

Abstract
Background:
Self-regulation is one of the current psychological concepts that have been known as a determinant of leisure time physical activity. Due to cultural and social diversity in different societies and age groups, application of specific questionnaires is essential to perform investigations about physical activities. The aim of this study is development and evaluation of psychometric properties of a self-regulation questionnaire about leisure time physical activity in Iranian male adolescents.
Materials and Methods:
This cross-sectional study was conducted in 2013, and data of 603 male students from 12 high schools in Isfahan were collected. A comprehensive literature review and similar questionnaire review were conducted and 25 items were selected or developed to measure self-regulation. Comprehensibility of items was evaluated in a pilot study and an expert panel evaluated face and content validity. Exploratory factors analysis (EFA) was used for evaluation of construct validity and extraction of sub-constructs of self-regulation. Leisure time physical activity was assessed using International Physical Activity Questionnaire (IPAQ).
Results:
The mean age of the participants was 16.3 years (SD =1.0) and the range was 15-19 years. Cronbach's α coefficient of the questionnaire in the pilot and main study was 0.84 and 0.90, respectively. EFA resulted in four sub-constructs including “enlistment of social support”, “goal setting”, “self-construction”, and “self-monitoring”, which explained 63.6% of the variance of self-regulation.
Conclusions:
Results of this investigation provide some support to the validity and reliability of the 16-item questionnaire of self-regulation abut leisure time physical activity in the target group.
Keywords: Adolescent, exercise, Iran, physical activity, questionnaire, reliability, self-regulation, validity
INTRODUCTION
Despite the fact that physical inactivity has been known as a risk factor for non-communicable, chronic diseases,[1] reduced participation in physical activities is one of the changes that has occurred recently in lifestyle.[1,2,3] This problem is not specific to a particular population, and adolescents are at risk of physical inactivity as well.[4,5] Based on the Centres for Disease Control and Prevention report, in 2011, only 29% of high school students in the USA had satisfactory physical activity.[6] However, the US Department of Health and Human Services recommends that performing at least 60 min of physical activity per day is necessary to maintain and improve adolescents’ health. These physical activities must be repeated 3 days or above per week, and include strength exercises to increase the capability of main muscles of the body and limbs and aerobic activities to increase cardiorespiratory capacity.[7] Contrary to public perceptions, adolescents’ physical inactivity is also highly prevalent in developing communities, as in developed communities.[8] A study published in 2010 demonstrated that over 60% of adolescents in Iran showed lack of adequate physical activity.[9] Available evidence shows that there is an obvious decline in physical activity after childhood and inactivity is likely to become a personal habit continuing in older ages.[3,4,5,10] Therefore, the researchers highlight the need to conduct studies aimed to increase the participation of adolescents in regular physical activities and promote community's health.[2,3]
Physical activity, as with many other behaviors, is influenced by several individual, inter-personal, and environmental determinants.[11,12] Unsuitable circumstances that prevail currently around humans do not generally support healthy behaviors.[13,14] The spread of access to digital technologies and the reduced need for physical activities to do daily tasks and for transportation are some of the most important changes in environmental factors related to physical activity. The historical balance between energy intake and expenditure in humans is disrupted in this environment. In such a situation, the importance of intra-personal factors, alongside self-care, reassuring efforts, and protective behaviors, increases further.[13] Self-regulation is one of these determinants which exerts indirect effects on physical activity at inter-personal and environmental levels, in addition to individual level.[15]
Despite different definitions have been offered, self-regulation refers to a variety of strategies and behaviors used to adopt and/or maintain the behaviors associated with health.[16,17] According to Bendura, self-regulation is exerted through a variety of cognitive and behavioral mechanisms such as self-monitoring, goal setting, feedback, self-reward, self-instruction, enlistment of social support, and enables the individual to control individual and environmental health-related factors.[18] Through maintaining provision of practical guidelines and offering effective feedbacks on behavior and its outcomes, self-regulation enables the individual to have a high control of his/her behavior.[19]
Many times, exercise and physical activity require disregard of short-term joys to achieve a more valuable benefit in the future. Bearing short-term negative consequences in order to achieve long-term positive outcomes, as one of the known human capacities, is accomplished by self-regulation mechanisms.[20] Some studies have demonstrated self-regulation as a mediator between self-efficacy construct and physical activity, alongside its direct role in physical activity.[9,21]
