

Abstract
Background
There is substantial interest in the effects of nutrition labels on consumer food-purchasing behavior. However, conducting randomized controlled trials on the impact of nutrition labels in the real world presents a significant challenge.
Objective
The Food Label Trial (FLT) smartphone app was developed to enable conducting fully automated trials, delivering intervention remotely, and collecting individual-level data on food purchases for two nutrition-labeling randomized controlled trials (RCTs) in New Zealand and Australia.
Methods
Two versions of the smartphone app were developed: one for a 5-arm trial (Australian) and the other for a 3-arm trial (New Zealand). The RCT protocols guided requirements for app functionality, that is, obtaining informed consent, two-stage eligibility check, questionnaire administration, randomization, intervention delivery, and outcome assessment. Intervention delivery (nutrition labels) and outcome data collection (individual shopping data) used the smartphone camera technology, where a barcode scanner was used to identify a packaged food and link it with its corresponding match in a food composition database. Scanned products were either recorded in an electronic list (data collection mode) or allocated a nutrition label on screen if matched successfully with an existing product in the database (intervention delivery mode). All recorded data were transmitted to the RCT database hosted on a server.
Results
In total approximately 4000 users have downloaded the FLT app to date; 606 (Australia) and 1470 (New Zealand) users met the eligibility criteria and were randomized. Individual shopping data collected by participants currently comprise more than 96,000 (Australia) and 229,000 (New Zealand) packaged food and beverage products.
Conclusions
The FLT app is one of the first smartphone apps to enable conducting fully automated RCTs. Preliminary app usage statistics demonstrate large potential of such technology, both for intervention delivery and data collection.
Trial Registration
Australian New Zealand Clinical Trials Registry ACTRN12614000964617. New Zealand trial: Australian New Zealand Clinical Trials Registry ACTRN12614000644662.
Keywords: randomized controlled trial, smartphone, public health, nutrition labeling
Introduction
Smartphone technology offers promising new ways to deliver health interventions and undertake research [1], and smartphone-assisted randomized controlled trials (RCTs) are an emerging methodology. The role of smartphone technology in RCTs varies from provision of simple information or text message reminders to participants to more complex tools enabling, for example, self-monitoring or data collection [2-4]. Messages have been the most common tool used in smartphone-assisted studies to date, although specialized smartphone apps are increasing in popularity [5]. Although systematic reviews suggest mixed evidence of the effectiveness of smartphone-delivered health interventions compared to traditional methods [6,7], advantages of such programs include ability to deliver an intervention remotely and a potentially wider population reach. Greater participant retention and adherence to the intervention and improved convenience for participants compared to traditional methods have also been reported for smartphone-assisted interventions [2,8,9].
Most smartphone RCTs to date have been only partially technology-assisted, that is, smartphone technology is used as an add-on to an existing behavior change program or an automated intervention is compared with a standard technology-free control group [3,10]. Automated RCTs conducted entirely via a smartphone app are a novel approach in health research, and thus, limited published data are currently available in this field. To date, we are aware of only 1 other RCT (a smoking cessation app) that used this approach [11].
Here we describe a new smartphone app developed for use in automated RCTs on the effects of different nutrition label formats on the healthiness of consumer food purchases in 2 countries (Australia and New Zealand) [12,13]. The app (Food Label Trial, FLT) was designed to overcome 2 common challenges of nutrition-labeling interventions: (1) delivery of various nutrition label formats for foods in real-world supermarkets (the intervention) and (2) collection of reliable, objective, household-level food shopping data.
Although the potential public health benefits of interpretive, easy-to-understand nutrition labels are generally accepted [14], it is difficult to test the effectiveness of such labels as an intervention in real-world retail settings. Therefore, assessment of their effectiveness is often only possible in controlled settings [15] or in nonrandomized natural experiments [16]. Technology used in the FoodSwitch smartphone app [17], available in Australia and New Zealand, enables delivery of nutritional information via digital nutrition labels. FoodSwitch users place their smartphone camera over the barcode of a packaged food, the unique barcode is then matched with a product in the underlying food database, and an interpretive nutrition label for the scanned product is displayed on screen. The intervention delivery mode of the FLT app uses the same technology to deliver a nutrition-labeling intervention to trial participants.
A second challenge is collection of individual-level data on food purchases. Traditional methods involve collection of itemized food shopping receipts. However, this requires manual coding and data entry, which is time-consuming and resource intensive [18-20]. Other ways of recording individual purchases, for example, via barcode scanners [21], have also been explored but have presented limitations such as the need for additional equipment or being limited to specific participating stores. To overcome this challenge, our RCT app was designed to have inbuilt data collection functionality using barcode scanning technology.
