

Abstract
Context:
Accidental root canal perforations are among the main complications of endodontic treatment.
Aim:
This study evaluated the influence of operating microscope (OM) in the marginal adaptation of mineral trioxide aggregate (MTA) (Angelus®) and glass ionomer (Vitremer) inserted into cervical perforations.
Materials and Methods:
Perforations were made in the cervical third of the buccal wall of the root canal in mandibular incisors. Next, the teeth were divided into four groups (N = 10): MG — MTA without OM; VG — Vitremer without OM; MOMG — MTA with OM; VOMG — Vitremer with OM. The perforations were sealed according to the group and the teeth were prepared for analysis by confocal laser scanning microscope. Images of perforation region (1,024×) were made and the gap presented by the materials was measured using the Image J program. LEXT OLS4100 three dimensional (3D) measuring laser microscope measured the volumetric misfit. Data of gap were analyzed by Kruskal-Wallis and Dunn's tests. Analysis of variance (ANOVA) and Tukey's tests compared the volumetric misfits.
Results:
The results showed lower volume and gap in the interface dentin/material in VOMG compared to the other groups (P < 0.05).
Conclusion:
The use of OM improved the quality of cervical perforations sealed with Vitremer, being indicated in clinical situations of iatrogenic cervical perforations.
Keywords: Confocal laser scanning microscopy (CLSM), glass ionomer, mineral trioxide aggregate (MTA), operating microscope (OM)
INTRODUCTION
Accidental root canal perforations are among the main complications of endodontic treatment, resulting in loss of integrity of root and adjacent periodontal tissues.[1] The perforation location along the root surface is fundamental for the prognosis. Cervical perforations that occur relatively close to the crestal bone and epithelial attachment may have a critical prognosis despite favourable visualization. This is attributed to bacterial contamination from the oral environment along the gingival sulcus, which delayes the repair process.[2]
Light-cured glass ionomer cement (GIC) is a hybrid bioactive adhesive restorative material that bonds to dentin and releases fluoride, helping remineralization and biocompatibility.[3,4] Its capability to adhere to dentin is the differential when compared to other materials. It occurs due to its better flow[5] and higher thermal expansion coefficient.[4] When compared to chemically activated GIC, the light-cured GIC presented better results to seal furcal perforations.[5] These findings are justified by clinical limitations of chemically activated GIC, including long setting time, dehydration during initial setting, and rough surface texture.[6]
Mineral trioxide aggregate (MTA) was developed with a specific aim of sealing communications between tooth and external surfaces. Its biocompatibility and ability to set in contact with moisture are favorable features to promote good seal when used at root perforations.[7,8]
Considering the necessity for better visualization of anatomical structures during endodontic treatments, magnification and luminosity become important. The use of clinical operating microscope (OM) provides a magnification up to 20 times that helps in locating calcified canals, identifying root canal perforations, detecting microfractures, identifying isthmuses, interpreting root canal system complexities, removing intraradicular posts and fractured instrument removal.[9,10]
The influence of using OM in the quality of material investigation has been little investigated to date. Different methods were used to study marginal adaptation of materials in perforations. Dye penetration is the most commonly employed method[11,12,13,14] and the confocal laser scanning microscopy (CLSM) is an alternative method that provides a volumetric evaluation.[15]
The aim of the present study was to analyze, in the CLSM, the influence of OM on the quality of marginal adaptation of a light-cured GIC (Vitremer, 3M ESPE, Minesota, USA) and MTA Angelus (Angelus Soluções Odontológicas, Londrina, Brazil).
MATERIALS AND METHODS
The study was reviewed and approved by the Research Ethics Committee of the University Federal of Rio Grande do Sul (UFRGS). Forty human single-canal mandibular incisors were selected.
Coronal access was performed with a high-speed handpiece with a round diamond point (1012HL, KG Sorensen, São Paulo, Brazil). After, the teeth were fixed vertically, with the cementoenamel junction (CEJ) aligned, on a metal base and cervical perforations were prepared with 1012HL point on a high-speed handpiece coupled to a parallelometer in order to standardize the position of communication. The point was triggered at 45° angled relative to the tooth long axis toward the buccal wall of the root canal, 3 mm below the CEJ, until the wall was disrupted.
Then, the specimens were randomly divided into four experimental groups (N = 10), according to the material used to seal the cervical perforation and according to the use of OM (Alliance Comercial São Carlos LTDA, São Carlos, SP, Brazil) under 10× magnification. The groups were as follows: MG — MTA (Angelus®) (Londrina-PR, Brazil) without OM; VG — Vitremer (3M ESPE, Minesota, USA) without OM; MOMG — MTA (Angelus®) (Londrina-PR, Brazil) with OM; VOMG — Vitremer (3M ESP Minesota, EUA) with OM.