Given the role of self-regulation construct in analysis and moderation of physical activity-related behaviors, availability of an appropriate instrument to measure this psychological construct is particularly important. So, different types of questionnaires have been presented up to now for the assessment of self-regulation about leisure time physical activity.[20,21,22,23,24] One of the commonly used instruments to measure physical activity-related self-regulation is the 43-item questionnaire (PASR-43) introduced by Petosa in 1994. This questionnaire, which has been developed to measure self-regulation in middle-aged population, consists of six main sub-constructs. Today, the questionnaires such as PASR-43 have been translated into different languages, including Persian, and are commonly used to measure self-regulation construct.[9,16]
Although one of the benefits of administering standard questionnaires is to save research resources, the efficiency of each questionnaire is mostly dependent on the social and cultural specifications of the populations which are going to be measured by the questionnaire.[25] One of the specifications of a good questionnaire is the ability to uniformly assess the individuals of various age groups, gender, and ethnic populations with specific educational level and other demographic characteristics. This characteristic of a questionnaire is referred to as fairness. Although fairness of a questionnaire makes the findings of a study in which it has been administered highly generalizable, lack of a quantitative approach for assessing this characteristic and validity's dependency on specifications of the target population have caused failure to address fairness satisfactorily.[26] As a result, several studies have demonstrated the weakness of common questionnaires in view of fairness. For example, in Umstattd et al.'s study conducted in 2009 on the elderly adults, construct validity of Petosa questionnaire was demonstrated as unacceptable.[22] Similar studies conducted recently have shown the significance of use of specific measurement instruments in populations with different cultural, language, age, and gender characteristics.[22,27,28,29] In addition, the passage of time could influence an instrument's capability of measuring psychological constructs in a particular population.[25]
Despite the significance of using specific instruments to measure the factors related to physical activity, no evidence has yet been obtained regarding a specific instrument to measure self-regulation construct in adolescents in Iran. Therefore, the present study seeks to show the steps of development and psychometric evaluation of a specific 16-item questionnaire to measure self-regulation construct in Iranian male adolescents. This questionnaire is expected to be administered with fewer items than in similar questionnaires to conduct observational and interventional studies.
MATERIALS AND METHODS
Type of study
This study is a cross-sectional, descriptive study conducted in April and May, 2013, in Isfahan, Central Iran. Isfahan was divided into three regions, privileged, semi-privileged, and sub-privileged, based on relevant studies of socioeconomic status[30] and the viewpoints of municipal experts and healthcare professionals. Then, four high schools were randomly enrolled from each region. After explaining the research purposes, we gave necessary explanations to the students regarding the confidentiality of data and volunteer participation. The inclusion criteria for the study were: Age 15-19 years, lack of a major health problem preventing regular physical activity, and no membership in professional sports teams. Unwillingness and failure to fill out the questionnaire were considered as the exclusion criteria.
Thus, 650 male adolescents of age 15-19 years, living in Isfahan, participated in the study. But 47 questionnaires were set aside due to failure to fill them out completely. Therefore, data on 603 students were analyzed.
Measurement instrument
The rate of physical activity during leisure time was determined by the long form of International Physical Activity Questionnaire (IPAQ). This questionnaire was developed by a group of Italian researchers in 1998 and administered in observational and interventional studies after being translated into various languages, including Persian.[31,32] Reliability and validity of the Persian version of IPAQ were assessed in several studies. In a study conducted in Tabriz, Iran, content validity index (CVI) and content validity ratio (CVR) of IPAQ were derived and found to be 0.85 and 0.77, respectively. In addition, Cronbach's alpha of this questionnaire in a Persian-speaking population was estimated as 0.7 and Spearman's correlation coefficient was estimated as 0.9 by test-retest. Using this questionnaire, the individuals could be assigned to three groups: Lowly active (less than 600 MET-min/week), moderately active (between 600 and 3000 MET-min/week), and severely active (higher than 3000 MET-min/week).[33]
The instrument recommended for self-regulation measurement consists of 16 items. This instrument measures the rate of use of self-regulation mechanisms in the past 4 weeks by propositions of “always,” “often,” “sometimes,” “rarely,” and “never.”
Process of development of measurement instrument and evaluation of validity and reliability
After review of the literature, 25 items were developed to measure self-regulation construct about leisure time physical activity. Some of the items were already used identically in previous studies and translation of these items into Persian was done by translation-back translation method by two health experts who had mastered the language.
