

Abstract
Medication-related osteonecrosis of the jaw (MRONJ) is a severe adverse drug reaction, consisting of progressive bone destruction in the maxillofacial region of patients. ONJ can be caused by two pharmacological agents: Antiresorptive (including bisphosphonates (BPs) and receptor activator of nuclear factor kappa-B ligand inhibitors) and antiangiogenic. MRONJ pathophysiology is not completely elucidated. There are several suggested hypothesis that could explain its unique localization to the jaws: Inflammation or infection, microtrauma, altered bone remodeling or over suppression of bone resorption, angiogenesis inhibition, soft tissue BPs toxicity, peculiar biofilm of the oral cavity, terminal vascularization of the mandible, suppression of immunity, or Vitamin D deficiency. Dental screening and adequate treatment are fundamental to reduce the risk of osteonecrosis in patients under antiresorptive or antiangiogenic therapy, or before initiating the administration. The treatment of MRONJ is generally difficult and the optimal therapy strategy is still to be established. For this reason, prevention is even more important. It is suggested that a multidisciplinary team approach including a dentist, an oncologist, and a maxillofacial surgeon to evaluate and decide the best therapy for the patient. The choice between a conservative treatment and surgery is not easy, and it should be made on a case by case basis. However, the initial approach should be as conservative as possible. The most important goals of treatment for patients with established MRONJ are primarily the control of infection, bone necrosis progression, and pain. The aim of this paper is to represent the current knowledge about MRONJ, its preventive measures and management strategies.
Keywords: Bisphosphonate-associated osteonecrosis of the jaw, bone metastases, drug therapy, medication-related osteonecrosis of the jaw, osteoporosis
INTRODUCTION
Medication-related osteonecrosis of the jaw (MRONJ) is a severe adverse drug reaction, consisting of progressive bone destruction in the maxillofacial region of patients.
In 2014, the American Association of Oral and Maxillofacial Surgeons (AAOMSs) suggested to change the nomenclature from bisphosphonate- related osteonecrosis of the jaw (BRONJ) to MRONJ to accommodate the growing number of osteonecrosis cases involving the maxilla and mandible associated with other antiresorptive (denosumab) and antiangiogenic therapies.[1,2] The aim of this paper is to represent the current knowledge about MRONJ, its preventive measures and management strategies.
MEDICATION-RELATED OSTEONECROSIS OF THE JAW RELATED MEDICATION
Osteonecrosis of the jaw (ONJ) can be caused by two pharmacological agents: Antiresorptive (including bisphosphonates (BPs) and receptor activator of nuclear factor kappa-B ligand [RANK-L] inhibitors) and antiangiogenic.
BPs can be divided into aminobisphosphonates (NBPs) and non-NBPs on the basis of an amino functional group presence in the molecule. NBPs are the one involved in the ONJ [Table 1].
Table 1.
Medication-related osteonecrosis of the jaw-related medications
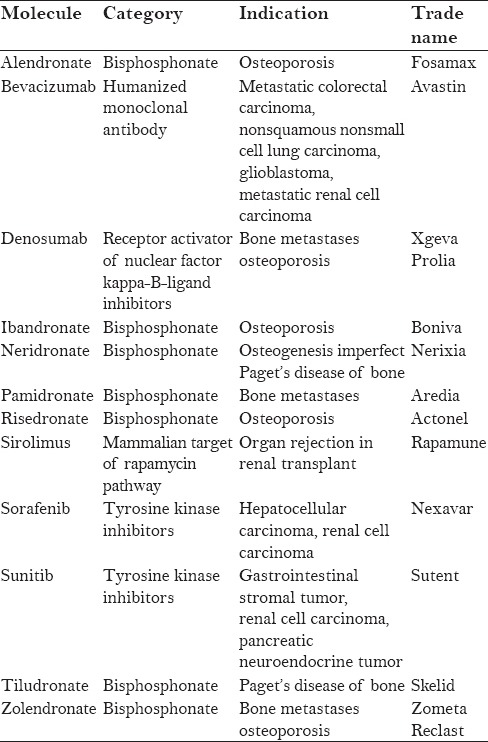
Intravenous (IV) BPs are utilized to treat conditions associated with cancer as well as hypercalcemia of malignancy, skeletal-related events connected with bone metastases from solid tumor and for the management of lytic lesion related to multiple myeloma.[3,4,5,6]
Oral BPs are used to treat osteoporosis,[7] osteopenia,[8] or other less common conditions such as Paget's disease and osteogenesis imperfecta.[9]
RANK ligand inhibitor (denosumab) is an antiresorptive medication that inhibits osteoclast function, decreases bone resorption, and increases bone density.[10,11] It is used in patients affected by osteoporosis or metastatic bone diseases.
