

Introduction
Herlyn-Werner-Wunderlich (HWW) syndrome is an example of mullerian duct anomaly and is due to lateral fusion defect comprising uterus didelphys, obstructed hemivagina, and ipsilateral renal agenesis. Reported incidence of this particular syndrome is 0.16–10 %. This is usually observed in postmenarchal adolescents and young women presenting with irregular menses, dysmenorrhoea, abdominal pain, and pelvic mass [1]. The diagnosis may be difficult due to infrequency of this syndrome. Complex malformation is rare, often incorrectly identified, inappropriately treated, and incorrectly reported [2].
Case Report
Sixteen-year-old girl, student of 9th standard, reported to Gynae OPD with H/O pain lower abdomen for 1–2 years which had increased gradually and was moderate to severe for the last 2–3 months. It was insidious in onset, moderate in intensity, continuous, dull ache with no relieving factor, non-radiating but associated with vomiting whenever pain was severe. There was H/O aggravation of pain in the premenstrual phase (congestive dysmenorrhoea). There was no associated menstrual irregularity, urinary, or bowel complaint. There was no history suggestive of T.B. or that of loss of appetite/weight. There was nothing significant in family and past history. There was no abnormality on GPE, and secondary sexual characters were well developed. USG suggested bicornuate uterus with right horn well developed and left horn smaller in size. There was evidence of hematometra and hematosalpinx with free fluid in peritoneal cavity and the absence of right kidney. MRI of pelvis was done which confirmed the findings of USG, i.e., uterus didelphys with two cervix with right-sided hematometra and hematosalpinx with free fluid in peritoneal cavity and the absence of right kidney. On history and the findings of the imaging, the case was diagnosed as HWW syndrome. EUA was done which revealed single vagina of normal caliber with single cervix toward the left side. There was a bulge on right fornix and right adnexal mass of size 8 × 5 cm. Clinical diagnosis was uterus bicornuate unicollis with non-communicating right rudimentary horn. She was taken up for exploratory laparotomy.
Operative Findings
Uterus was didelphys with right horn non-communicating and enlarged to about 10 × 8 cm. Right fallopian tube showed hematosalpinx along with chocolate cyst of right ovary and free dark altered blood in peritoneal cavity. Left-sided horn of uterus, fallopian tube, and ovary were normal in size and shape (as seen in Fig. 1). Removal of rudimentary horn with right salpingectomy and cystectomy was done. Ovarian reconstruction of remaining part of ovary was done. Postoperative period was uneventful and she was discharged on 5th POD in good health and called for follow-up after 4 weeks. The HPE report confirmed the findings of rudimentary horn with hematosalpinx. On follow-up, there was no complaint and she had normal periods.
Fig. 1.

Long arrow shows right rudimentary horn & encircled structure is right hematosalpinx. Smaller arrow is pointing toward left-sided normal uterus, fallopian tube, & left ovary
Discussion
Herlyn-Werner-Wunderlich (HWW) syndrome is a rare congenital anomaly characterized by triad of uterus didelphys, hemivagina, and absent ipsilateral kidney. Uterus didelphys is a symmetric anomaly in which two completely separate uterine cavities are identified, each with normal zonal anatomy as well as its own endometrial cavity and cervix. No communication between the two cavities is present. A complete or partial longitudinal vaginal septum is associated with this anomaly in 75 % of case [3]. Majority of cases present with hematocolpos and/or hematometra along with renal agenesis. According to the American Fertility Society classification of mullerian anomalies, uterus didelphys is class III anomaly, as shown in Fig. 2.
Fig. 2.