The items were examined for face validity and cultural adaptation by five experts of health education to evaluate qualitatively as per some criteria including compliance with the principles and rules of Persian language, simplicity, comprehensibility, relevance, appropriateness to the construct of interest, and lack of ambiguity.[34]
CVR of each item was also assessed according to Lawshe method by 10 other experts of health education who formed the expert panel.[34,35] This panel commented on each item as “essential,” “useful but non-essential,” and “non-essential.”
To determine CVI, simplicity, specificity, and clarity were considered. For simplicity, the options used were “quite simple,” “simple,” “relatively simple,” and “not simple.” For specificity, the options were “highly relevant,” “relevant,” “moderately relevant,” and “irrelevant.” For clarity, they were “quite clear,” “clear,” “relatively clear,” and “unclear.” Comprehensibility of the questionnaire was assessed in a pilot study of 35 members of the target population who were not enrolled in the final study, using the options “fully comprehensible,” “comprehensible,” “relatively comprehensible,” and “not comprehensible.” The number of “fully comprehensible” and “comprehensible” ticked items was divided by 35 to derive comprehensibility coefficient.
To derive reliability coefficient, we administered the questionnaire to 75 members of the target population who were not enrolled in the final study and the internal consistency criterion was used.
Data analysis
After analysis of the items, exploratory factor analysis (EFA) was run to estimate the construct validity of the questionnaire. Since the recommended instrument contained a number of sub-divisions, the extraction step was done with the presupposition of principle components. Because of the potential correlation among these sub-divisions, the type of rotation of the items was determined promax. The above statistical tests were run using SPSS, version 19.
Ethical considerations
The study was started after approved by Isfahan University of Medical Sciences and Isfahan Education organization.
Ethical approval was granted by the deputy of research and technology of Isfahan university of medical sciences
The purpose and procedures of the study were explained to the participants, and researcher's emphasis on confidentiality of data and voluntary nature of participation.
Parental informed consent and student dissent were considered as an Inclusion criteria.
The investigators guaranteed that there were no any conflicts of interest.
RESULTS
Mean age of the participants in the study was 16.3 ± 1.0 (range: 15-19) years.
Determining face validity, CVI, CVR, comprehensibility, and reliability coefficient of the questionnaire
As per the comments of the five-member expert panel, 12 out of total 25 items were revised and changed for phrasing and 6 items were deleted. Also, two new items were added to the previous items. The expert panel believed that addition of these two items enhances the questionnaire's coverage of various dimensions of self-regulation construct and promotes its validity. These items were included as no. 8 and 16 in the final questionnaire. Item no. 8 addresses an individual's effort to find a solution when facing the barriers to physical activity. Item no. 16 reflects an individual's requesting others around to be able to run one's physical activity. Then, CVR of the remaining items was calculated and on using the relevant formula, the CVR of five items did not register the threshold level, and hence, the items were excluded.
Given that 0.79 was considered as the items’ CVI acceptability to remain in the questionnaire,[34] all the remaining items (n = 16) were satisfactory with regard to CVI. After administering the questionnaire in the pilot study, we determined 0.79 as the acceptable comprehensibility and all items met the comprehensibility requirements. Also, the questionnaire's Cronbach's alpha was investigated in a pilot study of 75 members of the target population and was found to be 0.84.
Participation in physical activities
After exclusion of outliers, the mean physical activity was found to be 2324 ± 1437 MET-min/week and the mean physical activity in leisure time was 842 ± 831 MET-min/week. Also, 293 (49%) participants had low activity, 278 (46%) had moderate activity, and 32 (5%) had high activity.