Antiangiogenic medications hinder the development of novel blood vessels, blocking the angiogenesis-signaling cascade. They are basically divided into two types of drugs: Monoclonal antibodies that stop the receptor or growth factor (bevacizumab) and small molecules, which determine the block by binding the tyrosine kinase receptor (sunitinib and sorafenib). It has been hypothesized that they facilitate the other anticancer agents delivery.[12]
MRONJ pathophysiology is not completely elucidated.[13,14] There are several suggested hypothesis that could explain its unique localization to the jaws: Inflammation or infection, microtrauma, altered bone remodeling or over suppression of bone resorption, angiogenesis inhibition, soft tissue BPs toxicity, peculiar biofilm of the oral cavity, terminal vascularization of the mandible, suppression of immunity, or Vitamin D deficiency.[13,15,16,17,18]
Three risk factors such as local factors, underlying disease, and kind of medication [Table 2] should be considered. To explain the MRONJ disease frequency value, we have to consider two criteria: Therapeutic indications (osteoporosis/osteopenia and malignancy) and type of medication (BP and non-BP). The ONJ risk in patients treated with zolendronate is 50–100 times superior to individuals treated by placebo. The MRONJ risk in cancer patients treated by denosumab is similar to the possibility of ONJ in patients exposed to zolendronate.[13,19] As reported in Table 3, the risk of MRONJ is different on the basis of the medications and the administrations.[21,22,23,24,25,26,27] Even if the ONJ risk is similar, it is important to underline a substantial difference between BRONJ and DRONJ (denosumab-related ONJ). BRONJ occurs after a mean administration of 33 months (IV administration in cancer patients) or 48 months (oral administration in osteoporotic patients). DRONJ occurs early after treatment, independently of the number of previous administrations. Hence, ONJ risk after the use of RANK-L inhibitors decreases monthly while BP drugs remain stable for years. Risk of BRONJ is directly related to the duration of the therapy and total amount of the medication. Risk factors for MRONJ are reported in Table 2. Oral surgery is one of the greatest risk factors for MRONJ: According to several authors, 52–61% of patients reported tooth extraction as a precipitating event.[20,28] The risk of ONJ in patients treated by oral-BPs after a tooth extraction is 0.5%; ONJ risk in patients with cancer treated with IV BPs ranges from 1.6% to 14.8%.[29] MRONJ appears more frequently in the mandible (73%) compared to maxilla (22.5%); it involves both jaws in 4.5% of the cases.[28]
Table 2.
Medication-related osteonecrosis of the jaw risk factors
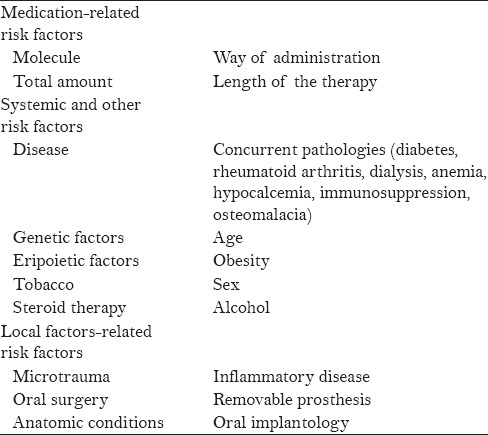
Table 3.
Osteonecrosis of the jaw risk (cases per 10,000 patients)

DEFINITION AND STAGING SYSTEMS
Patients are affected by MRONJ if all the following clinical manifestations are demonstrated:
Ongoing or antecedent treatment with antiangiogenic or antiresorptive drugs
No patient history of radiation therapy or manifest metastasis to the jaw
Exposed bone or presence of an intraoral or extraoral fistula in the maxillofacial region persisting for more than 8 weeks.[1]
However, many authors disagree with the last definition. Hence, the exposed necrotic bone in the oral cavity is just one of the possible manifestations of BRONJ, and it is not found in all patients. In 2012, the SICMF (Italian Society for Maxillofacial Surgery) and the SIPMO (Italian Society of Oral Pathology and Medicine) proposed a new definition:[30] “BRONJ is an adverse drug reaction described as the progressive destruction and death of bone that affects the mandible or maxilla of patients exposed to the treatment with nitrogen-containing BPs, in the absence of a previous radiation treatment.” It was supported by a study[31] on a large population of European patients. According to the AAOMS definition, just the 76% of the BRONJ were diagnosed; 24% remaining ONJ could not be diagnosed because of nonvisible necrotic bone.
