

Abstract
Objective:
Maintenance of meticulous oral health practices is critical for patients who are under orthodontic treatment as failure to do so can result in deterioration of periodontal health. Thus, the present study was commenced to assess dental negligence and oral health status among patients undergoing orthodontic treatment using dental neglect scale (DNS) questionnaire.
Materials and Methods:
The present cross-sectional study was planned and carried out among the 40 patients undergoing fixed orthodontic treatment. The study comprised of two questionnaires, one was close-ended questionnaire which consisted of questions regarding patient practice in maintenance of oral health and other questionnaire comprised of DNS followed by examination of oral hygiene status using Oral Hygiene Index Simplified. Data so obtained were subjected to analysis using SPSS version 20 and Chi-square test was used to statistically analyze data with P < 0.05 regarded as a statistically significant value.
Results:
The present study revealed that 63% among the studied orthodontic patients brushed once daily, 26% brushed twice daily, and 11% brushed thrice. About one-fourth was using brush with soft bristles and only 9% among the respondents used interdental aids. Data revealed positive correlation between DNS and oral hygiene index-simplified score with P < 0.05.
Conclusion:
The present study found that less frequency of brushing, rinsing mouth, and eating sticky and hard food can be attributed to self-neglect of the orthodontic patients.
Keywords: Brushing, dental neglect, fixed orthodontic treatment, interdental aids, self-negligence
INTRODUCTION
Orthodontic treatment ensures proper alignment of the teeth and improves the occlusal and jaw relationship, which aids in better mastication, speech, and facial esthetics, which contributes to general and oral health, thereby improving the quality of life. Orthodontic treatment, in addition to its benefits, has also associated risks and complications. Periodontal complications are found to be most common side effect of orthodontic therapy.[1] Inability of the orthodontic patient to clean oral cavity adequately due to the presence of braces can be considered as a factor leading to inflamed gingiva. Gingivitis as well as gingival enlargement seems to be the most common short-term effect of orthodontic treatments on the periodontal health.[2]
Maintenance of meticulous oral health practices are critical for patients who are under orthodontic treatment as failure to maintain good oral hygiene can result in accumulation of plaque over the braces and other orthodontic appliances, leading to inflammation of gingiva and further causing deterioration of periodontium health. Thus, the orthodontist carries a dual responsibility of advising patients regarding measures for plaque control as well as to observe the efficiency of the oral hygiene practices so that periodontal health can be maintained. However, in spite of recommending appropriate instructions by orthodontist, most of the patients undergoing orthodontic treatment usually fall short to maintain a satisfactory standard of plaque control.[3] Atassi and Awartani[4] investigated status of oral hygiene among patients undergoing fixed orthodontic therapy in Saudi Arabia and reported inadequate oral home care among patients under fixed orthodontic therapy. Terri[5] reported less than optimal oral hygiene as a contributing factor to poor tissue status among orthodontic patients. Hence, it is utmost important that the orthodontist should be able to commune the significance of oral care practices to encourage patients to maintain an adequate standard of oral hygiene throughout orthodontic therapy.[3] Thus, the present study was commenced to assess dental negligence and oral health status among patients undergoing orthodontic treatment using dental neglect scale (DNS) questionnaire.
MATERIALS AND METHODS
The present cross-sectional study was planned and conducted among the 40 patients (27 females and 13 males) aged 18–30 years undergoing fixed orthodontic treatment who fulfilled the inclusion criteria of the study and who were willing to participate in the study. The clearance of the ethical committee of the institute was obtained. Simple random sampling technique was employed to enroll participants for the study. The inclusion criterion consisted of patients undergoing orthodontic treatment for more than 3 months. This duration of time period was selected as in the initiation of any treatment patients are usually conscious regarding the same but, as the time passes, they become careless toward same. The exclusion criterion was any dental student undergoing fixed orthodontic treatment to avoid the bias in the study. Informed consent was obtained from each patient before the commencement of the study. The study comprised of two questionnaires, one was close-ended questionnaire[5] which consisted of questions regarding patient practice in maintenance of oral health [Table 1] and other questionnaire comprised of DNS [Table 2][6] followed by examination of oral hygiene status using Oral Hygiene Index Simplified (OHIS). The reliability (Cronbach's alpha) of the questionnaire was tested in a pilot study conducted before the commencement of final study, and it was found to be 0.71 for questionnaire 1 and 0.69 for questionnaire 2. At the time when respondents were filling questionnaires, it was taken into consideration that the concerned participant fully understood the questions and did not discuss the data with any other participant. Each participant rated six statements which ranged from Definitely Yes to Definitely No. The values obtained for the DNS varied from 6 to 30, with more scores representing more neglect toward dental health. Data so obtained were analyzed using SPSS version 20 (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) and Chi-square test was used to statistically analyze data with P < 0.05 considered statistically significant value.