The aim of this paper is to describe the development and functionality of the smartphone app used for the trials, provide an overview of the end product, and report preliminary usage statistics and common technical issues.
Methods
Approvals
Both trials received appropriate ethics approvals (University of Sydney Human Research Ethics Committee, reference number 460; University of Auckland Human Participant Ethics Committee, reference number 011390).
Trial Overview
Full trial protocols, including aims, design, outcome measurements, and power calculations, have been previously published [12,13]. In summary, the randomized controlled trials aimed to assess the effects of different nutrition label formats on the healthiness of consumer food purchases. Individual food and beverage shopping data were collected during 5 weeks (1-week baseline and run-in and a 4-week intervention period). Eligible participants were randomized to 1 of 5 nutrition-labeling formats in Australia and 1 of 3 labeling formats in New Zealand (Figure 1): Daily Intake Guide [22] (Australian trial only), Traffic Light labels [23], Health Star Rating [24], Nutrition Information Panel (control) [25], or a Warning Label [13] (Australian trial only). Both intervention and control nutrition labels were delivered via the smartphone app to minimize technology bias.
Figure 1.
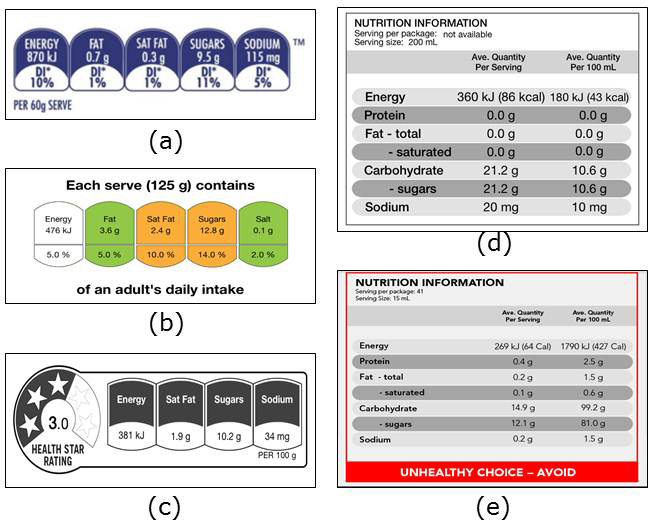
Nutrition-labeling formats allocated to intervention and control groups in the trials. (a) Daily Intake Guide*. (b) Traffic Lights. (c) Health Star Rating. (d) Nutrition Information Panel (control arm). (e) Warning Label*. *Australian trial only.
Development of the App
Key Requirements
The app had 3 key functionality requirements: (1) fully automating the conduct of RCTs [12,13], that is, consent, screening, randomization, and questionnaire administration; (2) delivering trial intervention, that is, nutrition labels; and (3) facilitating data collection.
The framework for the first function is presented in Figure 2 as a sequence of the key trial events. Progression through those events was determined by in-app and server-side checks, including an email address check to prevent duplicate registrations, a check that consent has been provided and terms and conditions have been accepted, eligibility at screening, and a check that at least 15 barcoded food or beverage items were recorded during week 1 (run-in phase requirement). A timeline check (from the moment of registration) was also required to ensure delivery of key events such as randomization (end of week 1) and the follow-up questionnaire (end of week 5).
Figure 2.
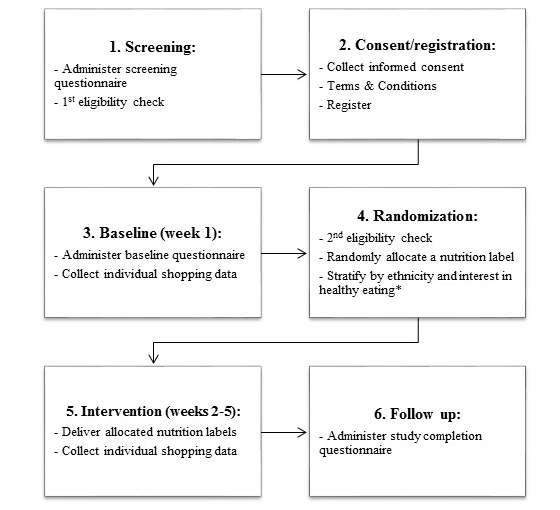
Sequence of the key trial events automatically delivered via the FLT mobile app. *New Zealand trial only.
Intervention delivery functionality provided users with a nutrition label for a scanned food product. The format of the label provided was determined by the participant’s randomization allocation (Figure 1). Designs of digital nutrition labels in the app were based on the relevant style guides [22-25]. Similar to the FoodSwitch app, nutrient content information for the scanned product was obtained by matching the barcode number with one from the food composition database at the back end.