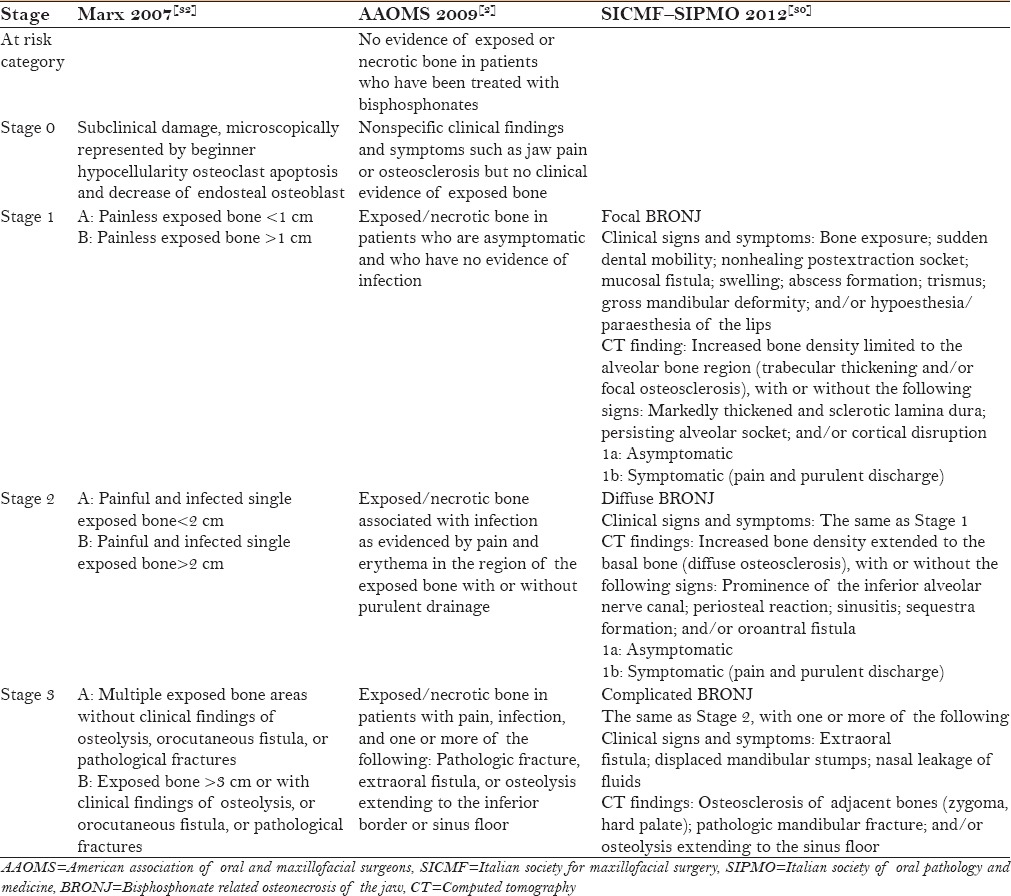
BRONJ staging systems are copious, and most of them are based on clinical findings: In 2006, Ruggiero et al.[16] proposed a clinical staging system with three different clinical levels based on signs and symptoms; in 2009, the AAOMSs implemented it with Stage 0.[2] Marx,[32] in 2007, was the only one who divided the stages on the basis of the lesion's size. Bedogni et al.,[30] in 2012, proposed a clinical-radiological staging system. Different BRONJ staging systems are given in Table 4.
Table 4.