Items analysis
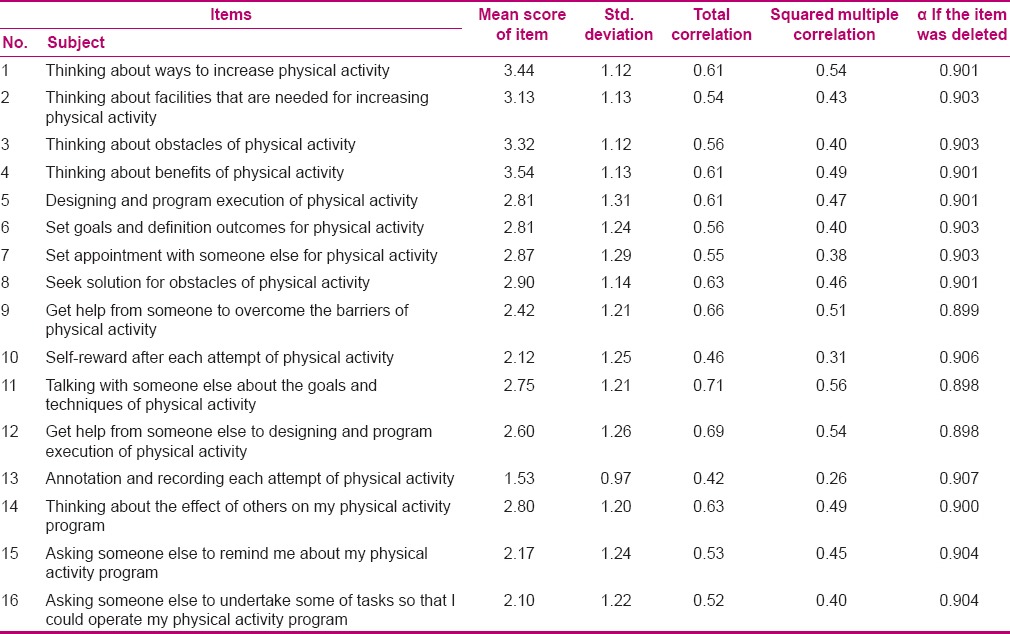
The questionnaire's Cronbach's alpha was found to be 0.90 after 603 participants filled it up. By correlation matrix, all the recommended items had a correlation coefficient of higher than 0.4 with the other items (P ≤ 0.005). All the items were determined as acceptable and none of them was excluded [Table 1].
Table 1.
Item Total statistic of self-regulation questionnaire abut leisure time physical activity in Iranian male adolescents
Exploratory factor analysis
Kaiser–Meyer–Olkin index was found to be 0.92 and Bartlett's test of sphericity was significant at 95% CI (χ2= 4139, df =120, P = 0.00). Given the adequacy of sample size and correlation matrix's appropriateness to factor analysis, the data were included in the EFA.
By this test, four main factors were generated, which explained 63.6% of the variance in self-regulation.
The first factor included the items 9, 11, 12, 14, 15, and 16. This factor alone explained 42.3% of the variation in self-regulation total score and the internal consistency coefficient of the items relevant to this factor was estimated as 0.85 by Cronbach's alpha. Out of the relevant items to this factor, item no. 15 yielded the highest (0.737) correlation. This item addressed requesting others around to remind the individual of the time of physical activity. Item no. 11 yielded the lowest (0.607) correlation; it reflected the individual's conversations with others about the ways to develop and implement physical activity and also correlated with item no. 2 (0.408).
The second factor included the items 5, 6, 7, 8, and 11. This factor explained 9.6% of the variation in self-regulation and the Cronbach's alpha of the items relevant to this factor's total items was found to be 0.81. Item no. 6 addressing goal setting and item no. 7 representing schedule development to do physical activity yielded the highest (0.703) correlation with item no. 2. Item no. 11 yielded the lowest (0.408) correlation [Table 2].
Table 2.
Rotated component and structure matrix with PCA and promax rotation for items of self-regulation questionnaire related to leisure time physical activity in Iranian male adolescents
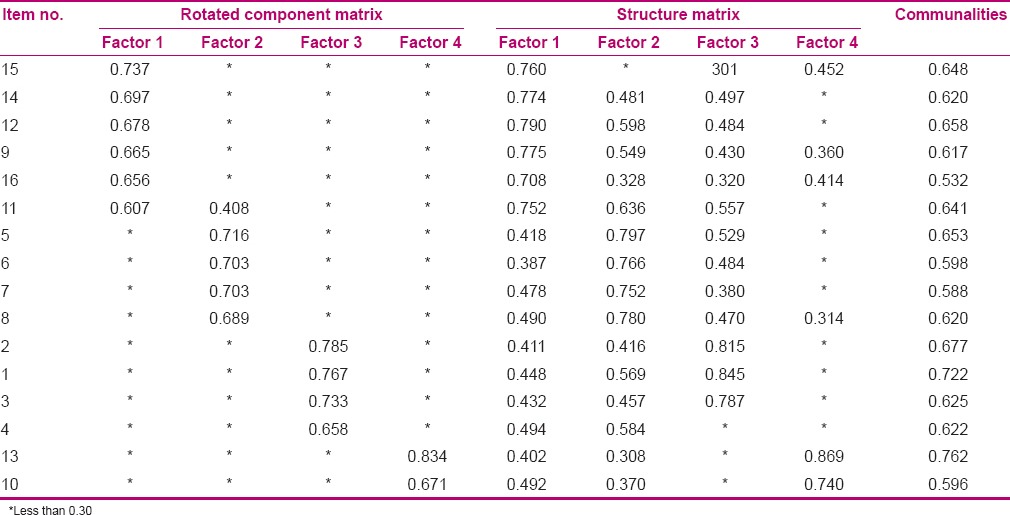
The third factor included the items 1, 2, 3, and 4. This factor explained 6.3% of the variation in self-regulation and the Cronbach's alpha of the items relevant to this factor's total items was found to be 0.82. Item no. 2 addressing the required facilities for physical activity yielded the highest (0.785) correlation with item no. 3. Item no. 4 yielded the lowest (0.650) correlation and it addressed the benefits of physical activity.