To seal perforations, the teeth were fixed with wax (Clássico, São Paulo-SP, Brazil) in an endodontic dummy (Prodens, São Gonçalo-RJ, Brazil). The wax covered the whole root including the perforation area. For MG and MOMG, MTA was prepared according to the manufacturer's instructions and placed in the perforation area, using a MTA dispenser (Angelus®, Londrina-PR, Brasil), and compressed into cavity with a condenser (Duflex; SS White Artigos Dentários Ltda). For VG and VOMG, initially, using a microbrush (Microbrush, KG Sorensen, Cotia - SP, Brazil), the primer was applied during 30 s, dried with compressed air at a distance of 10 cm for 15 s and light cured for 20 s. Then, Vitremer powder and liquid were mixed according the manufacturer's instructions, placed in the perforation area, using a Centrix injector (DFL indústria e coméricio, Jacarépagua - RJ, Brazil), and light cured for 40 s.
After the sealing procedure, the teeth were removed from the endodontic dummy and stored at 37°C (±1) in 95% (±5) humidity, until the preparation of the specimens for analysis in the CLSM.
Each specimen was horizontally sectioned under water cooling, using a cut machine (Extec Labcut 1010, Enfield, CT) at 2 mm bellow CEJ and 1 mm below the end of perforation, resulting in a 3.5 mm length fragment that included the perforation area. Next, the perforation surfaces were polished with 30 μm granulation aluminum oxide paste (Arotec, Cotia, SP, Brazil) to produce a highly reflective surface. To remove any residues present on the polished surface, the samples were immersed in distilled water, activated in an ultrasonic cleaner (Cristófoli, Campo Mourão, PR, Brazil) during 10 min and dried with absorbent paper. All prepared surfaces were conditioned with phosphoric acid 37% (Condac 37; FGM Produtos Odontológicos Ltda., Joinville, SC, Brazil), for 5 min and, then, were washed with 50 mL of distilled water, dehydrated, and fixed individually on a glass slide.
The specimens were analyzed under a CLSM (LEXT OLS4100; Olympus, Shinjuku-ku, Tokyo, Japan). A blind operator using the depth-tracking tool in the CLSM calculated the volume of material-free areas. Initially, the position of the greater depth extension of the gap was identified. Then, eight scans in equidistant points on the perimeter of the perforation were done and the total volume of material-free area were calculated at each point with the following formula: π × r2 × (misfit depth)/3. The sum of the eight values was calculated to obtain the total misfit volume.
To evaluate marginal adaptation of materials, one image of each sample was acquired and saved using specific software (Olympus Stream; Olympus, Shinjuku-ku, Tokyo, JP), with magnification of 1,024×. Then, a blind operator, using Image J software (Toronto, ON, Canada), calibrated in micrometers (μm), measured the gap areas in every 10 μm of dentin/material interface, in an extension of 100 μm.
Kruskal-Wallis and Dunn's post hoc tests evaluated marginal adaptation differences among groups. One-way analysis of variance (ANOVA) and Tukey's post hoc tests compared data of volume misfit between groups. The significance level was set at .05 using Statistical Package for the Social Sciences (SPSS) (v18.0) software (IBM Corp, Somers, NY).
RESULTS
The results are summarized in Tables 1 and 2. Vitremer with OM group showed the smallest values of volume misfit and gap areas when compared to the other groups (P < 0.05). Figure 1 illustrates 3D images of interface dentin/material in the experimental groups.
Table 1.
Median (quartiles 25/75) of gap areas in experimental groups

Table 2.
Mean and standard deviation (μm3) of volume misfit in experimental groups

Figure 1.
