, Rucker D C, Gilbert H B. et al. A telerobotic system for transnasal surgery. IEEE ASME Trans Mechatron. 2014;19(3):996–1006. doi: 10.1109/TMECH.2013.2265804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Miroir M Nguyen Y Szewczyk J et al. RobOtol: from design to evaluation of a robot for middle ear surgery Available at: http://ieeexplore.ieee.org/xpl/login.jsp?tp=&arnumber=5650390. IEEE/RSJ International Conference on Intelligent Robots and Systems; 2010:850–856
- 6.Taylor R, Jensen P, Whitcomb L. et al. A steady-hand robotic system for microsurgical augmentation. Int J Robot Res. 1999;18(12):1201–1210. [Google Scholar]
- 7.Simaan N, Xu K, Kapoor A. et al. Design and Integration of a telerobotic system for minimally invasive surgery of the throat. Int J Robot Res. 2009;28(9):1134–1153. doi: 10.1177/0278364908104278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lanfranco A R, Castellanos A E, Desai J P, Meyers W C. Robotic surgery: a current perspective. Ann Surg. 2004;239(1):14–21. doi: 10.1097/01.sla.0000103020.19595.7d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Prasad S M, Prasad S M, Maniar H S, Chu C, Schuessler R B, Damiano R J Jr. Surgical robotics: impact of motion scaling on task performance. J Am Coll Surg. 2004;199(6):863–868. doi: 10.1016/j.jamcollsurg.2004.08.027. [DOI] [PubMed] [Google Scholar]
- 10.Gosline A H, Vasilyev N V, Butler E J. et al. Percutaneous intracardiac beating-heart surgery using metal MEMS tissue approximation tools. Int J Robot Res. 2012;31(9):1081–1093. doi: 10.1177/0278364912443718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Webster R J III, Romano J M, Cowan N J. Mechanics of precurved-tube continuum robots. IEEE Trans Robot. 2009;25(1):67–78. [Google Scholar]
- 12.Dupont P E, Lock J, Itkowitz B, Butler E. Design and control of concentric-tube robots. IEEE Trans Robot. 2010;26(2):209–225. doi: 10.1109/TRO.2009.2035740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gilbert H, Hendrick R, Remirez A, Webster R III. A robot for transnasal surgery featuring needle-sized tentacle-like arms. Expert Rev Med Devices. 2014;11(1):5–7. doi: 10.1586/17434440.2013.854702. [DOI] [PubMed] [Google Scholar]
- 14.Rucker D C, Webster R J III, Chirikjian G S, Cowan N J. Equilibrium conformations of concentric-tube continuum robots. Int J Robot Res. 2010;29(10):1263–1280. doi: 10.1177/0278364910367543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rucker D C, Jones B A, Webster R J III. A geometrically exact model for externally loaded concentric-tube continuum robots. IEEE Trans Robot. 2010;26(5):769–780. doi: 10.1109/TRO.2010.2062570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Swaney P J Croom J M Burgner J et al. Design of a quadramanual robot for single-nostril skull base surgery ASME Dynamic Systems and Control Conference/Vibration Control Conference; 2012:387–393
- 17.Bekeny J R, Swaney P J, Webster R J III, Russell P T, Weaver K D. Forces applied at the skull base during transnasal endoscopic transsphenoidal pituitary tumor excision. J Neurol Surg B Skull Base. 2013;74(6):337–341. doi: 10.1055/s-0033-1345108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fahlbusch R, Ganslandt O, Buchfelder M, Schott W, Nimsky C. Intraoperative magnetic resonance imaging during transsphenoidal surgery. J Neurosurg. 2001;95(3):381–390. doi: 10.3171/jns.2001.95.3.0381. [DOI] [PubMed] [Google Scholar]
- 19.Gilbert H B Swaney P J Burgner J Weaver K D Russell T III Webster R J III A feasibility study on the use of concentric tube continuum robots for endonasal skull base tumor removal Hamlyn Symposium on Medical Robotics; 2012
- 20.Burgner J, Swaney P J, Lathrop R A, Weaver K D, Webster R J III. Debulking from within: a robotic steerable cannula for intracerebral hemorrhage evacuation. IEEE Trans Biomed Eng. 2013;60(9):2567–2575. doi: 10.1109/TBME.2013.2260860. [DOI] [PubMed] [Google Scholar]
- 21.Sun W Torres L G van den Berg J Alterovitz R Safe motion planning for imprecise robotic manipulators by minimizing probability of collision International Symposium on Robotics Research; 2013
- 22.Abbott J J Marayong P Okamura A M Haptic virtual fixtures for robot-assisted manipulation Available at: http://www.eng.utah.edu/∼jabbott/pmwiki/uploads/Main/Abbott_RoboticsResearch07.pdfSpringer Tracts in Advanced Robotics 20072849–64. [Google Scholar]