

Abstract
Piezogenic pedal papules (PPP) are herniations of subcutaneous adipose tissue into the dermis. PPP are skin-colored to yellowish papules and nodules on lateral surfaces of feet that typically become apparent when the patient stands flat on his/her feet. Some connective tissue diseases and syndromes have been reported in association with PPP. Mitral valve prolapse (MVP) is a myxomatous degeneration of the mitral valve, characterized by the displacement of an abnormally thickened mitral valve leaflet into the left atrium during systole. MVP may be isolated or part of a heritable connective tissue disorder. PPP, which is generally considered as an isolated lesion, might be also a predictor of some cardiac diseases associated with connective tissue abnormalities such as MVP. A detailed systemic investigation including cardiac examination should be done in patients with PPP. Since in the literature, there are no case reports of association of PPP with MVP, we report these cases.
Keywords: Connective tissue disorders, mitral valve prolapse, piezogenic pedal papules
What was known?
Piezogenic pedal papules are herniations of subcutaneous adipose tissue into the dermis. Association between PPP and some connective tissue disorders were previously reported. Mitral valve prolapse is a myxomatous degeneration of the mitral valve, which could be isolated or part of a heritable connective tissue disorder.
Introduction
Piezogenic pedal papules (PPP) are herniation of subcutaneous adipose tissue into the dermis. This herniation cause soft, skin-colored or yellowish papules, and nodules on feet. Typically, they become apparent on the medial or lateral aspect of the heels, when the patient stands flat on his/her feet and disappear if the weight is taken off the foot. The papules can be seen unilaterally or bilaterally and may be present on medial, posterior, or lateral aspects of feet. Similar papules can also be seen on the lateral edge of the hand and wrist when pressure is applied. The histology of PPP is fragmentation of dermal elastic tissue and herniation of subcutaneous adipose tissue into the dermis.[1,2]
Generally, no hereditary diseases or syndromes are associated with PPP. However, some connective tissue diseases and syndromes such as Ehlers-Danlos syndrome, Prader-Willi syndrome, and rheumatoid arthritis were reported in association with PPP.[2,3] In addition, in the literature, there are a few reported cases in which PPP is seen together with some cardiac diseases including rheumatic heart disease, mitral insufficiency, and pulmonary hypertension.[1] PPP are usually painless and benign. Rarely, they can be painful. Painful PPP are more likely to be seen in association with Ehlers-Danlos syndrome, obesity, and occupational or sporting exposure than painless ones. Painful papules can limit patients’ recreational or occupational activities, and treatment may be needed.
Herein, we present two cases with PPP and mitral valve prolapse (MVP).
Case Reports
Case 1
A 35-year-old male patient was admitted to our Dermatology Clinic with a complaint of asymptomatic skin-colored lesions on his left foot. According to his medical history, he has not been diagnosed with any systemic disease and had not used any medication. There was no history of such lesions in his family members. The lesions developed in the past 1–2 years. Typically, they were only present when the patient was standing and disappeared when the weight was taken off the foot [Figure 1]. He had no pain while standing. Dermatological examination revealed soft skin-colored papules on his left foot. On ultrasonography, millimetric dermal defects on his left heel and herniation of subcutaneous adipose tissue into the epidermis were detected. Patient's lesions were diagnosed as PPP clinically. Histopathological examination was not considered because the diagnosis was clear. In addition, due to the complaint of atypical chest pain, the patient was referred to our Out-patient Cardiology Clinic. On auscultation, a late systolic murmur with a mid-systolic click was audible at the apex. The rest of the physical examination was normal. His electrocardiography revealed a normal sinus rhythm with an incomplete right bundle branch block. On echocardiography, MVP with mild mitral regurgitation was detected [Figure 2]. His biochemical tests were also within normal limits. Since the papules were asymptomatic, surgical excision was not considered. No medication was given for his asymptomatic papules or MVP. He will be followed for his PPP and MVP.
Figure 1.

Soft skin-colored papules on the medial aspect of the left heel (arrow), typically disappear when the weight is taken off the foot (a) and appear when the patient stands with full on the heels (b)
Figure 2.