The fourth factor included the items 10 and 13. This factor explained 5.2% of the variation in self-regulation. Item no. 13 (0.671) addressed registry of performed physical activity and item no. 10 (0.834) was related to self-reward after each accomplishment in performing physical activity or its constituents. The internal consistency of the items related to this factor was derived as 0.68 by Cronbach's alpha.
DISCUSSION
This study was conducted to evaluate the psychometrics of a 16-item questionnaire specifically developed to measure self-regulation related to leisure time physical activity in Iranian male adolescents. For this, reliability, content validity, and construct validity of this instrument were assessed by a logical and common way.
The questionnaire's reliability was assessed by internal consistency and Cronbach's alpha in two steps. In the pilot study, Cronbach's alpha coefficient was derived as 0.84 and total internal consistency was found to be satisfactory. This index was also estimated as 0.90 after the questionnaires were filled out. This coefficient was reported 0.96 in Yeom et al.'s study. The findings of the present study are consistent with the reliability coefficient of the 53-item questionnaire introduced by Petosa and calculated by test-retest.[22] In addition, Cronbach's alpha was found to be 0.85 for enlistment of social support, 0.81 for goal setting and schedule development, 0.82 for self-instruction, and 0.68 for self-monitoring, representing satisfactory consistency of the items associated with any sub-construct of the questionnaire except self-monitoring. In Petosa's study, although the Cronbach's alpha was reported as 0.79 for self-monitoring, this index was found to be 0.62 for one of the measured sub-constructs, i.e. reinforcement. In Petosa's opinion, the emphasis of the items related to a sub-construct on the behavioral mechanisms of self-regulation and failure to address cognitive behaviors could explain the relatively low internal consistency of the items.[22] Hence, future studies are expected to enhance the internal consistency of this sub-construct by introducing one or two items related to cognitive processes of self-regulation.
To achieve satisfactory face and content validity, we elicited the comments of health experts to determine the CVI and CVR of the 25 recommended items and then unsatisfactory items were excluded. Finally, 16 items remained in accordance with the experts’ comments elicited in different steps. The efforts to achieve content validity were initiated since the questionnaire's development. Brons and Gorow have offered literature review and eliciting the comments of experts and the representatives of the target population as the most important measures to achieve content validity for measurement instruments, which should be considered at the step of instrument development.[36] Therefore, the comments of five health experts outside the research team were elicited after literature review in the present study. These comments helped the researchers consider different dimensions of physical activity-related self-regulation and the contribution of each factor in the final items of the questionnaire at the step of instrument development.
EFA yielded four sub-constructs for the questionnaire. The first factor was mostly correlated with the items 9, 11, 12, 13, 14, 15, and 16, all of which are related to a sub-division of self-regulation construct addressing an individual's effort to garner social and environmental support. Therefore, this factor was named enlistment of social support. The associated items with this factor address thinking about the influence of others around on physical activity schedule, seeking assistance from others around to remind one of the time of physical activity, requesting them to eliminate the existing barriers to performing physical activity, and talking about the purposes and ways of performing physical activities with others. The second factor including the items 5, 6, 7, 8, and 11 exhibited the highest correlation. This factor, namely goal setting, included the issues concerning setting goal and developing physical activity schedule. The items included in the second factor sub-division address the issues including development of a regular schedule and setting of specific output and behavioral goals for physical activity, planning for performing physical activity schedule along with others, planning for solving current problems, as well as talking about the purposes and methods of performing physical activity with others. Notably, item no. 11 was concurrently correlated with the first and second factors, concerning talking with others about the purposes and ways of performing physical activity schedule. As this item is related to both planning and enlistment of social support, its correlation with both first and second factors could be justified.