Different bisphosphonate related osteonecrosis of the jaw staging systems
PREVENTION OF MEDICATION-RELATED OSTEONECROSIS OF THE JAW
Dental screening and adequate treatment are fundamental to reduce the risk of ONJ in patients under antiresorptive or antiangiogenic therapy or before initiating the administration.[28,33,34,35] The treatment of MRONJ is generally difficult, and the optimal therapy strategy is still to be established. For this reason, prevention is even more important. Several authors suggested a “drug holiday” before teeth extractions or other invasive procedures. However, there is no unanimous consensus on this treatment and not enough data to support the cessation of medical treatment in patients with osteoporosis. Currently, AAOMS considers appropriate drug holiday procedure as reported by Damm and Jones in “at risk” patients with extended exposure history (>4 years).[36] Even in cancer, individuals receiving IV therapy, there are limited data about the consequence of interrupting BPs IV administration before surgical procedures. If is allowed by patient conditions, the oncologist should consider to stop the therapy until the healing of soft tissue has occurred.[36] As part of a preventive approach, a distinction needs to be made between IV and oral therapy in patients under medical treatment or about to initiate it.
Cancer patients about to initiate intravenous medical treatment
Prior to the beginning of an IV medical treatment, the patient should always be carefully evaluated by a dentist. The main goals of preventive dental measures are to remove any oral infection, pathology, or risk factors in order to obtain a stable oral health situation, preventing the necessity for invasive dental procedures in the near or intermediate future.[37] Extraction of partially embedded teeth should be performed at this time. Embedded teeth completely covered by bone and soft tissue without any communication with the oral cavity should be left undisturbed.[38] Conservative endodontic and prosthodontic therapies of teeth with good prognosis should be completed. Periodontal stabilization splints for teeth with Grades 1–2 mobility in patients with good dental hygiene and extraction in patients with poor dental hygiene are necessary.[35,37] If allowed by general health conditions, the beginning of antiangiogenic or antiresorptive treatment should be deferred as far as oral status is stable or, at least, until the surgical site has mucosalized (2–3 weeks).[1]
Inadequate dentures should be modified, rebased, or replaced to decrease the oral tissue pressure and to prevent sore spots, especially along the lingual flange region or at the mandibular tori. Patients should achieve a proper oral hygiene and be educated to report any grief, inflammation, or bone exposure. Patients should be included in a periodic clinical-radiological follow-up, the frequency of which is based on the medical administration, the number of risk factors, and oral health status.
Asymptomatic cancer patients receiving intravenous medical treatment
It is essential that a detailed oral evaluation with regular check-ups every 4–6 months for exposed bone and “early stage” MRONJ diagnosis. An orthopantomography every 6–12 months for radiographic evidence of osteosclerosis or osteolysis, widened periodontal ligament spaces, or furcation involvements should be performed.[37] A good oral hygiene is essential to prevent dental infections that may require dentoalveolar surgery. Indeed, every invasive procedure that involves bone injury should be avoided. Nonrestorable teeth should be treated by removal of the crown and endodontic treatment of the remaining roots.[39] Teeth with mobility Grades 1–2 should be splinted rather than removed only in the absence of dental/periodontal lesions; extraction of teeth with mobility Grade 3 and/or endodontal-periodontal lesion it should be completed with the minimum bone injury and providing antibiotic treatment. An antibiotic prophylaxis for surgery procedures is necessary: Penicillin remains the first choice, in case of penicillin allergy, a combination of quinolones-metronidazole or erythromycin-metronidazole is a valuable alternative. Inadequate dentures should be modified, rebased, or replaced and in case of fixed prosthodontics, the biological width should be respected. Elective surgery and dental implants placement should be avoided.
Osteoporotic patients about to start oral medical treatment
Starting the therapy, patients should be instructed to the risk of developing MRONJ, especially if the treatment exceed beyond 4 years.[23] Informative and educational documents about the current knowledge of MRONJ as well as the instruction to quickly report every signs and symptoms should be given to patients. Periodic clinical-radiological follow-ups are recommended. The importance of oral hygiene and dental health should be underlined.[1] Implant placement is possible but a cautious approach is suggested. Data are limited, so an informed consent for a nonquantifiable risk of long term developing of MRONJ should be obtained.
Osteoporotic patients receiving oral medical treatment
The risk of developing MRONJ associated with oral BPs is very low, and it increases when the duration of therapy exceeded 4 years.[23] This period should be decreased in the case of comorbidities as well as antiangiogenic or chronic corticosteroid drugs.[28,35] However, the risk of MRONJ in patients treated with oral BPs is lower compared to subjects treated with IV medications. Elective dentoalveolar surgery is not contraindicated in these patients.
Patients treated with oral-aminobisphosphonate for <4 years without risk factors
No modification or delay of surgery is necessary, and all dental procedures are possible in this group. The importance of oral hygiene and dental health should be underlined.[1] Informative and educational documents about the current knowledge of MRONJ as well as the instruction to quickly report every signs and symptoms should be given to the patient.