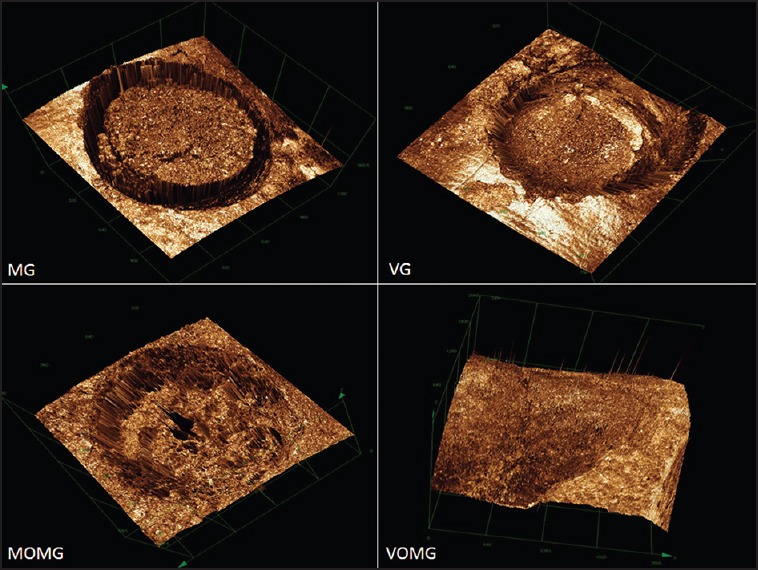
Images of the interface dentin/material in groups: MG (MTA without OM), VG (Vitremer without OM), MOMG (MTA with OM), and VOMG (Vitremer with OM) (1,024×)
DISCUSSION
During coronal access, an error in the inclination of the drill may determine a lateral or, at multirradicular teeth, a furcal perforation.[3] Inflammation may occur on adjacent periodontal tissue, resulting in insertion and bone loss.[2,16] However, few studies have been conducted to investigate alternatives of lateral perforation treatment. Thus, the present study contributed on the influence of a modern equipment recently introduced in endodontic clinic and about the materials indicated to seal lateral cervical perforations.
The use of OM influenced significantly the quality of marginal adaptation of GIC. This feature has been used in endodontics in order to minimize the obscurity of the operative field. It provides high magnification and brightness, facilitating the procedures performed. Thus, it favors the higher quality of therapeutic procedures, with significant increase in success rate.[17]
It is well known that the use of the OM favors visualization of anatomical structures of the root apex when used to perform surgical procedures involving periapical region. In those cases, the OM makes the prognosis more predictable. The use of this feature in nonsurgical endodontic procedures is increasing, especially for coronal access, root canals location, removal of fractured instruments, and detection of fractures.[18] In the present study, the magnification facilitated the insertion of materials in lateral cervical perforations, favoring GIC marginal adaptation into the cavity.
The most commonly used materials for sealing perforation are amalgam, zinc oxide-eugenol cement, IRM®, Super-EBA®, GIC, composite resin, Sealapex®, and MTA. Some authors compared these materials for the treatment of apical and furcal perforation and as root-end filling material.[14,15,19] More recently, Biodentine and calcium-enriched mixture (CEM) cement have been suggested to seal perforations.[20,21] In cases of lateral cervical perforation the chosen material to seal this communication will be in direct contact with periodontal ligament, so it's important to be aesthetic and allow final polishing.[22]
The results of this investigation showed better marginal adaptation to Vitremer when inserted in cavities using OM. This can be justified by the good properties of GIC such as good adhesion to dentin by the formation of a chemical bond with calcium ions of dentin[2] and ease of insertion.[23] Moreover, the good flow of light-cured GIC causes a better adaptation to dentin walls, helping the quality of sealing.[3] In addition, the coefficient of thermal expansion between tooth structure and the GIC provides good marginal sealing, low infiltration, and a high retention rate.[4] Therefore, the GIC is an alternative in cases of perforation, mainly when located in the cervical region, where restorative materials have been indicated.[13]
Despite its excellent biological properties, MTA has the worst marginal adaptation when inserted in cavities using OM. Some characteristics of this material, such as prolonged setting time,[24] which would allow displacement forces on the material to occur in the first hours after insertion, and prevent of its adaptation to dentin,[25] could have contributed to that result. Besides, according to the manufacturer's instructions, MTA needs to be in contact with a damp cotton pellet during 3-4 h, in order to set.[25] Moreover, the cervical lateral perforation site hampers the access of the condenser to MTA, hindering an adequate compression of the material in the cavity after its insertion with MTA dispenser.
In contrast to the findings of the present investigation, some authors found better marginal adaptation and sealing ability for MTA and Biodentine when compared to GIC.[4,15,26] However, such investigations had evaluated these materials to seal furcal perforations and as root-end filling material.
Literature reported cases of lateral perforation treatment with MTA[27] and GIC,[22] both with satisfactory clinical follow-up for 36 months. Despite the satisfactory results for both materials, these findings could not be compared with the present investigation as they refer to case reports while this investigation employed an in vitro model.