The third factor, namely self-instruction, included the items 1, 2, 3, and 4. These items assessed the rate of thinking about physical activity benefits, the ways to increase physical activity, and the facilities of and barriers to performing physical activity. The fourth identified factor was named self-monitoring. This factor was mostly correlated with the items 10 and 13. These two items address the registry of performed physical activities and rewarding self for accomplishment of physical activity performance. However, the questionnaire developed by Petosa has identified six sub-constructs consisting of goal setting, self-monitoring, time management, enlistment of social support, reinforcements, and relapse prevention.[16,22,37] Fleury introduced the Index of Self-regulation in 1998 to measure the self-regulation related to physical activity.[38] The initial target population of this 9-item questionnaire includes middle-aged adults and only three dimensions, including stimulus control, behavior maintenance, and behavior monitoring, have been considered.
In recent years, some items of this questionnaire were used to develop specific questionnaires to particular target populations and the validity and reliability of the new questionnaires were reported.[20] The difference in the number of generated sub-constructs between the present study and two other studies could be attributed to the development and selection of the items as per the experts’ comments. These items were introduced based on the demographic and cultural specifications of the target community. For example, while Petosa et al. have introduced a single sub-construct, namely self-reward, the associated behaviors with self-reward were assigned to the self-monitoring sub-construct. As the associated behaviors with self-reward are a subdivision of self-communication skills, it is also associated with social and cultural specifications of different communities, which could contribute to the number of the items selected by the expert panel to measure self-reward-related behaviors in Iranian male adolescents.[39] In addition, the selection of the present questionnaire's items with the assistance of expert panel was made in such a way that led to elimination of relapse prevention and time management sub-constructs. However, these two sub-constructs were already considered in Petosa's questionnaire.
Failure to implement the qualitative extraction of the items using the target population and estimate concurrent and predictive validity could be the most important limitation of the present study. However, use of a considerable number of the target population members (N = 603) was a strength of this study. In addition, division of Isfahan into three regions, privileged, semi-privileged, and sub-privileged, and enrollment of participants from all the regions could increase the generalizability of the findings.
CONCLUSION
Although the findings indicated that the 16-item questionnaire used in this study enjoyed satisfactory validity and reliability to measure physical activity-related self-regulation construct in leisure time of male adolescents in Iran, the reassessment of validity and reliability of the new instrument in this population and others, and assessment of concurrent and predictive validity with regard to other main constructs of socio-cognitive theory could be helpful.
ACKNOWLEDGMENTS
Hereby, we gratefully thank all the students, teachers, and principals of the high schools who cooperated with the research team by filling out the questionnaires. In addition, the expert panel is appreciated for revising and estimating the questionnaire's validity and the Research and Technology Deputy of Isfahan University of Medical Sciences is thanked for funding this research.
Footnotes
Source of Support: This article has been derived from a thesis for PhD degree on health education and promotion in Isfahan School of Public Health, which was supported by the Deputy of Research of Isfahan University of Medical Sciences, that its number is 391476.
Conflict of Interest: I guarantee that there is not any conflict of interest.
REFERENCES
- 1.Olsen J, Bertollini R, Victora C, Saracci R. Global response to non-communicable diseases-the role of epidemiologists. Int J Epidemiol. 2012;41:1219–20. doi: 10.1093/ije/dys145. [DOI] [PubMed] [Google Scholar]
- 2.Robbins LB, Pender NJ, Conn VS, Frenn MD, Neuberger GB, Nies MA, et al. Physical activity research in nursing. J Nurs Scholarsh. 2001;33:315–21. doi: 10.1111/j.1547-5069.2001.00315.x. [DOI] [PubMed] [Google Scholar]
- 3.Allender JA, Spradley BW. Community Health Nursing: Promoting and Protecting the Public Health. 6th ed. Philadeelphia: Lippincott, Williams and Wilkins; 2005. p. 19. [Google Scholar]
- 4.Hamel LM, Robbins LB, Wilbur J. Computer- and web-based interventions to increase preadolescent and adolescent physical activity: A systematic review. J Adv Nurs. 2011;67:251–68. doi: 10.1111/j.1365-2648.2010.05493.x. [DOI] [PubMed] [Google Scholar]
- 5.Kelishadi R, Ghatrehsamani S, Hosseini M, Mirmoghtadaee P, Mansouri S, Poursafa P. Barriers to physical activity in a population-based sample of children and adolescents in Isfahan, Iran. Int J Prev Med. 2010;1:131–7. [PMC free article] [PubMed] [Google Scholar]
- 6.Physical Activity Facts. [Last accessed on 2014 Apr 12]. Available from: http://www.cdc.gov/healthyyouth/physicalactivity/facts.htm .