Patients treated with oral-aminobisphosphonate for <4 years with risk factors or for >4 years
The patient should be motivated to achieve and maintain an optimal level of oral health.[1] A detailed oral evaluation with regular check-ups for exposed bone and “early stage” MRONJ diagnosis is suggested. An orthopantomography every 6–12 months for radiographic evidence of osteonecrosis should be performed. Teeth with mobility Grades 1–2 should be splinted whereas teeth with mobility Grade 3 should be extracted with minimum bone injury. An antibiotic prophylaxis for surgery procedures is necessary.[38] Inadequate dentures should be modified, rebased, or replaced and in case of fixed prosthodontics, the biological width should be respected. Endodontic procedures should be preferred to dental surgery. Implant placement is possible, but the patient should be informed about the possibility of short and long term loss of dental implants and ONJ risk.
TREATMENT OF MEDICATION-RELATED OSTEONECROSIS OF THE JAW
Treatment of ONJs is a demanding challenge for clinicians, and an effective and appropriate MRONJ therapy is still to be decided. It is suggested a multidisciplinary team approach including a dentist, an oncologist, and a maxillofacial surgeon to evaluate and decide the best therapy for patient. The choice between a conservative treatment and surgery is not easy, and it should be made on a case by case basis. However, the initial approach should be as conservative as possible. The most important goals of treatment for patients with established MRONJ are primarily the control of infection, bone necrosis progression and pain.[1]
At risk category
Patients are in this group if they have a treatment history with antiresorptive or antiangiogenic drugs. They do not need any treatment.[1] Anyway, they should be educated to the risk of developing MRONJ such as instructed to quickly report every signs and symptoms. Local risk factors management and periodical clinical and radiological check-ups are suggested.
Stage 0
A medical treatment (antiseptic, analgesic, antibiotic, and antiphlogistic therapy) and management of local risk factors are indicated.[1] Low-level laser therapy is a possible choice for treatment of osteonecrosis by helping reparative process, improving osteoblastic index, and stimulating lymphatic and blood capillaries growth.[39,40] A careful follow-up for the evolution to a greater stage is necessary.
Stage 1
If exposed and necrotic bone or fistulae are present, they are rinsed with antiseptic fluids and covered with an adhesive paste, 3 times a day. In the absence of healing tendency, after 8 weeks, it is possible for a surgical debridement approach.[41]
Stage 2
After 2 weeks of medical therapy to reduce inflammatory symptoms, a surgical debridement is indicated. It should be more conservative as possible but extended as large as necessary to a complete removal of affected bone.[41] Antibiotic and antiphlogistic treatments are administered. Follow-up examinations are necessary.
Stage 3
Marginal or segmental osteotomies are recommended for severe cases.[42,43,44,45,46] Invasive surgery is indicated only if it could improve patient's quality of life. In other cases or if patient rejects surgery, a conservative approach to control symptoms and to prevent the osteonecrosis progression is administered.[42]
CONCLUSION
The pathophysiology of MRONJ is not completely elucidated, and an effective and appropriate therapy is still to be decided. It is crucial in future to improve the current knowledge about MRONJ and develop better strategies for its prevention and treatment. Governments and institutions should stimulate and support future research in this direction.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest
REFERENCES
- 1.Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, Mehrotra B, et al. American Association of oral and maxillofacial surgeons position paper on medication-related osteonecrosis of the jaw – 2014 update. J Oral Maxillofac Surg. 2014;72:1938–56. doi: 10.1016/j.joms.2014.04.031. [DOI] [PubMed] [Google Scholar]