The experiment of Mannocci and[11] Vitremer had the highest rate of leakage when compared to amalgam, IRM, and Bilfill. Furthermore, Tanomaru-Filho[13] had observed satisfactory and similar sealing ability to Vitremer and MTA (Angelus®). It is important to point out that in both studies the marginal adaptation was macroscopically evaluated by 2% methylene blue penetration. This dye penetration method has several limitations, including the dissolution of the dye during the process and difficulty in observing the maximum depth penetration.[12]
With advances in technology, the use of the CLSM allows to analyze marginal adaptation with greater precision. It is a noninvasive method, thus permitting the preservation of samples. The CLSM allowed better visualization of the interface dentin/sealer material and evaluation of the misfit in sections of 100 mm. The main advantage of this method is the capacity to produce sequential images in a defined plan, improving contrast and definition of scanned images when compared to traditional microscopic techniques that can generate artifacts in the images due to physical cuts.[15]
As in the present study, Ravichandra[15] also evaluated sealing materials (GIC, MTA, and Biodentine) marginal adaptation. The authors observed lower marginal adaptation to GIC. However, the materials were used to seal apical perforations, OM was not used for insertion of materials and the rhodamine blue dye stained area was measured by the CLSM to evaluate marginal adaptation. In the present investigation, marginal adaptation was analyzed by measuring gap areas and total misfit volume, providing more accurate results.
CONCLUSION
Considering the method and results obtained, it was concluded that the use of OM improved the quality of cervical perforations sealed with Vitremer, being indicated in clinical situations of iatrogenic cervical perforations occurring during endodontic access.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors deny any conflicts of interest. We affirm that we have no financial affiliation (e.g., employment, direct payment, stock holdings, retainers, consultantships, patent licensing arrangements, or honoraria), or involvement with any commercial organization with direct financial interest in the subject or materials discussed in this manuscript, nor have any such arrangements existed in the past 3 years. Any other potential conflict of interest is disclosed.
REFERENCES
- 1.Shahi S, Rahimi S, Hasan M, Shiezadeh V, Abdolrahimi M. Sealing ability of mineral trioxide aggregate and Portland cement for furcal perforation repair: A protein leakage study. J Oral Sci. 2009;51:601–6. doi: 10.2334/josnusd.51.601. [DOI] [PubMed] [Google Scholar]
- 2.Main C, Mirzayan N, Shabahang S, Torabinejad M. Repair of root perforations using mineral trioxide aggregate: A long-term study. J Endod. 2004;30:80–3. doi: 10.1097/00004770-200402000-00004. [DOI] [PubMed] [Google Scholar]
- 3.Alhadainy HA, Himel VT. An in vitro evaluation of plaster of Paris barriers used under amalgam and glass ionomer to repair furcation perforations. J Endod. 1994;20:449–52. doi: 10.1016/S0099-2399(06)80036-1. [DOI] [PubMed] [Google Scholar]
- 4.Abd El Halim S, Zaki D. Comparative evaluation of microleakage among three different glass ionomer types. Oper Dent. 2011;36:36–42. doi: 10.2341/10-123-LR. [DOI] [PubMed] [Google Scholar]
- 5.Alhadainy HA, Himel VT. Comparative study of the sealing ability of light-cured versus chemically cured materials placed into furcation perforations. Oral Surg Oral Med Oral Pathol. 1993;76:338–42. doi: 10.1016/0030-4220(93)90264-5. [DOI] [PubMed] [Google Scholar]
- 6.Bona AD, Pinzetta C, Rosa V. Microleakage of acid etched glass ionomer sandwich restorations. J Min Interv Dent. 2009;2:36–43. [Google Scholar]
- 7.Yoshimine Y, Ono M, Akamine A. In vitro comparison of the biocompatibility of mineral trioxide aggregate, 4META/MMA-TBB resin, and intermediate restorative material as root-end-filling materials. J Endod. 2007;33:1066–9. doi: 10.1016/j.joen.2007.05.006. [DOI] [PubMed] [Google Scholar]
- 8.Al-Daafas A, Al-Nazhan S. Histological evaluation of contaminated furcal perforation in dogs’ teeth repaired by MTA with or without internal matrix. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:e92–9. doi: 10.1016/j.tripleo.2006.09.007. [DOI] [PubMed] [Google Scholar]