Data collection functionality used barcode scanning to create electronic itemized records of food purchases made by participants, and the smartphone camera was used to photograph the till receipts. Participants were requested to record all food purchases during the 5-week trial period. Additional information on demographics and usual shopping patterns was collected via in-app baseline and follow-up questionnaires. Two in-app tutorials were developed for user training purposes. In-app and push notifications and reminders were developed to prompt user engagement and adherence to the trial protocol and timelines. The following ethical and security requirements were adhered to: (1) A participant information statement was available to participants via the app throughout the trial, and (2) all data collected via the app were stored securely with identifiable information stored separately from trial outcome data.
Two similar versions of the FLT app were created for the Australian and New Zealand RCTs, with the following differences between the apps for the two countries: (1) five intervention arms in the Australian app versus 3 for New Zealand; (2) different randomization algorithms with (New Zealand) or without (Australia) stratification by ethnicity and self-reported interest in healthy eating [12]; (3) Australian and New Zealand trial-specific participant information and consent statements, terms and conditions, logos, and content-management systems; and (4) country-specific back-end food composition databases.
Backend Food Composition Databases
Country-specific food composition databases provided the nutrient information to create nutrition labels and assess outcome measures. The Australian version of the app used The George Institute for Global Health’s FoodSwitch database [17], which currently contains nutrition information for more than 65,000 Australian packaged food items. The New Zealand version of the app used the NZ FoodSwitch database, which currently contains nutrition information for more than 21,000 products. The most up-to-date versions of the food composition datasets available at the time of app development were used.
Usability Evaluation
The initial decision on whether an FLT smartphone intervention was feasible to conduct in Australia and New Zealand was based on the popularity of the FoodSwitch app, which currently has more than 600,000 downloads in Australia (population 23.7 million in 2015) and 65,000 downloads in New Zealand (population 4.5 million in 2015). Because the FoodSwitch and FLT apps’ core functionality were very similar, separate usability evaluation was not deemed necessary for the FLT app.
Development and Testing
The app was designed by research teams at used The George Institute for Global Health, University of Sydney, Australia, and the National Institute for Health Innovation, University of Auckland, New Zealand. Software and interface development was led by Buzinga Apps, Australia. The app was developed for Android and iOS platforms, the most common smartphone platforms in Australia and New Zealand [17]. During the development period, weekly online conference meetings were held between the used The George Institute for Global Health, National Institute for Health Innovation, and Buzinga teams. The time frame for development was approximately 9 months, with the framework, interface, technical requirements, and algorithms being developed over the first 5 months (Jan-May 2014) and the iterative development and testing process implemented over the following 4 months (June-Sep 2014). All components of the FLT app and the final versions were pretested by the software developer and research teams. Final products, for both Android and iOS, were tested by independent volunteers from the same research institutions who were not involved in the project. Final versions of the FLT app were submitted to Apple and Android app stores in October 2014. The initial version of the app was compatible with smartphones running either iOS 7 and above or Android 4.3-4.4. The app was updated as new versions of the operating systems became available.
Data Management
All data collected via the FLT app were automatically transmitted to a trial database located on a remote server. Country-specific content management systems were developed for data processing, management, and extraction. Automatic in-app and server-side logic checks on the incoming data were used to ensure adherence to trial requirements and progress through the stages.
Technical Issue Management
On-going quality control of the collected data was carried out by research teams to identify any potential issues. Any identified issues were prioritized by the research team and addressed by Buzinga Apps based on the impact on trial data and the level of inconvenience to participants. Weekly meetings were held between researchers and the app development teams to ensure timely resolution of major technical problems. Two updates of the app for the Android platform and 1 for iOS platform were released after the initial app launch to provide fixes for identified issues.
Analysis of the App Usage
Data collected from the trial app between October 2014 and June 2015 were used for analyses and represent the first nine months of the trial. Simple descriptive statistics were used to report the number of downloads, registrations, randomizations, and the amount of individual shopping data collected via the app. The final trial completion rates will be reported in the results papers (the trials were ongoing at the time of drafting).
Results
Functionality Overview
A flowchart with sample screenshots is presented in Figure 3, and the 16 main functionality components of the FLT app are summarized in Table 1. The first event in the FLT app was the informed consent and registration process. All subsequent events were automatically triggered either by a task completion (eg, a questionnaire) or by reaching a key trial time point (eg, end of baseline phase after 1 week). The trial tutorials are available in the Multimedia Appendices 1 and 2. The logic and schedule of key reminder messages and notifications are summarized in Table 2. The messages were triggered either by the trial timelines or user’s progress on task completion.