Table 1.
Distribution of participants’ response regarding oral hygiene practices
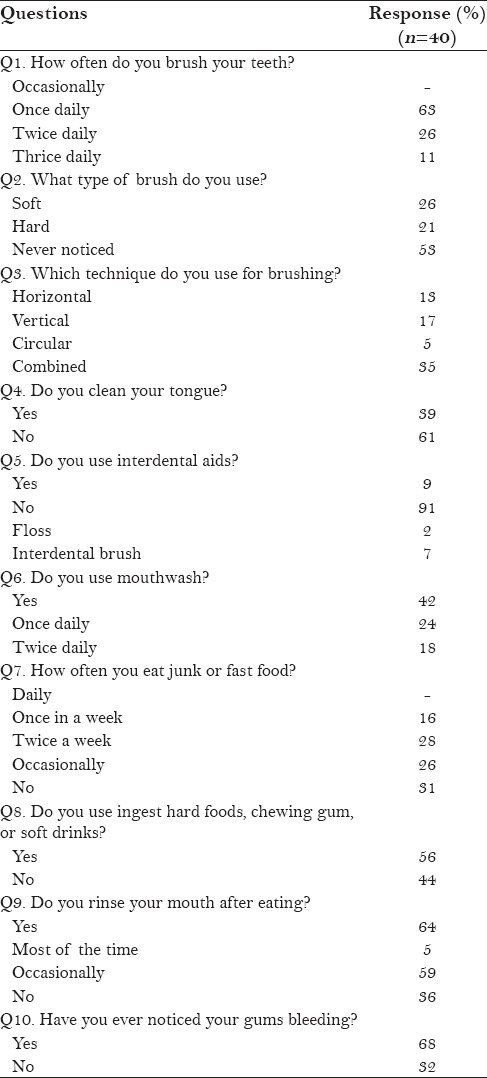
Table 2.
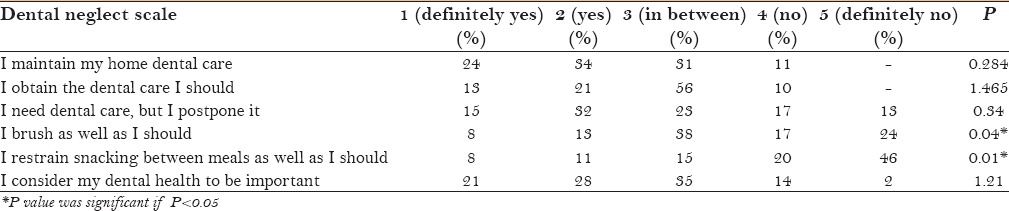
Dental neglect score scale distribution (n=40)
RESULTS
In the present study, among the respondents, 27 were females and 13 were males. Data regarding the response of participants [Table 1] revealed that 63% among them brushed once daily, 26% brushed twice daily, and 11% brushed thrice. About more than half of the participants, 53% never noticed the type of brush they were using, 26% were using brush with soft bristles, and 21% hard were using brush with soft bristles. Regarding technique of brushing, 13% used horizontal, 17% used vertical, 5% used circular, and 35% used combined technique. 39% of the respondents reported that they clean their tongue and only 9% among the respondents used interdental aids; among them, 2% used floss and 7% used interdental brush. 42% of the respondents used mouthwash for rinsing the mouth, of which 24% used once daily and 18% used twice daily. Regarding eating habits, 16% of the respondents eat junk or fast food once in a week, 28% twice a week, 26% occasionally, 31% avoided fast food, and 56% among respondents ingested hard foods, chewing gums or soft drinks. 5% of respondents used to rinse their mouth most of the time after eating, 59% occasionally, and 36% do not rinse their mouth after eating. 68% of them noticed bleeding gums.
The data in Table 2 reveal that 24% of the respondents revealed that they definitely maintain their home dental care, 13% that they obtain the dental care they need, 15% that they require dental care, but they postpone it, 8% brushed as well as they should, only 8% responded that they definitely restrain snacking in between meals as well as they should, and 21% of the respondents considered their dental health to be important. DNS score was divided into two parts to compare DNS with OHIS, that is, low (DNS score ≤15) and high (DNS score >15) DN groups.
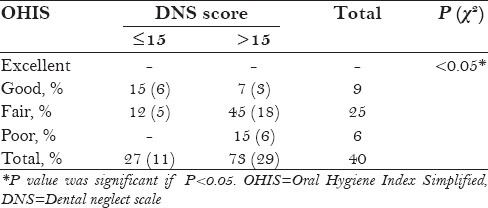
According to interpretation of OHIS scores [Table 3], among lower dental neglect group 15% had good oral hygiene and 12% had fair oral hygiene whereas in group with higher lower DNS, 7% had good oral hygiene, 45% had fair oral hygiene, and 15% had poor oral hygiene. Data revealed positive correlation between DNS and oral hygiene index-simplified score with P < 0.05.