- 7.Adams MA, Johnson WD, Tudor-Locke C. Steps/day translation of the moderate-to-vigorous physical activity guideline for children and adolescents. Int J Behav Nutr Phys Act. 2013;10:49. doi: 10.1186/1479-5868-10-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sepanlou SG, Kamangar F, Poustchi H, Malekzadeh R. Reducing the burden of chronic diseases: A neglected agenda in Iranian health care system, requiring a plan for action. Arch Iran Med. 2010;13:340–50. [PubMed] [Google Scholar]
- 9.Taymoori P, Rhodes RE, Berry TR. Application of a social cognitive model in explaining physical activity in Iranian female adolescents. Health Educ Res. 2010;25:257–67. doi: 10.1093/her/cyn051. [DOI] [PubMed] [Google Scholar]
- 10.Pirasteh A, Hidarnia A, Asghari A, Faghihzadeh S, Ghofranipour F. Development and validation of psychosocial determinants measures of physical activity among Iranian adolescent girls. BMC Public Health. 2008;8:150. doi: 10.1186/1471-2458-8-150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Norman A, Bellocco R, Vaida F, Wolk A. Total physical activity in relation to age, body mass, health and other factors in a cohort of Swedish men. Int J Obes Relat Metab Disord. 2002;26:670–5. doi: 10.1038/sj.ijo.0801955. [DOI] [PubMed] [Google Scholar]
- 12.Lim K, Taylor L. Factors associated with physical activity among older peopl-a population-based study. Prev Med. 2005;40:33–40. doi: 10.1016/j.ypmed.2004.04.046. [DOI] [PubMed] [Google Scholar]
- 13.Peters JC, Wyatt HR, Donahoo WT, Hill JO. From instinct to intellect: The challenge of maintaining healthy weight in the modern world. Obes Rev. 2002;3:69–74. doi: 10.1046/j.1467-789x.2002.00059.x. [DOI] [PubMed] [Google Scholar]
- 14.Navalpotro L, Regidor E, Ortega P, Martinez D, Villanueva R, Astasio P. Area-based socioeconomic environment, obesity risk behaviours, area facilities and childhood overweight and obesity: Socioeconomic environment and childhood overweight. Prev Med. 2012;55:102–7. doi: 10.1016/j.ypmed.2012.05.012. [DOI] [PubMed] [Google Scholar]
- 15.Karoly P. Mechanisms of self-regulation: A systeme view. Annu Rev Psychol. 1993;44:23–52. [Google Scholar]
- 16.Rajati F, Mostafavi F, Sharifirad G, Sadeghi M, Tavakol K, Feizi A, et al. A theory-based exercise intervention in patients with heart failure: A protocol for randomized, controlled trial. J Res Med Sci. 2013;18:659–67. [PMC free article] [PubMed] [Google Scholar]
- 17.Schmid-Mohler G, Fehr T, Witschi P, Albiez T, Biotti B, Spirig R. Development of an evidence-based self-management programme for patients in the first year after renal transplantation with a focus on prevention of weight gain, physical exercise and drug adherence. Pflege. 2013;26:191–205. doi: 10.1024/1012-5302/a000291. [DOI] [PubMed] [Google Scholar]
- 18.Viswanath K. Models of Interpersonal health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior and Health Education: Theory, Research, and Practice. 4th ed. San Francisco: Jossey-Bass; 2008. pp. 170–88. [Google Scholar]
- 19.Miller LM, West RL. The effects of age, control beliefs, and feedback on self-regulation of reading and problem solving. Exp Aging Res. 2010;36:40–63. doi: 10.1080/03610730903418380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yeom HA, Fleury J. Validity and reliability of the index of self-regulation scale for physical activity in older Korean Americans. Nurs Res Pract. 2011;2011:329534. doi: 10.1155/2011/329534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dishman RK, Motl RW, Sallis JF, Dunn AL, Birnbaum AS, Welk GJ, et al. Self-management strategies mediate self-efficacy and physical activity. Am J Prev Med. 2005;29:10–8. doi: 10.1016/j.amepre.2005.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Umstattd MR, Motl R, Wilcox S, Saunders R, Watford M. Measuring physical activity self-regulation strategies in older adults. J Phys Act Health. 2009;6(Suppl 1):S105–12. doi: 10.1123/jpah.6.s1.s105. [DOI] [PubMed] [Google Scholar]