Figure 3.
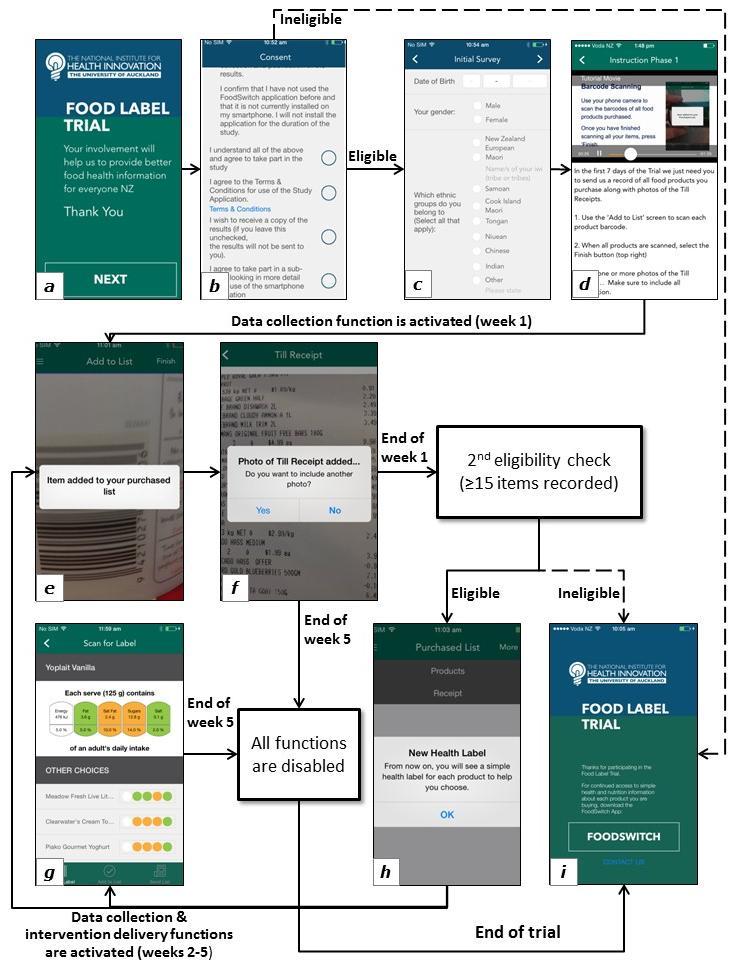
Food Label Trial app key functionality flowchart with sample screenshots (from the New Zealand version of the app). (a) Welcome screen. (b) Consent and terms and conditions screen. (c) Baseline questionnaire screen. (d) Tutorial. (e) Data collection mode: barcode scanning. (f) Data collection mode: adding a matching till receipt image. (g) Intervention delivery: traffic light label arm. (h) Postrandomization in-app notification. (i) End of trial screen, offering a link to the FoodSwitch app.
Table 1.
Main functions of the Food Label Trial app.
| Component | Time point | Description |
| Consent and T&Ca statement | User opens the app for the first time | On-screen consent statement with links to full PIS and T&C documents. Multichoice tick box answer options. Acceptance of the consent statement and T&C were mandatory. |
| Registration form | After screening questionnaire | Questions with free text answer options. A requirement to enter a unique email address. |
| Questionnaires | Screening: after consent Baseline: prior to week 1 Follow-up: end of week 5 |
Questions with multi-choice (tick-box or sliding scale) or free text answer options. |
| Eligibility checks | First: at screening Second: at the end of week 1 |
Eligibility was determined from the screening questionnaire answers (first check) and the number of products recorded during baseline (second check). |
| Randomization | End of week 1 | Server-side central blocked randomization with variable block sizes. |
| Barcode scanning | Weeks 1-5 | Barcode numbers of the scanned products were matched with an in-app backend food database. |
| Electronic lists of purchases | Weeks 1-5 | Automatically generated electronic list of scanned product items |
| Till receipt capture | Weeks 1-5 | Smartphone camera is engaged to photograph the till receipt images. |
| Intervention (nutrition label) delivery | Weeks 2-5 | For recognized products, a nutrition label was displayed. The label format was determined by the user’s randomization allocation. A random selection of other products from the same category was displayed under the label. |
| Crowdsourcing: missing product information | Weeks 2-5 | An optional functionality allowed users to submit photos of missing products (as with the crowdsourcing function of the FoodSwitch app [17]. |
| Tutorials | First: before week 1 Second: before week 2 |
Short in-app video clips introducing the app functionality and the required tasks. |
| Reminders and notifications | Throughout the trial | Automatically triggered in-app and push notification messages. The logic and schedule are described in Table 2. |
| Progress tracker | Weeks 1-5 | Showed the number of weeks completed on the trial. |
| History | Weeks 1-5 | A history of all previously sent electronic lists |
| Trial information | Weeks 1-5 | Information about the trial, research team and technical support contacts, PIS. |
| Link to FoodSwitch | Ineligible users, end of trial | A link to the FoodSwitch app offered as an alternative resource for healthy food choices. |
aPIS: participant information statement, T&C: terms and conditions.