Table 3.
Comparison of dental neglect scale and oral hygiene index-simplified score
DISCUSSION
Dental esthetics are the main reason that attracts patient to undergo orthodontic treatment. Even though orthodontic treatment improves oral health, esthetics, and self-esteem, appliances used during orthodontic therapy can result in unwanted hitches if required care is not considered during the treatment phase. It is essential that the person enduring orthodontic treatment are informed of these possible risks, so that they must be aware of their responsibilities during the treatment.[7,8] The present study found that 73% individuals enrolled for the study had high DNS that attributed to fair oral hygiene index among 45% and poor oral hygiene index among 15% of respondents. Maintenance of a healthy oral status demands a symbiotic relationship of the patient and dentist, which is the utmost important factor that determines the dental health and attitude of a person toward their dentition.[9]
DNS provides an estimation regarding concern of a person toward oral health. This scale can be considered as a useful alternative for collection of clinical data in oral health surveys when insufficient resources restrict the oral examination of study population.[10] Acharya et al.[11] conducted a study to the endorse the Indian translation of the DNS among a sample of Indian women and found to be reliable for evaluating oral health neglect among the study participants.
Subjects experiencing orthodontic treatment go through significant changes in the oral cavity due to accumulation of food particles within the teeth and braces that lead to increase in plaque formation as fixed appliances hinder adequate cleaning for the patient. Gingivitis and enamel decalcification around fixed appliances are frequent complications in the absence of implementation preventive programs.[12] The main cause behind these periodontal complications patient factors that include past periodontal condition, increased susceptibility, and poor oral hygiene.[13]
The present study revealed that 63% of the studied orthodontic patients brushed once daily, 26% brushed twice daily, and 11% brushed thrice. About one-fourth was using brush with soft bristles and only 9% among the respondents used interdental aids. 42% of the respondents used mouthwash for rinsing the mouth, out of which 24% used once daily and 18% used twice daily.
Bardal et al.[14] investigated the oral hygiene practices among patients undergoing fixed orthodontic treatment and found that around 44% of the subjects reported tooth brushing thrice a day, 22% even more than thrice a day, 30% subjects brushed twice daily, 4% only once a day, and only 11% of the studied subjects reported using interdental and end-tufted brushes. Sukhia et al.[15] reported that lack of oral hygiene practices among the orthodontic patients presents a strong affinity for enamel decalcification.
Dentist recommends patient undergoing fixed orthodontic treatment to brush and floss after meals using a toothbrush with soft bristles and for flossing the teeth, it is important to get the floss under the wire that attaches the brackets together.[16] The oldest method of plaque removal is manual tooth brushing and instructions should accentuate the need to apply required pressure to remove plaque. Chlorhexidine mouthwashes used in addition to tooth brushing control gingival inflammation and fluoride mouthwash significantly reduces the extent of enamel decalcification during orthodontic treatment.[3]
Plaque plays a major etiologic role in the development of gingivitis. Studies conducted on experimental animal have found that in the absence of plaque, forces caused by orthodontic wires and tooth movements do not cause gingivitis. However, in the presence of plaque, these similar forces can induce angular bone defects whereas tipping and intruding orthodontic tooth movements can result in attachment loss. Thus, the forgoing data conclude that utmost important factor is the presence of microbial plaque that results in periodontal diseases.[6] Thus, the characteristic relationship between orthodontic and periodontic specialties in treating patients can be referred to as synergistic relation as the word synergy refers to different influences or factors that act together to produce result more than that expected by separate effects of the individual factors.[9]
The present study found that around half of the respondents ingested hard foods, chewing gums, or soft drinks. The present can be attributed to self-neglect of patients. It is necessary to understand various factors resulting in self-neglect to frame a sound practice approach, which usually involves insufficient personal and environmental hygiene practices along with nonadherence to recommended health care regimen.[17] Dentists instruct patients undergoing orthodontic treatment not to eat hard and sticky foods that can result in breakage of the orthodontic appliances.[16]
Patients undergoing orthodontic treatment must be encouraged to maintain meticulous oral hygiene as the difficult areas to be cleaned in banded teeth are located on the cervical side of the band and in case of teeth with bonded brackets the crucial surfaces which receive inadequate cleaning are areas on the mesial and distal sides of the bracket base. Hence, as these areas are placed under the arch wire and are inaccessible to toothbrush bristles, they are prone to detrimental effects.[14]
In view of this, it is mandatory to undergo scaling along with complete examination of oral cavity performed routinely during this phase. Thus, at the end of active orthodontic treatment and on the removal of appliances, the patient should be recommended renewed oral hygiene instructions for diminishing the risk of recession. Hence, it is the responsibility of orthodontist to educate patient in respect of their brushing technique in conjunction to considering adjunct interdental cleaning aids, such as an oral irrigator, dental floss, and interdental toothbrushes.[1] Hence, knowledge and positive attitude toward oral health are an important consideration for good oral health status.[9]
The limitation of the present study is that patients selected belonged to one geological area as well as most of them belonged to middle class socioeconomic group as patients from high class usually prefer private clinics and poor people do not afford spending on aesthetics, thus further studies with subjects enrolled from various socioeconomic groups with large sample size should be carried out to draw conclusions.