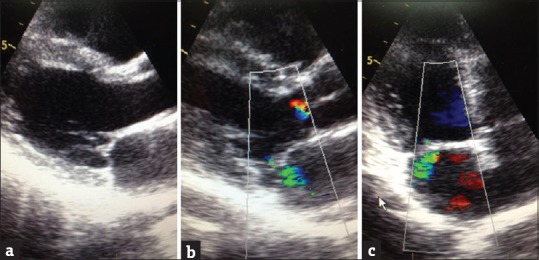
Parasternal long-axis view showing mitral valve prolapse (a), parasternal long-axis color-Doppler imaging showing mitral valve prolapse with mild mitral regurgitation (b), apical four-chamber color-Doppler imaging showing mild mitral regurgitation (c)
Case 2
A 32-year-old female patient was admitted to our Cardiology Clinic with a complaint of palpitation. She was diagnosed with MVP 2 years ago and does not get any medication for it. On physical examination; in addition to typical auscultation findings of MVP, asymptomatic skin-colored lesions were detected bilaterally on her wrists. Her electrocardiography revealed sinus tachycardia. Her biochemical tests including thyroid panel were within normal limits. Transthoracic echocardiography revealed MVP with minimal mitral regurgitation. Patient was referred to the Dermatology Clinic for the lesions on her wrists. She had them for several years, and she did not have any family member, who has such lesions. Dermatological examination revealed soft skin-colored papules that typically appeared when pressure is applied [Figure 3], bilaterally on her wrists, and they were diagnosed as PPP. Low-dose metoprolol treatment was initiated for palpitation, and no treatment was considered for these asymptomatic papules.
Figure 3.

Soft skin-colored papules on the wrist (arrow); typically disappear when pressure is taken off (a) and appear when pressure is applied (b)
Discussion
PPP are common lesions; however, there is no agreement about the prevalence of PPP which generally varies between 10% and 20% in the literature.[1,2,3] Nevertheless in a recent study with 100 patients, PPP were seen in 80 of them,[4] and this indicates that the prevalence of PPP might be higher than thought. PPP were first described by Shelley et al. in patients with long-term heavy loads. Reaction to internal mechanical stress is considered as the main reason for the formation of these lesions. Generally, they occur on feet but can be found on hands or wrists. Typically papules appear when weight is put on that particular area. Papules can be painful if there is herniation of adipose tissue into the dermis as a result of reduction in dermal thickness. This pain can be explained by ischemia due to extrusion of adipose tissue with its vascular supply and associated nerves.[1,2]
PPP are frequently reported in especially physically active patients such as marathon runners and spending too much time for standing or carrying heavy loads in their daily jobs. To regard PPP as an inherited disease is controversial but the association with connective tissue disorders such as Ehlers-Danlos syndrome was described in previous case reports.[2]
It was reported that even some unexpected dermatological lesions such as skin tags could be related to cardiac diseases.[5] PPP, which is generally considered an isolated lesion might be also a predictor of some cardiac diseases associated with connective tissue abnormalities.
MVP is a myxomatous degeneration of the mitral valve, characterized by the displacement of an abnormally thickened mitral valve leaflet into the left atrium during systole. This is generally a benign condition but in some severe cases, MVP can be associated with complications such as mitral regurgitation, infectious endocarditis, congestive heart failure, and rarely sudden cardiac death.[6] MVP can be easily diagnosed by standard two-dimensional echocardiography in suspected patients. The systolic movement of portions or segments of the mitral valve leaflets into the left atrium can be observed during left ventricular systole on echocardiography. MVP can be sporadic or familial. Although no specific gene has been described, different loci on chromosomes have been found to be linked to MVP.[7] Further, MVP may be isolated or part of a heritable connective tissue disorders including Marfan syndrome, Ehlers-Danlos syndrome, or osteogenesis imperfect.[8,9,10] Isolated MVP is also considered as a cardiovascular abnormality of connective tissue origin. Due to its frequency in the general population, MVP constitutes the larger group of patients with heritable connective tissue abnormalities of the heart.[8] The prevalence of MVP is generally estimated as 2–3%.[6,11] Similar to PPP, some studies suggest that MVP prevalence might be higher than estimated (5–15% up to 38%).[12,13,14] In addition, both PPP and MVP are reported to be more frequent in different ethnic groups such as in Nigerians MVP prevalence is 10% and in Indians PPP prevalence is 80%.[4,14] We suggest that the higher prevalence of both MVP and PPP in some ethnic groups may support the association between PPP and MVP. Further studies are needed to support this hypothesis.
Association between PPP and heritable connective tissue abnormalities such as Ehlers-Danlos syndrome was also described in previous reports.[2] PPP might be a predictor of connective tissue abnormalities. A detailed systemic investigation, including cardiac examination, should be considered in patients with PPP. MVP is also more frequent in patients with connective tissue abnormalities.[8,9,10] Therefore, PPP may also be associated with MVP. In literature, there is only one case report of an association between PPP and mitral regurgitation due to rheumatic heart disease.[1] Since in the literature, there are no case reports of an association between PPP and MVP, we report these cases. Due to common occurrence of both PPP and MVP, this association may be also a coincidence. We suggest cardiac workup in patients with PPP in order to find out the relation with cardiac abnormalities.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
What is new?