Table 2.
Key notification and reminder messages delivered by the Food Label Trial app
| Message description | Trigger | Time point and frequency | Type |
| Notification informing of ineligibility for the trial; offered a link to the FoodSwitch app. | First eligibility check failed | Once after the screening questionnaire | In-app message |
| Reminder to complete the registration or baseline questionnaire | Registration form not completed | Two days after consent, then once a week up to 4 times, then once a month until 5 weeks before the overall trial recruitment completion | Push notification |
| Reminder to record at least 15 items during week 1 | User submitted a list of purchased products during week 1, and the total number of items recorded by the user to date is less than 15 | After every submitted list that meets the criteria | In-app message |
| Notification that the product list has been successfully sent | User submitted a list of purchased products, and it was successfully transmitted to the trial database. The number of products recorded during week 1 is 15 items or more | After every submitted list that meets the criteria | In-app message |
| Reminder to record food purchases (baseline phase) | User has not sent any product lists since the beginning of week 1 | At days 3 and 5 of week 1 | Push notification |
| Reminder to keep recording food purchases (intervention phase) | User has not been sending through any new product lists | At days 4, 6, 9, 12, 18, and 24 since the last product list was sent OR since the beginning of the intervention phase | Push notification |
| Reminder that the trial is ending soon | Day 26 of the intervention phase | Day 26 of the intervention phase | Push notification |
| Request to complete the follow-up questionnaire | Day 28 of the intervention phase | Day 28 of the intervention phase | In-app message |
| Reminder to complete the follow-up questionnaire | User has not completed the follow-up questionnaire | Days 6, 12, 18, 24, and 30 from completion of the intervention phase | Push notification |
| Notification of the trial completion | User completed the follow-up questionnaire | Once after the follow-up questionnaire | In-app message |
Preliminary App Usage Statistics
The FLT app usage statistics for the initial 13 months since the app launch are summarized in Figure 4 (October 2014-Nov 2015). In total, 3000 users downloaded the FLT app to undergo an eligibility check, and of these, close to 1500 unique users were randomized to receive the trial intervention. During this time, participants submitted close to 13,000 electronic shopping lists, with more than 150,000 individual food or beverage items and over 20,000 matching receipt images. The labeling intervention usage rates are reported in Figure 4 as a total number of “label views.”
Figure 4.
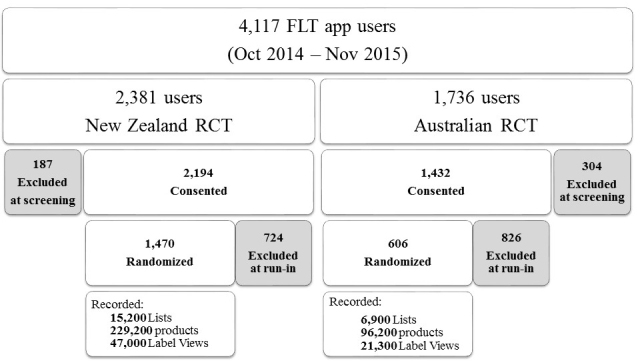
Food Label Trial app usage statistics for the period of October 2014-November 2015.
Key Technical Issues
The most common issues encountered were intermittent problems in connecting to the server while recording purchased products and reminder messages being sent very frequently. Other less-frequent issues, potentially caused by attempts to use the app on incompatible devices, included incorrect recording of consent status, problems viewing nutrition labels, registration issues, issues with focusing smartphone camera on barcodes during scanning, and multiple identical copies of baseline and follow-up surveys recorded for some users. A small number of users experienced issues accessing the trial intervention after the iOS 9.1 release in October 2015.
Discussion
The FLT app is a novel smartphone app designed to conduct an automated RCT on the effects of different nutrition labels on food purchases. To our knowledge, this is the first fully automated smartphone-based trial in public health nutrition. The use of the FLT app overcomes a major challenge commonly encountered in current nutrition-labeling interventions, that is, delivery of randomly allocated nutrition labels to study participants in their regular real-world food shopping locations. Previously, real-world effect of nutrition labels was assessed at a large scale in a natural experiment observation study [16]. Another large study used shelf-labeling in a selected chain of supermarkets [15]. However, a randomized controlled approach has not been possible, and as a result, the current trials are the first RCTs to measure the real-world effect of nutrition labels on food purchasing [26].