- 23.Yeom HA, Choi M, Belyea M, Fleury J. Psychometric evaluation of the index of self-regulation. West J Nurs Res. 2011;33:268–85. doi: 10.1177/0193945910378854. [DOI] [PubMed] [Google Scholar]
- 24.Marques M, De Gucht V, Maes S, Gouveia MJ, Leal I. Psychometric properties of the Portuguese version of the treatment self-regulation questionnaire for physical activity (TSRQ - PA) Psychology, Community and Health. 2012;1:212–20. [Google Scholar]
- 25.Boynton P, Greenhalgh T. Hands-on guide to questionnaire research: Selecting, designing, and developing your questionnaire. BMJ. 2004;328:1312. doi: 10.1136/bmj.328.7451.1312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Saffari M, Shojeaizadeh D, Ghofranipour F, Heidarnia AR, Pakpour A. Health Education and Health Promotion Theories, Models and Methods. 1st ed. Tehran: Asare Sobhan; 1388. pp. 100–12. [Google Scholar]
- 27.Reis MS, Reis RS, Hallal PC. Validity and reliability of a physical activity social support assessment scale. Rev Saude Publica. 2011;45:294–301. doi: 10.1590/s0034-89102011000200008. [DOI] [PubMed] [Google Scholar]
- 28.Keele R. Development of the exercise motivation questionnaire with Mexican American adults. J Nurs Meas. 2009;17:183–94. doi: 10.1891/1061-3749.17.3.183. [DOI] [PubMed] [Google Scholar]
- 29.van de Steeg N, Sielk M, Pentzek M, Bakx C, Altiner A. Drug-adherence questionnaires not valid for patients taking blood-pressure-lowering drugs in a primary health care setting. J Eval Clin Pract. 2009;15:468–72. doi: 10.1111/j.1365-2753.2008.01038.x. [DOI] [PubMed] [Google Scholar]
- 30.Nastaran M, Abolhasani F, Izadi M. Application of taps technique for analysis and prioritize sustainable urban development. Environmental Geography and Planning Journal. 1389;38:83–10. [Google Scholar]
- 31.Shirazi KK, Wallace LM, Niknami S, Hidarnia A, Torkaman G, Gilchrist M, et al. A home-based, transtheoretical change model designed strength training intervention to increase exercise to prevent osteoporosis in Iranian women aged 40-65 years: A randomized controlled trial. Health Educ Res h. 2007;22:305–17. doi: 10.1093/her/cyl067. [DOI] [PubMed] [Google Scholar]
- 32.Moini B, Jalilian F, Jalilian M, Barati M. Predicting factors associated with regular physical activity among college students applying BASNEF model. Scientific Journal of Hamadan University of Medical Sciences. 2010;18:70–6. [Google Scholar]
- 33.Moghaddam MH, Aghdam FB, Jafarabadi MA, Allahverdipour H, Nikookheslat SD, Safarpour S. The Iranian version of international physical activity questionnaire (IPAQ) in Iran: Content and construct validity, factor structure, internal consistency and stability. World Appl Sci J. 2012;18:1073–80. [Google Scholar]
- 34.Hajizadeh E, Asghari M. Statistical Methods and Analyses in Health and Biosciences. 1st ed. Tehran: Jahade Daneshgahi; 2010. pp. 399–401. [Google Scholar]
- 35.Lawshe CH. A quantitative approach to content validity. Pers Psychol. 1975;28:563–75. [Google Scholar]
- 36.Yaghmai F. Content validity and its estimation. J Med Educ. 2003;3:25–7. [Google Scholar]
- 37.Petosa PS. Use of Social Cognitive Theory to Explain Exer-Cise Behavior among Adults. Ohio, USA: The Ohio State University; 1993. pp. 295–309. [Google Scholar]
- 38.Fleury J. The index of self-regulation: Development and psychometric analysis. J Nurs Meas. 1998;6:3–17. [PubMed] [Google Scholar]
- 39.Glen Mick D, Demoss M. Self gift: Phenomenological insight from four contexts. J Consum Res. 1990;17:10. [Google Scholar]