Piezogenic pedal papules (PPP) which is generally considered as an isolated lesion, might be predictor of some cardiac diseases, such as mitral valve prolapse, associated with connective tissue abnormalities. A detailed systemic investigation including cardiac examination should be considered in patients with PPP.
References
- 1.Singh SK, Tehseen M, Kalam A. Painless piezogenic pedal papules in a patient with rheumatic heart disease. Indian J Dermatol Venereol Leprol. 2002;68:107–8. [PubMed] [Google Scholar]
- 2.Kahana M, Feinstein A, Tabachnic E, Schewach-Millet M, Engelberg S. Painful piezogenic pedal papules in patients with Ehlers-Danlos syndrome. J Am Acad Dermatol. 1987;17(2 Pt 1):205–9. doi: 10.1016/s0190-9622(87)70192-3. [DOI] [PubMed] [Google Scholar]
- 3.Schepis C, Greco D, Siragusa M, Romano C. Piezogenic pedal papules during Prader-Willi syndrome. J Eur Acad Dermatol Venereol. 2005;19:136–7. doi: 10.1111/j.1468-3083.2004.01048.x. [DOI] [PubMed] [Google Scholar]
- 4.Zaidi Z, Jafri N, Noori B, Thawerani H. Piezogenic papules – A study of 100 cases. J Pak Med Assoc. 1995;45:93–4. [PubMed] [Google Scholar]
- 5.El Safoury OS, Ezzat M, Abdelhamid MF, Shoukry N, Badawy E. The evaluation of the impact of age, skin tags, metabolic syndrome, body mass index, and smoking on homocysteine, endothelin-1, high-sensitive C-reactive protein, and on the heart. Indian J Dermatol. 2013;58:326. doi: 10.4103/0019-5154.113947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Boudoulas KD, Boudoulas H. Floppy mitral valve (FMV)/mitral valve prolapse (MVP) and the FMV/MVP syndrome: Pathophysiologic mechanisms and pathogenesis of symptoms. Cardiology. 2013;126:69–80. doi: 10.1159/000351094. [DOI] [PubMed] [Google Scholar]
- 7.Grau JB, Pirelli L, Yu PJ, Galloway AC, Ostrer H. The genetics of mitral valve prolapse. Clin Genet. 2007;72:288–95. doi: 10.1111/j.1399-0004.2007.00865.x. [DOI] [PubMed] [Google Scholar]
- 8.Bowen J, Boudoulas H, Wooley CF. Cardiovascular disease of connective tissue origin. Am J Med. 1987;82:481–8. doi: 10.1016/0002-9343(87)90448-7. [DOI] [PubMed] [Google Scholar]
- 9.Leier CV, Call TD, Fulkerson PK, Wooley CF. The spectrum of cardiac defects in the Ehlers-Danlos syndrome, types I and III. Ann Intern Med. 1980;92(2 Pt 1):171–8. doi: 10.7326/0003-4819-92-2-171. [DOI] [PubMed] [Google Scholar]
- 10.Hirata K, Triposkiadis F, Sparks E, Bowen J, Boudoulas H, Wooley CF. The Marfan syndrome: Cardiovascular physical findings and diagnostic correlates. Am Heart J. 1992;123:743–52. doi: 10.1016/0002-8703(92)90515-w. [DOI] [PubMed] [Google Scholar]
- 11.Freed LA, Levy D, Levine RA, Larson MG, Evans JC, Fuller DL, et al. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med. 1999;341:1–7. doi: 10.1056/NEJM199907013410101. [DOI] [PubMed] [Google Scholar]
- 12.Levy D, Savage D. Prevalence and clinical features of mitral valve prolapse. Am Heart J. 1987;113:1281–90. doi: 10.1016/0002-8703(87)90956-2. [DOI] [PubMed] [Google Scholar]
- 13.Warth DC, King ME, Cohen JM, Tesoriero VL, Marcus E, Weyman AE. Prevalence of mitral valve prolapse in normal children. J Am Coll Cardiol. 1985;5:1173–7. doi: 10.1016/s0735-1097(85)80021-8. [DOI] [PubMed] [Google Scholar]
- 14.Oladapo OO, Falase AO. Prevalence of mitral valve prolapse in healthy adult Nigerians as diagnosed by echocardiography. Afr J Med Med Sci. 2001;30:13–6. [PubMed] [Google Scholar]