The FLT app enabled simplified collection of participant household food purchase data, automatically linked to demographic characteristics (via the participant ID number) and to the food database (via product barcodes). Compared to previous research in this area using shopping receipts as a primary data collection mode for food purchases [18-20], the FLT app substantially reduces the requirements for manual coding and data entry of packaged foods. To minimize potential bias due to technology influence, a control group nutrition label was also delivered via the smartphone, which replicates current mandatory nutrition labels found on the back of the pack of most food and beverage items in Australia and New Zealand.
Preliminary statistics of the FLT app usage have been promising; a large amount of data on intervention usage (label viewing) and individual food purchases has been collected to date. Completeness of electronic shopping data collected will be verified against the shopping receipts at the end of the trial. It will be useful to determine feasibility of this data collection approach in contest of the result of the studies using traditional grocery shopping receipt data collection methods [18].
Previous smartphone-assisted public health intervention trials have mainly focused on comparing the efficacy of technology-based intervention with traditional methods (eg, face-to-face behavior change consultations [3]). The described “smart” trials use a different approach: The FLT app is not just an intervention within a trial, but a platform enabling a fully automated RCT to be conducted. The app allows screening, consent, registration, and management of study participants remotely, without any manual input from the research team. Ethical and security requirements have also been considered during the app development, which is important, as previous systematic reviews have identified patient privacy as a potential area of concern when using smartphone technology [5].
This novel, “smart” RCT approach offers potential learning benefits for future trials, eliminating the need for in-person or telephone appointments and substantially reducing the time commitment for both researchers and trial participants. To date, limited data have been published on other trials using this approach. A study protocol by BinDhim et al [11] uses a similar “smart” RCT design. This smoking cessation trial also uses an app for screening, consenting, and randomizing trial participants, intervention delivery, and data collection. However, there are 2 key differences compared with the FLT app functionality. First, the FLT app provides a personalized intervention based on participants’ interactions with their environment, rather than delivering a generic intervention to all participants. Second, similar to the app used in the study by BinDhim et al [11], the FLT app passively records app usage and collects self-reported data via questionnaires. However, the FLT app also enables participants to actively record their food purchase data. This is of particular importance for a nutrition-labeling intervention, where there is a known shortage of outcomes based on objectively measured shopping data [27].
The FLT app design has certain limitations. Because of the relatively long duration of the projects (18 months recruitment period), it was necessary to update the app following the release of new versions of Android and Apple operating systems. Each app update required time for additional testing and resubmission to the app stores, and thus some users could experience issues with the app functionality until the update was finalized. In addition, because of the large range of smartphone devices available on the market, it was not possible to test compatibility with every one, and thus identify in advance device-specific issues. The issues affecting trial intervention delivery, such as barcode scanning or issues with producing nutrition labels, were considered of high importance for the trial, and thus were prioritized for fixing. The impact of data collection issues was partially offset by using backup data collection methods (hard copies of till receipts) [12,13]. The issues that affected the trial management process, such as very frequent reminders, created inconvenience for participants but had fewer implications for the trial outcomes.
Another limitation is that static backend food databases were used for the app. Therefore, new products appearing on the market after the app release were not recognized by the app. This may have affected both data collection and intervention delivery modes of the app, because both functions work by barcode identification within existing food databases. The impact on data collection can be managed by linking a complete trial dataset with an updated food database at a later time, and thus matching all previously unrecognized barcode numbers with new product information. However, the impact on the intervention delivery is greater, as participants cannot view nutrition labels for missing products.
Finally, the technology-based nature of the trial has a potential to contribute to sample selection bias. Although smartphone ownership is high in both Australia (up to 80% [28]) and New Zealand (up to 70% [29]), a range of factors, such as lack of an active Internet connection, may limit accessibility of some population groups to this research medium. Thus, generalizability of the smart RCT’s findings need to be further examined.
In conclusion, the FLT demonstrates the feasibility of using smartphone apps to undertake real-world nutrition-labeling interventions and enable easy collection of individualized electronic food purchasing data. The app technology allows immediate access to intervention nutrition labels in any real-world retail outlet and enables randomized comparison of the label effectiveness. The FLT app is among the first smartphone apps to enable conducting fully automated RCTs.
Acknowledgments
The Australian Food Label Trial was funded by a National Health & Medical Research Council Partnership Grant (App 1072047).
The New Zealand nutrition-labeling RCT was funded by a Health Research Council of New Zealand program grant (13/724).