- 2.Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE, Mehrotra B. American Association of oral and maxillofacial surgeons position paper on bisphosphonate-related osteonecrosis of the jaws – 2009 update. J Oral Maxillofac Surg. 2009;67(5 Suppl):2–12. doi: 10.1016/j.joms.2009.01.009. [DOI] [PubMed] [Google Scholar]
- 3.Nussbaum SR, Younger J, Vandepol CJ, Gagel RF, Zubler MA, Chapman R, et al. Single-dose intravenous therapy with pamidronate for the treatment of hypercalcemia of malignancy: Comparison of 30-, 60-, and 90-mg dosages. Am J Med. 1993;95:297–304. doi: 10.1016/0002-9343(93)90282-t. [DOI] [PubMed] [Google Scholar]
- 4.Hortobagyi GN, Theriault RL, Lipton A, Porter L, Blayney D, Sinoff C, et al. Long-term prevention of skeletal complications of metastatic breast cancer with pamidronate. Protocol 19 Aredia Breast Cancer Study Group. J Clin Oncol. 1998;16:2038–44. doi: 10.1200/JCO.1998.16.6.2038. [DOI] [PubMed] [Google Scholar]
- 5.Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, et al. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J Natl Cancer Inst. 2004;96:879–82. doi: 10.1093/jnci/djh141. [DOI] [PubMed] [Google Scholar]
- 6.Berenson JR, Hillner BE, Kyle RA, Anderson K, Lipton A, Yee GC, et al. American society of clinical oncology clinical practice guidelines: The role of bisphosphonates in multiple myeloma. J Clin Oncol. 2002;20:3719–36. doi: 10.1200/JCO.2002.06.037. [DOI] [PubMed] [Google Scholar]
- 7.Delmas PD. The use of bisphosphonates in the treatment of osteoporosis. Curr Opin Rheumatol. 2005;17:462–6. doi: 10.1097/01.bor.0000163448.51661.87. [DOI] [PubMed] [Google Scholar]
- 8.Medical economics. Physicians' Desk Reference. 57th ed. Montvale, NJ: Medical Economics; 2003. [Google Scholar]
- 9.Delmas PD, Meunier PJ. The management of Paget's disease of bone. N Engl J Med. 1997;336:558–66. doi: 10.1056/NEJM199702203360807. [DOI] [PubMed] [Google Scholar]
- 10.Delmas PD. Clinical potential of RANKL inhibition for the management of postmenopausal osteoporosis and other metabolic bone diseases. J Clin Densitom. 2008;11:325–38. doi: 10.1016/j.jocd.2008.02.002. [DOI] [PubMed] [Google Scholar]
- 11.Fizazi K, Carducci M, Smith M, Damião R, Brown J, Karsh L, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: A randomised, double-blind study. Lancet. 2011;377:813–22. doi: 10.1016/S0140-6736(10)62344-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tenore G, Palaia G, Gaimari G, Brugnoletti O, Bove L, Lo Giudice R, et al. Medication-Related Osteonecrosis of the Jaws (MRONJ): Etiological update. Senses Sci. 2014;1:147–52. [Google Scholar]
- 13.Reid IR, Bolland MJ, Grey AB. Is bisphosphonate-associated osteonecrosis of the jaw caused by soft tissue toxicity? Bone. 2007;41:318–20. doi: 10.1016/j.bone.2007.04.196. [DOI] [PubMed] [Google Scholar]
- 14.Allen MR, Burr DB. The pathogenesis of bisphosphonate-related osteonecrosis of the jaw: So many hypotheses, so few data. J Oral Maxillofac Surg. 2009;67(5 Suppl):61–70. doi: 10.1016/j.joms.2009.01.007. [DOI] [PubMed] [Google Scholar]
- 15.Bamias A, Kastritis E, Bamia C, Moulopoulos LA, Melakopoulos I, Bozas G, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol. 2005;23:8580–7. doi: 10.1200/JCO.2005.02.8670. [DOI] [PubMed] [Google Scholar]
- 16.Ruggiero SL, Fantasia J, Carlson E. Bisphosphonate-related osteonecrosis of the jaw: Background and guidelines for diagnosis, staging and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:433–41. doi: 10.1016/j.tripleo.2006.06.004. [DOI] [PubMed] [Google Scholar]
- 17.Kos M, Junka A, Smutnicka D, Bartoszewicz M, Kurzynowski T, Gluza K. Pamidronate enhances bacterial adhesion to bone hydroxyapatite. Another puzzle in the pathology of bisphosphonate-related osteonecrosis of the jaw? J Oral Maxillofac Surg. 2013;71:1010–6. doi: 10.1016/j.joms.2012.12.005. [DOI] [PubMed] [Google Scholar]