CONCLUSION
The present study found that less frequency of brushing, rinsing mouth, and eating sticky and hard food can be attributed to self-neglect of the orthodontic patients. Dentist must emphasize patients regarding significance of plaque control and maintenance of good oral hygiene before and during commencement of the fixed appliance treatment and importance of ensurance of patient compliance throughout treatment to prevent deterioration of periodontal health.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest
REFERENCES
- 1.Singh G, Batra P. The orthodontic periodontal interface: A narrative review. J Int Clin Dent Res Organ. 2014;6:77–85. [Google Scholar]
- 2.Dannan A. An update on periodontic-orthodontic interrelationships. J Indian Soc Periodontol. 2010;14:66–71. doi: 10.4103/0972-124X.65445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sebbar M, Abidine Z, Laslami N, Bentahar Z. Periodontal health and orthodontics. In: Virdi MS, editor. Emerging Trends in Oral Health Sciences and Dentistry. 1st ed. China: InTech; 2015. pp. 717–32. [Google Scholar]
- 4.Atassi F, Awartani F. Oral hygiene status among orthodontic patients. J Contemp Dent Pract. 2010;11:E025–32. [PubMed] [Google Scholar]
- 5.Terri T. Oral health maintenance in orthodontics. Dimens Dent Hyg. 2014;12:19–22. [Google Scholar]
- 6.Jain N, Mitra D, Ashok KP, Dundappa J, Soni S, Ahmed S. Oral hygiene-awareness and practice among patients attending OPD at Vyas Dental College and Hospital, Jodhpur. J Indian Soc Periodontol. 2012;16:524–8. doi: 10.4103/0972-124X.106894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sarkar P, Dasar P, Nagarajappa S, Mishra P, Kumar S, Balsaraf S, et al. Impact of dental neglect scale on oral health status among different professionals in Indore City-A cross- sectional study. J Clin Diagn Res. 2015;9:ZC67–70. doi: 10.7860/JCDR/2015/14321.6674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Meeran NA. Iatrogenic possibilities of orthodontic treatment and modalities of prevention. J Orthod Sci. 2013;2:73–86. doi: 10.4103/2278-0203.119678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Vinod K, Reddy YG, Reddy VP, Nandan H, Sharma M. Orthodontic-periodontics interdisciplinary approach. J Indian Soc Periodontol. 2012;16:11–5. doi: 10.4103/0972-124X.94597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kumar A, Manjunath PP, Sowmya KR. Dental neglect – A review. J Dent Sci. 2015;3:1–9. [Google Scholar]
- 11.Acharya S, Pentapati KC, Bhat PV. Dental neglect and adverse birth outcomes: A validation and observational study. Int J Dent Hyg. 2013;11:91–8. doi: 10.1111/idh.12001. [DOI] [PubMed] [Google Scholar]
- 12.Baheti MJ, Toshniwal NG, Bagrecha SD. Oral health in orthodontic treatment: Preventive and innovative approach. J Dentofacial Sci. 2014;3:39–46. [Google Scholar]
- 13.Alfuriji S, Alhazmi N, Alhamlan N, Al-Ehaideb A, Alruwaithi M, Alkatheeri N, et al. The effect of orthodontic therapy on periodontal health: A review of the literature. Int J Dent. 2014;2014:585048. doi: 10.1155/2014/585048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bardal PA, Olympio KP, Bastos JR, Henriques JF, Buzalaf MA. Education and motivation in oral health – Preventing disease and promoting health in patients undergoing orthodontic treatment. Dent Press J Orthod. 2011;16:95–102. [Google Scholar]
- 15.Sukhia HR, Ayub A, Ghandhi D. Enamel decalcification in orthodontic patients; prevalence and oral distribution – A cross sectional study. Pak Oral Dent J. 2008;28:193–7. [Google Scholar]
- 16.Rosenblatt M. Smile Works Orthodontics- Oral hygiene. [Last assessed on 12 Jan 2016]. Available from: http://www.smileworksortho.ca/oral-hygiene.php .
- 17.Ajagannanavar SL, Sequeira PS, Jain J, Battur H. Dental neglect among college going adolescents in Virajpet, India. J Indian Assoc Public Health Dent. 2014;12:215–8. [Google Scholar]