Abbreviations
- RCT
Randomized controlled trial
- FLT
Food Label Trial
Food Label Trial app tutorial 1.
Food Label Trial app tutorial 2.
Footnotes
Conflicts of Interest: None declared.
References
- 1.WHO Global Observatory for eHealth Series - Volume 3: New Horizons for Health Through Mobile Technologies. 2011. [2015-04-14]. http://www.who.int/goe/publications/goe_mhealth_web.pdf .
- 2.Varnfield M, Karunanithi M, Lee C, Honeyman E, Arnold D, Ding H, Smith C, Walters DL. Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: Results from a randomised controlled trial. Heart. 2014 Nov;100(22):1770–9. doi: 10.1136/heartjnl-2014-305783. http://heart.bmj.com/cgi/pmidlookup?view=long&pmid=24973083 .heartjnl-2014-305783 [DOI] [PubMed] [Google Scholar]
- 3.Allen JK, Stephens J, Dennison Himmelfarb CR, Stewart KJ, Hauck S. Randomized controlled pilot study testing use of smartphone technology for obesity treatment. J Obes. 2013;2013:151597. doi: 10.1155/2013/151597. doi: 10.1155/2013/151597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Eyles H, McLean R, Neal B, Doughty RN, Jiang Y, Ni MC. Using mobile technology to support lower-salt food choices for people with cardiovascular disease: Protocol for the SaltSwitch randomized controlled trial. BMC Public Health. 2014;14:950. doi: 10.1186/1471-2458-14-950. http://www.biomedcentral.com/1471-2458/14/950 .1471-2458-14-950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Derbyshire E, Dancey D. Smartphone medical applications for women's health: What is the evidence-base and feedback? Int J Telemed Appl. 2013;2013:782074. doi: 10.1155/2013/782074. doi: 10.1155/2013/782074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Donker T, Petrie K, Proudfoot J, Clarke J, Birch M, Christensen H. Smartphones for smarter delivery of mental health programs: A systematic review. J Med Internet Res. 2013;15(11):e247. doi: 10.2196/jmir.2791. http://www.jmir.org/2013/11/e247/ v15i11e247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ghorai K, Akter S, Khatun F, Ray P. mHealth for smoking cessation programs: A systematic review. J Pers Med. 2014;4(3):412–23. doi: 10.3390/jpm4030412. http://www.mdpi.com/resolver?pii=jpm4030412 .jpm4030412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Payne HE, Lister C, West JH, Bernhardt JM. Behavioral functionality of mobile apps in health interventions: A systematic review of the literature. JMIR Mhealth Uhealth. 2015;3(1):e20. doi: 10.2196/mhealth.3335. http://mhealth.jmir.org/2015/1/e20/ v3i1e20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wayne N, Ritvo P. Smartphone-enabled health coach intervention for people with diabetes from a modest socioeconomic strata community: Single-arm longitudinal feasibility study. J Med Internet Res. 2014;16(6):e149. doi: 10.2196/jmir.3180. http://www.jmir.org/2014/6/e149/ v16i6e149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kirwan M, Vandelanotte C, Fenning A, Duncan MJ. Diabetes self-management smartphone application for adults with type 1 diabetes: Randomized controlled trial. J Med Internet Res. 2013;15(11):e235. doi: 10.2196/jmir.2588. http://www.jmir.org/2013/11/e235/ v15i11e235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.BinDhim NF, McGeechan K, Trevena L. Assessing the effect of an interactive decision-aid smartphone smoking cessation application (app) on quit rates: A double-blind automated randomised control trial protocol. BMJ Open. 2014;4(7):e005371. doi: 10.1136/bmjopen-2014-005371. http://bmjopen.bmj.com/cgi/pmidlookup?view=long&pmid=25037644 .bmjopen-2014-005371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Volkova E, Neal B, Rayner M, Swinburn B, Eyles H, Jiang Y, Michie J, Ni MC. Effects of interpretive front-of-pack nutrition labels on food purchases: Protocol for the Starlight randomised controlled trial. BMC Public Health. 2014;14:968. doi: 10.1186/1471-2458-14-968. http://www.biomedcentral.com/1471-2458/14/968 .1471-2458-14-968 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Australian New Zealand Clinical Trial Registry The effects of four front-of-pack labelling schemes compared to standard Nutrition Information Panel, on the healthiness of food Purchases among adult Australian consumers. 2014. [2015-09-08]. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=366945 .