- 9.Rubinstein R. Magnification and illumination in apical surgery. Endod Topics. 2005;11:56–77. [Google Scholar]
- 10.Kersten DD, Mines P, Sweet M. Use of the microscope in endodontics: Results of a questionnaire. J Endod. 2007;34:804–7. doi: 10.1016/j.joen.2008.04.002. [DOI] [PubMed] [Google Scholar]
- 11.Mannocci F, Vichi A, Ferrari M. Sealing ability of several restorative materials used for repair of lateral root perforations. J Endod. 1997;23:639–41. doi: 10.1016/S0099-2399(97)80178-1. [DOI] [PubMed] [Google Scholar]
- 12.Tamse A, Katz A, Kablan F. Comparison of apical leakage shown by four different dyes with two evaluating methods. Int Endod J. 1998;31:333–7. [PubMed] [Google Scholar]
- 13.Tanomaru-Filho M, Faleiros FC, Tanomaru JM. Sealing ability of materials used in root lateral perforations. Rev Fac Odontol Lins. 2002;14:40–3. [Google Scholar]
- 14.Daoudi MF, Saunders WP. In vitro evaluation of furcal perforation repair using mineral trioxide aggregate or resin modified glass ionomer cement with and without the use of the operating microscope. J Endod. 2002;28:512–5. doi: 10.1097/00004770-200207000-00006. [DOI] [PubMed] [Google Scholar]
- 15.Ravichandra PV, Vemisetty H, Deepthi K, Reddy JS, Ramkiran D, Krishna JN, et al. Comparative evaluation of marginal adaptation of biodentine™ and other commonly used root end filling materials — An in vitro study. J Clin Diagn Res. 2014;8:243–5. doi: 10.7860/JCDR/2014/7834.4174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bargholz C. Perforation repair with mineral trioxide aggregate: A modified matrix concept. Int Endod J. 2005;38:59–69. doi: 10.1111/j.1365-2591.2004.00901.x. [DOI] [PubMed] [Google Scholar]
- 17.Lins CC, Silva EM, De Lima GA, Menezes SE, Travassos RM. Operating microscope in endodontics: A systematic review. Open J Stomatol. 2013;3:1–5. [Google Scholar]
- 18.García Calderín M, Torres Lagares D, Calles Vázquez C, Usón Gargallo J, Gutiérrez Pérez JL. The application of microscopic surgery in dentistry. Med Oral Patol Oral Cir Bucal. 2007;12:E311–6. [PubMed] [Google Scholar]
- 19.Song M, Kim E. A prospective randomized controlled study of mineral trioxide aggregate and super ethoxy-benzoic acid as root-end filling materials in endodontic microsurgery. J Endod. 2012;38:875–9. doi: 10.1016/j.joen.2012.04.008. [DOI] [PubMed] [Google Scholar]
- 20.Nazari Moghadam K, Aghili H, Rashed Mohassel A, Zahedpasha S, Moghadamnia AA. A comparative study on sealing ability of mineral trioxide aggregate, calcium enriched cement and bone cement in furcal perforations. Minerva Stomatol. 2014;63:203–10. [PubMed] [Google Scholar]
- 21.Sinkar RC, Patil SS, Jogad NP, Gade VJ. Comparison of sealing ability of ProRoot MTA, RetroMTA, and Biodentine as furcation repair materials: An ultraviolet spectrophotometric analysis. J Conserv Dent. 2015;18:445–8. doi: 10.4103/0972-0707.168803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dragoo MR. Resin ionomer and hybrid-ionomer cements: Part I. Comparison of three materials for the treatment of subgingival root lesions. Int J Periodontics Restorative Dent. 1996;16:595–601. [PubMed] [Google Scholar]
- 23.Chong BS, Pitt Ford TR, Watson TF. The adaptation and sealing ability of light-cured glass ionomer retrograde root fillings. Int Endod J. 1991;24:223–32. doi: 10.1111/j.1365-2591.1991.tb01148.x. [DOI] [PubMed] [Google Scholar]
- 24.Grazziotin-Soares R, Nekoofar MH, Davies TE, Bafail A, Alhaddar E, Hübler R, et al. Effect of bismuth oxide on white mineral trioxide aggregate: Chemical characterization and physical properties. Int Endod J. 2014;47:520–33. doi: 10.1111/iej.12181. [DOI] [PubMed] [Google Scholar]
- 25.Tsesis I, Fuss Z. Diagnosis and treatment of accidental root perforations. Endo Topics. 2006;13:95–107. [Google Scholar]
- 26.Xavier CB, Weismann R, de Oliveira MG, Demarco FF, Pozza DH. Root-end filling materials: Apical microleakage and marginal adaptation. J Endod. 2005;31:539–42. doi: 10.1097/01.don.0000152297.10249.5a. [DOI] [PubMed] [Google Scholar]
- 27.Yildirim G, Dalci K. Treatment of lateral root perforation with mineral trioxide aggregate: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:e55–8. doi: 10.1016/j.tripleo.2006.04.001. [DOI] [PubMed] [Google Scholar]