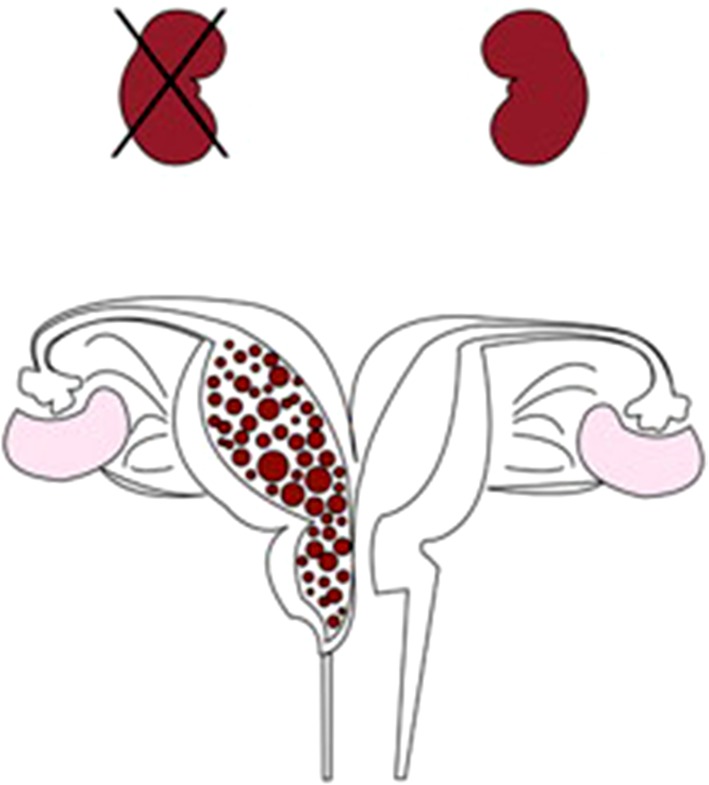
Diagrammatic representation of the Mullerian anomaly
The etiology is not known. The simultaneous insult to the paramesonephric system and metanephros could suggest a multifactorial origin [4]. An early failure of the metanephric diverticulum to develop from mesonephric duct results in agenesis of the ureteric bud, leading to ipsilateral agenesis of the ureter and kidney. The mesonephros is responsible for the development and positioning of paired paramesonephric ducts which result in un-united two horns of uterus.
HWW syndrome is usually discovered at puberty with non-specific symptoms like increasing pelvic pain, dysmenorrhoea, and palpable mass due to associated hematocolpos or hematometra which results from retained long-standing menstrual flow in the obstructed vagina. It rarely occurs with primary infertility in early adulthood when the vaginal septum is incomplete [5]. Pelvic pain is the most common presenting symptom (90 %) followed by an abdominal mass (40 %) and pressure symptoms. It rarely occurs with primary infertility. Early detection and immediate surgical resection of the obstructing vaginal septum can provide pain relief and prevent further complications, most common being endometriosis [1].
Conclusion
Prompt and accurate diagnosis of female reproductive tract disorders, including HWW syndrome, is necessary to prevent complications and preserve future fertility. Early recognition of this relatively rare syndrome would lead to the immediate, proper surgical intervention. The consequences that potentially occur due to the failure of treatment include urinary retention, hematosalpinx, endometriosis, and rupture of a tubo-ovarian abscess.
Acknowledgments
Conflict of interest
The authors declare that they have no conflict of interest.
Dr. Rita Mittal
is a Operating surgeon Obstetrician and Gynecologist at Kamla Nehru State Hospital for Mother and Child, Shimla and is serving as an Associate Professor. She did her postgraduate degree in 1997 and senior residency in 2004 in the same institution. She is a member of FOGSI since 1995. She has many publications in national as well as international journals.
Footnotes
Rita Mittal is a Operating surgeon Obstetrician and Gynecologist at Kamla Nehru State Hospital for Mother and Child, Shimla and is serving as an Associate Professor.
References
- 1.Kabiri D, Arzy Y, Hants Y. Herlyn-Werner-Wunderlich syndrome: uterus didelphys and obstructed hemivagina with unilateral renal agenesis. Imaging. 2013;15:66. [PubMed] [Google Scholar]
- 2.Arikan II, Harna M, Harma MI. Herlyn-Werner-Wunderlich syndrome—a case report. J Turk-Ger Gynecol Assoc. 2010;11:107–109. doi: 10.5152/jtgga.2010.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mahale A, Mahale N, Santosh K. Herlyn-Werner-Wunderlich syndrome-common presentation of an unusual variation: a case report. IOSR-J Dent Med Sci. 2014;13(6):01–03. doi: 10.9790/0853-13650103. [DOI] [Google Scholar]
- 4.El-agwany AS. Herlyn-Werner-Wunderlich syndrome. Afr J Urol. 2010;20(91-9):4. [Google Scholar]
- 5.Vescovo RD, et al. Herlyn-Werner-Wunderlich syndrome: MRI findings, radiological guide and differential diagnosis. BMC Med Imaging. 2012;12:4. doi: 10.1186/1471-2342-12-4. [DOI] [PMC free article] [PubMed] [Google Scholar]