- 18.Qi WX, Tang LN, He AN, Yao Y, Shen Z. Risk of osteonecrosis of the jaw in cancer patients receiving denosumab: A meta-analysis of seven randomized controlled trials. Int J Clin Oncol. 2014;19:403–10. doi: 10.1007/s10147-013-0561-6. [DOI] [PubMed] [Google Scholar]
- 19.Scagliotti GV, Hirsh V, Siena S, Henry DH, Woll PJ, Manegold C, et al. Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: Subgroup analysis from a randomized phase 3 study. J Thorac Oncol. 2012;7:1823–9. doi: 10.1097/JTO.0b013e31826aec2b. [DOI] [PubMed] [Google Scholar]
- 20.Vahtsevanos K, Kyrgidis A, Verrou E, Katodritou E, Triaridis S, Andreadis CG, et al. Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J Clin Oncol. 2009;27:5356–62. doi: 10.1200/JCO.2009.21.9584. [DOI] [PubMed] [Google Scholar]
- 21.Grbic JT, Black DM, Lyles KW, Reid DM, Orwoll E, McClung M, et al. The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: Data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc. 2010;141:1365–70. doi: 10.14219/jada.archive.2010.0082. [DOI] [PubMed] [Google Scholar]
- 22.Papapoulos S, Chapurlat R, Libanati C, Brandi ML, Brown JP, Czerwinski E, et al. Five years of denosumab exposure in women with postmenopausal osteoporosis: Results from the first two years of the FREEDOM extension. J Bone Miner Res. 2012;27:694–701. doi: 10.1002/jbmr.1479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lo JC, O'Ryan FS, Gordon NP, Yang J, Hui RL, Martin D, et al. Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure. J Oral Maxillofac Surg. 2010;68:243–53. doi: 10.1016/j.joms.2009.03.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mauri D, Valachis A, Polyzos IP, Polyzos NP, Kamposioras K, Pesce LL. Osteonecrosis of the jaw and use of bisphosphonates in adjuvant breast cancer treatment: A meta-analysis. Breast Cancer Res Treat. 2009;116:433–9. doi: 10.1007/s10549-009-0432-z. [DOI] [PubMed] [Google Scholar]
- 25.Qi WX, Tang LN, He AN, Yao Y, Shen Z. Risk of osteonecrosis of the jaw in cancer patients receiving denosumab: A meta-analysis of seven randomized controlled trials. Int J Clin Oncol. 2014;19(2):403–10. doi: 10.1007/s10147-013-0561-6. [DOI] [PubMed] [Google Scholar]
- 26.Coleman R, Woodward E, Brown J, Cameron D, Bell R, Dodwell D, et al. Safety of zoledronic acid and incidence of osteonecrosis of the jaw (ONJ) during adjuvant therapy in a randomised phase III trial (AZURE: BIG 01-04) for women with stage II/III breast cancer. Breast Cancer Res Treat. 2011;127:429–38. doi: 10.1007/s10549-011-1429-y. [DOI] [PubMed] [Google Scholar]
- 27.Guarneri V, Miles D, Robert N, Diéras V, Glaspy J, Smith I, et al. Bevacizumab and osteonecrosis of the jaw: Incidence and association with bisphosphonate therapy in three large prospective trials in advanced breast cancer. Breast Cancer Res Treat. 2010;122:181–8. doi: 10.1007/s10549-010-0866-3. [DOI] [PubMed] [Google Scholar]
- 28.Saad F, Brown JE, Van Poznak C, Ibrahim T, Stemmer SM, Stopeck AT, et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: Integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann Oncol. 2012;23:1341–7. doi: 10.1093/annonc/mdr435. [DOI] [PubMed] [Google Scholar]
- 29.Yamazaki T, Yamori M, Ishizaki T, Asai K, Goto K, Takahashi K, et al. Increased incidence of osteonecrosis of the jaw after tooth extraction in patients treated with bisphosphonates: A cohort study. Int J Oral Maxillofac Surg. 2012;41:1397–403. doi: 10.1016/j.ijom.2012.06.020. [DOI] [PubMed] [Google Scholar]
- 30.Bedogni A, Fusco V, Agrillo A, Campisi G. Learning from experience. Proposal of a refined definition and staging system for bisphosphonate-related osteonecrosis of the jaw (BRONJ) Oral Dis. 2012;18:621–3. doi: 10.1111/j.1601-0825.2012.01903.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fedele S, Bedogni G, Scoletta M, Favia G, Colella G, Agrillo A, et al. Up to a quarter of patients with osteonecrosis of the jaw associated with antiresorptive agents remain undiagnosed. Br J Oral Maxillofac Surg. 2015;53(1):13–7. doi: 10.1016/j.bjoms.2014.09.001. [DOI] [PubMed] [Google Scholar]