- 14.Hersey JC, Wohlgenant KC, Arsenault JE, Kosa KM, Muth MK. Effects of front-of-package and shelf nutrition labeling systems on consumers. Nutr Rev. 2013 Jan;71(1):1–14. doi: 10.1111/nure.12000. [DOI] [PubMed] [Google Scholar]
- 15.Sutherland LA, Kaley LA, Fischer L. Guiding stars: The effect of a nutrition navigation program on consumer purchases at the supermarket. Am J Clin Nutr. 2010 Apr;91(4):1090S–1094S. doi: 10.3945/ajcn.2010.28450C. http://www.ajcn.org/cgi/pmidlookup?view=long&pmid=20147468 .ajcn.2010.28450C [DOI] [PubMed] [Google Scholar]
- 16.Sacks G, Rayner M, Swinburn B. Impact of front-of-pack 'traffic-light' nutrition labelling on consumer food purchases in the UK. Health Promot Int. 2009 Dec;24(4):344–52. doi: 10.1093/heapro/dap032. http://heapro.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=19815614 .dap032 [DOI] [PubMed] [Google Scholar]
- 17.Dunford E, Trevena H, Goodsell C, Ng KH, Webster J, Millis A, Goldstein S, Hugueniot O, Neal B. FoodSwitch: A mobile phone app to enable consumers to make healthier food choices and crowdsourcing of national food composition data. JMIR mHealth uHealth. 2014;2(3):e37. doi: 10.2196/mhealth.3230. http://mhealth.jmir.org/2014/3/e37/ v2i3e37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.French SA, Wall M, Mitchell NR, Shimotsu ST, Welsh E. Annotated receipts capture household food purchases from a broad range of sources. Int J Behav Nutr Phys Act. 2009;6:37. doi: 10.1186/1479-5868-6-37. http://www.ijbnpa.org/content/6//37 .1479-5868-6-37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cullen K, Baranowski T, Watson K, Nicklas T, Fisher J, O'Donnell S, Baranowski J, Islam N, Missaghian M. Food category purchases vary by household education and race/ethnicity: Results from grocery receipts. J Am Diet Assoc. 2007 Oct;107(10):1747–52. doi: 10.1016/j.jada.2007.07.007.S0002-8223(07)01473-3 [DOI] [PubMed] [Google Scholar]
- 20.Martin SL, Howell T, Duan Y, Walters M. The feasibility and utility of grocery receipt analyses for dietary assessment. Nutr J. 2006;5:10. doi: 10.1186/1475-2891-5-10. http://www.nutritionj.com/content/5//10 .1475-2891-5-10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ni Mhurchu C, Blakely T, Jiang Y, Eyles HC, Rodgers A. Effects of price discounts and tailored nutrition education on supermarket purchases: A randomized controlled trial. Am J Clin Nutr. 2010 Mar;91(3):736–47. doi: 10.3945/ajcn.2009.28742. http://www.ajcn.org/cgi/pmidlookup?view=long&pmid=20042528 .ajcn.2009.28742 [DOI] [PubMed] [Google Scholar]
- 22.Daily Intake Guide: Healthy Eating Made Easy. [2015-09-28]. http://www.mydailyintake.net/
- 23.Guide to creating a front of pack (FoP) nutrition label for pre-packed products sold through retail outlets. 2013. [2015-09-08]. https://www.gov.uk/government/publications/front-of-pack-nutrition-labelling-guidance .
- 24.Health Star Rating – New Food Labelling System. 2014. [2015-09-09]. http://www.foodsafety.govt.nz/industry/general/labelling-composition/health-star-rating/
- 25.Food Standards Australia New Zealand Nutrition Information Panels. 2012. [2015-09-17]. http://www.foodstandards.govt.nz/consumer/labelling/panels/Pages/default.aspx .
- 26.Volkova E, Ni Mhurchu C. The influence of nutrition labeling and point-of-purchase information on food behaviours. Curr Obes Rep. 2015 Jan 9;4(1):19–29. doi: 10.1007/s13679-014-0135-6. [DOI] [PubMed] [Google Scholar]
- 27.van 't Riet J. Sales effects of product health information at points of purchase: A systematic review. Public Health Nutr. 2013 Mar;16(3):418–29. doi: 10.1017/S1368980012001103.S1368980012001103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Statista Share of mobile phone users that use a smartphone in Australia from 2010 to 2017. 2015. [2015-11-10]. http://www.statista.com/statistics/257041/smartphone-user-penetration-in-australia/
- 29.Research New Zealand. 2015. [2015-11-10]. A report on a survey of New Zealanders' use of smartphones and other mobile communication devices http://www.researchnz.com/pdf/Special%20Reports/Research%20New%20Zealand%20Special%20Report%20-%20Use%20of%20Smartphones.pdf .
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Food Label Trial app tutorial 1.
Food Label Trial app tutorial 2.