- 32.Marx RE. Oral and Intravenous Bisphosphonate-Induced Osteonecrosis of the Jaw. Chicago, Ill, USA: Quintessence; 2007. [Google Scholar]
- 33.Dimopoulos MA, Kastritis E, Bamia C, Melakopoulos I, Gika D, Roussou M, et al. Reduction of osteonecrosis of the jaw (ONJ) after implementation of preventive measures in patients with multiple myeloma treated with zoledronic acid. Ann Oncol. 2009;20:117–20. doi: 10.1093/annonc/mdn554. [DOI] [PubMed] [Google Scholar]
- 34.Ripamonti CI, Maniezzo M, Campa T, Fagnoni E, Brunelli C, Saibene G, et al. Decreased occurrence of osteonecrosis of the jaw after implementation of dental preventive measures in solid tumour patients with bone metastases treated with bisphosphonates. The experience of the National Cancer Institute of Milan. Ann Oncol. 2009;20:137–45. doi: 10.1093/annonc/mdn526. [DOI] [PubMed] [Google Scholar]
- 35.Vandone AM, Donadio M, Mozzati M, Ardine M, Polimeni MA, Beatrice S, et al. Impact of dental care in the prevention of bisphosphonate-associated osteonecrosis of the jaw: A single-center clinical experience. Ann Oncol. 2012;23:193–200. doi: 10.1093/annonc/mdr039. [DOI] [PubMed] [Google Scholar]
- 36.Damm DD, Jones DM. Bisphosphonate-related osteonecrosis of the jaws: A potential alternative to drug holidays. Gen Dent. 2013;61:33–8. [PubMed] [Google Scholar]
- 37.Hellstein JW, Adler RA, Edwards B, Jacobsen PL, Kalmar JR, Koka S, et al. Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis: Executive summary of recommendations from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2011;142:1243–51. doi: 10.14219/jada.archive.2011.0108. [DOI] [PubMed] [Google Scholar]
- 38.Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg. 2005;63:1567–75. doi: 10.1016/j.joms.2005.07.010. [DOI] [PubMed] [Google Scholar]
- 39.Endodontic Implication of Bisphosphonate-Associated Osteonecrosis of the Jaws. Chicago, IL: American Association of Endodontists; 2010. American Association of Endodontists; p. 4. [Google Scholar]
- 40.Scoletta M, Arduino PG, Reggio L, Dalmasso P, Mozzati M. Effect of low-level laser irradiation on bisphosphonate-induced osteonecrosis of the jaws: Preliminary results of a prospective study. Photomed Laser Surg. 2010;28:179–84. doi: 10.1089/pho.2009.2501. [DOI] [PubMed] [Google Scholar]
- 41.Romeo U, Galanakis A, Marias C, Vecchio AD, Tenore G, Palaia G, et al. Observation of pain control in patients with bisphosphonate-induced osteonecrosis using low level laser therapy: Preliminary results. Photomed Laser Surg. 2011;29:447–52. doi: 10.1089/pho.2010.2835. [DOI] [PubMed] [Google Scholar]
- 42.Rugani P, Acham S, Kirnbauer B, Truschnegg A, Obermayer-Pietsch B, Jakse N. Stage-related treatment concept of medication-related osteonecrosis of the jaw-a case series. Clin Oral Investig. 2015;19:1329–38. doi: 10.1007/s00784-014-1384-1. [DOI] [PubMed] [Google Scholar]
- 43.Carlson ER, Basile JD. The role of surgical resection in the management of bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2009;67(5 Suppl):85–95. doi: 10.1016/j.joms.2009.01.006. [DOI] [PubMed] [Google Scholar]
- 44.Brauner E, Guarino G, Jamshir S, Papi P, Valentini V, Pompa V, et al. Evaluation of highly porous dental implants in postablative oral and maxillofacial cancer patients: A prospective pilot clinical case series report. Implant Dent. 2015;24:631–7. doi: 10.1097/ID.0000000000000295. [DOI] [PubMed] [Google Scholar]
- 45.Seth R, Futran ND, Alam DS, Knott PD. Outcomes of vascularized bone graft reconstruction of the mandible in bisphosphonate-related osteonecrosis of the jaws. Laryngoscope. 2010;120:2165–71. doi: 10.1002/lary.21062. [DOI] [PubMed] [Google Scholar]
- 46.Pompa G, Bignozzi I, Cristalli MP, Quaranta A, Di Carlo S. Bisphosphonates and Osteonecrosis of the jaw: The oral surgeon's perspective. Eur J Inflamm. 2012;101:11–23. [Google Scholar]